
Introduction
The heart and the kidney share a complex interdependence on many levels. Consequently, the association of simultaneous heart and renal dysfunction is very common and has been termed ‘cardio-renal syndrome’ (CRS) (Table 1). The majority of patients who have advanced chronic kidney disease (CKD) will die from cardiac causes; this may be even more common than reaching dialysis. Conversely, patients with cardiac disease who have concomitant CKD have poorer outcomes.1
Unfortunately, the majority of seminal chronic heart failure (CHF) studies have excluded patients with significant CKD. Also, many of the medications used in CHF are themselves potentially nephrotoxic, mandating careful collaboration between cardiology and nephrology teams. In this article, we focus on the management of patients with end-stage CHF in whom CKD is evident at the outset or develops after CHF-focussed interventions. We also briefly highlight how ‘renal’ interventions (eg ultrafiltration) can help in the management of CHF with CKD.
Epidemiology of chronic heart failure and chronic kidney disease
Chronic heart failure affects approximately 1–2% of the adult population in developed countries, with increasing prevalence (≥10%) in patients over the age of 70 years.2 It includes both those with preserved and those with reduced ejection fraction,3 but here we will only consider the management of the latter.
Renal dysfunction is common in patients with CHF. One study found that 33% of CHF patients with New York Heart Association (NYHA) class III and IV symptoms had severely impaired renal function (creatinine clearance <30 ml/min).4
Baseline renal function is just as important a prognostic marker as ejection fraction or NYHA class. For each 1 ml/min decrease in creatinine clearance there is a 1% increase in mortality.4 This is important as some CHF interventions reduce creatinine clearance by >10 ml/min.
Pathophysiology of cardio-renal syndrome type 2 focussing on coincident chronic kidney disease
This article will focus predominantly on CRS type 2 (see Table 1), which involves CHF that leads either to new onset CKD or to the progression of existing CKD, as defined by the Acute Dialysis Quality Initiative (ADQI).5,6
Cardiorenal syndrome classification.
The pathophysiology behind the development of CRS type 2 is not fully understood and is beyond the scope of this article (Fig 1),7 but chronic over-activity of the sympathetic and renin-angiotensin aldosterone systems is prominent in these CHF and CKD patients.
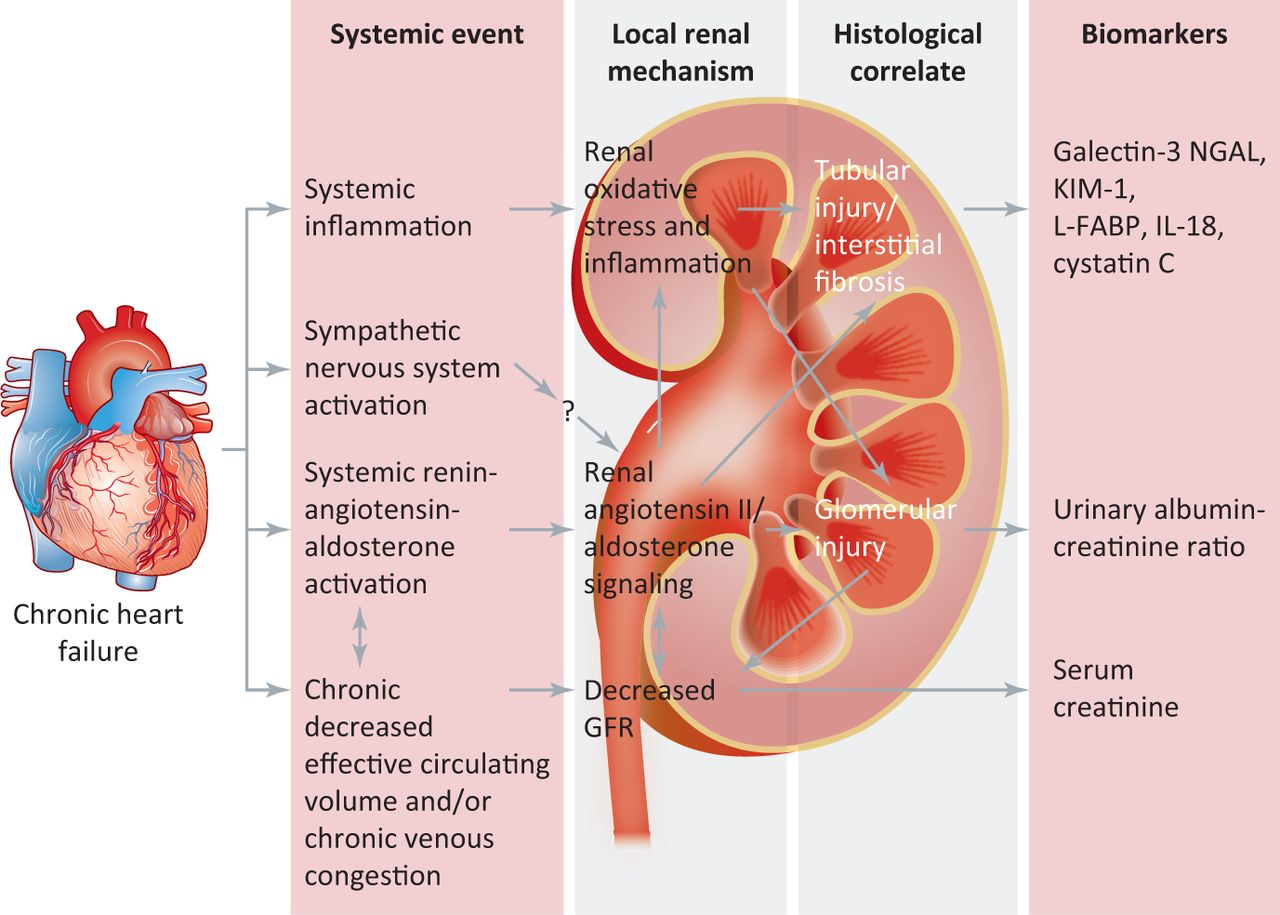
An overview of the key pathophysiology underlying the development of cardiorenal syndrome type 2.7 GFR = glomerular filtration rate; IL= interleukin; KIM = kidney injury molecule; L-FABP = liver-type fatty acid-binding protein; NGAL = neutrophil gelatinase-associated lipocalin.
Management of chronic heart failure with chronic kidney disease
Patients who have co-existing CHF and CKD are particularly challenging to treat. Earlier intervention, frequent monitoring of renal function and serum potassium and timely communication between specialties are mandatory and key.
There is an urgent need for the development of novel biomarkers of acute kidney injury (eg neutrophil gelatinase-associated lipocalin or cystatin C) and also of CHF that are not affected by CKD, enabling us to identify and to classify patients earlier.8,9 Brain natriuretic peptide (BNP) and NT-proBNP (the N-terminal prohormone of BNP), although still diagnostically useful in CHF, are partly excreted by the kidneys thereby reducing their specificity as a marker of CHF.10
Primary prevention
Lifestyle measures, such as increasing physical activity, smoking cessation, healthy diet, weight loss and blood pressure and cholesterol control are equally important in both renal and cardiac disease, which share many common underlying comorbidites, including age, hypertension, dyslipidaemia, smoking and diabetes mellitus.11
Secondary prevention
The role of beta-blockers, angiotensin converting enzyme inhibitors (ACEi) or angiotensin receptor blockers (ARB), and mineralocorticoid receptors (MRA) in the management of CHF is well established and is covered elsewhere.3,12 Theoretically, these drugs may prove helpful in addressing two key elements in the pathophysiology of CRS type 2: the chronic overactivity of the sympathetic and renin-angiotensin aldosterone systems, both of which adversely affect the heart and kidneys.5
Managing renal function while using chronic heart failure therapies
Renal function (eGFR) and serum potassium should be checked before initiating ACEi, ARB or MRA therapy, and repeated after 1–2 weeks of treatment and after each change in dose,3,12,13 with routine monitoring every 4 months in stable patients.3
‘Caution or specialist advice’ is advised in patients who have significant renal dysfunction (defined as a creatinine level of ≥221 μmol/l or estimated glomerular filtration rate [eGFR] <30 ml/min/1.73 m2 CKD stage IV), reflecting the exclusion criteria for many of the key trials in CHF management.3 This does not equate to withholding treatment: these patients in any case should be under shared care with nephrology.
Combined hydralazine and isosorbide dinitrate is an alternative first-line treatment for those who are ‘unable to tolerate’ an ACEi or ARB,3,12 but this combination does not directly address ongoing albuminuria, neither does it necessarily prevent further decline in renal function. There is increasing evidence to demonstrate both renal and cardiac benefits of ACEi or ARB therapy down to stage 5 CKD (including dialysis patients).14–16 The degree of initial renal impairment should not be seen as an absolute contraindication to ACEi, ARB or MRA therapy, but should reinforce the need for frequent review of the patient, their results and interdisciplinary communication.
A modest decline in renal function can be expected upon initiation of treatment with an ACEi, ARB or MRA as the result of haemodynamic reduction in intraglomerular pressure. (See Table 2 for ‘expected’ changes in renal function.)3,13,17–24 In these circumstances, the dose should not be modified but the renal function rechecked in 2 weeks.3,13
The safety of accepting these ‘modest’ changes in glomerular filtration rate has been shown by Bakris et al, who illustrated that an acute rise in creatinine of up to 30% that stabilised within the first 2 months of ACEi therapy was associated with preservation of renal function in the longer term.21 But this may not apply to older patients or to those with CKD stage IV and worse. This seems likely to apply also to ARB and MRA therapy. Patients with a serum creatinine level of >124 μmol/l at the time of ACEi initiation also demonstrated a 55–75% risk reduction for renal disease progression, compared to those with normal renal function.21
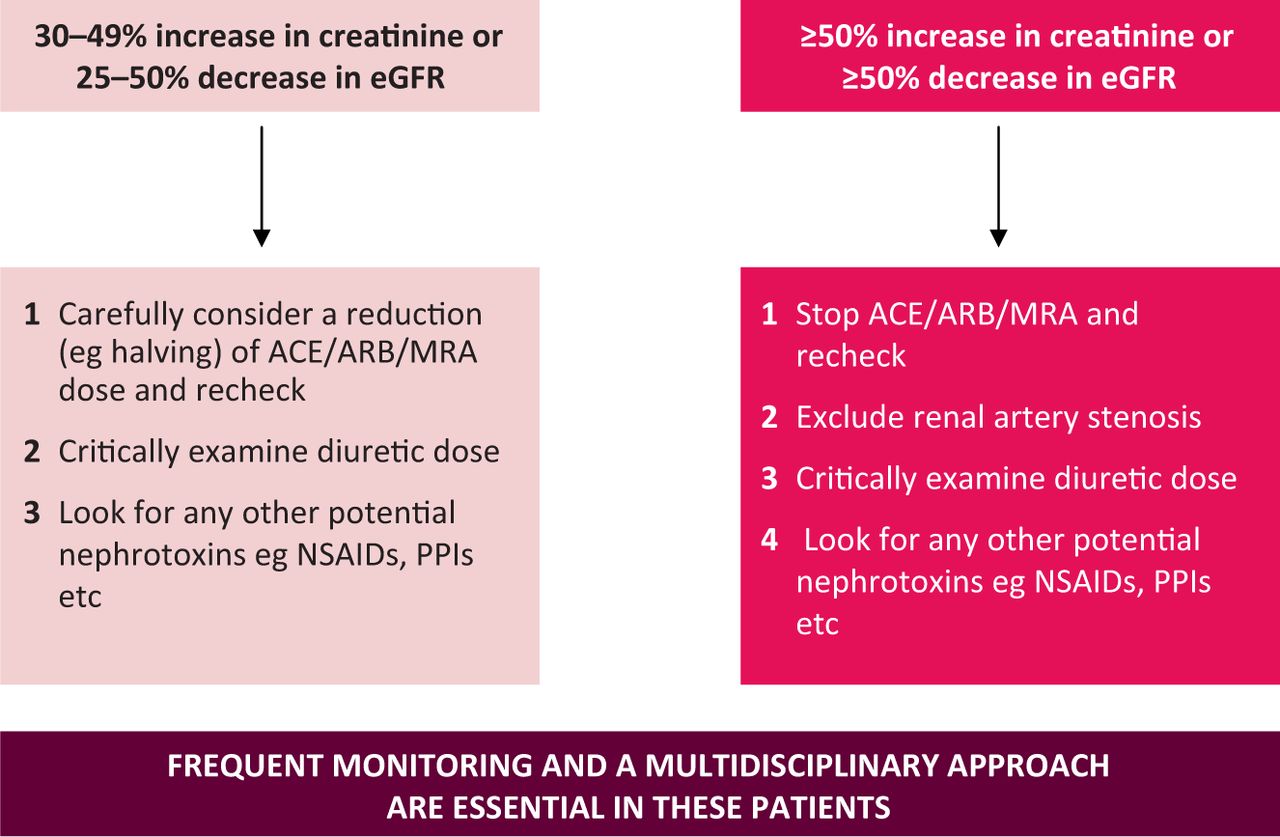
What is less certain is what we should do if the renal function deteriorates beyond these parameters. We suggest the algorithm shown in Fig 2.

Suggested algorithm for the management of patients with deteriorating renal function who are on ACE inhibitors, angiotensin receptor blockers or mineralocorticoid receptor antagonists. ACE = angiotensin converting enzyme; ARB = angiotensin receptor blocker; eGFR = estimated glomerular filtration rate; MRA = mineralocorticoid receptor antagonist; NSAIDS = non-steroidal anti-inflammatory drugs; PPIs = proton pump inhibitors.
A review of randomised control trial data from Phillips et al revealed that a combination of ARB and ACEi significantly worsened renal function over control (either ACEi alone or placebo) with a relative risk of 2.17.25 There was also a significant increase in the risk of hyperkalaemia (serum potassium ≥5.5 mEq/l) with the combination (relative risk 4.87).25 Although this combination is no longer recommended as first-line treatment for heart failure patients who have persisting symptoms, despite optimal ACEi or ARB and beta-blocker treatments, it illustrates the potential risks of combination therapy, as beta-blockers can also cause serum potassium elevation.3
Managing serum potassium while using chronic heart failure therapies
If serum potassium is >5.0 mmol/l, an ACEi, ARB or MRA should not be started immediately.3,12 Possible causes of hyperkalaemia should be addressed in the first instance; for example, high potassium diet, potassium supplementation, overdosing or potassium-retaining medication (eg amiloride) may be the cause, so restricting potassium intake by these means may allow continued administration of therapy.
See Table 2 for expected changes in serum potassium with CHF therapy and note that the increase seen with ARB therapy is generally slightly less than that for ACEi. It is important to appreciate that the low prevalence of ‘significant hyperkalaemia’ quoted for MRA therapy is likely to reflect the studies' exclusion criteria (potassium >5 mmol/l) and the regular monitoring the patients underwent; this low prevalence may not, therefore, be representative of the reality found in clinical practice.
The European Society of Cardiology (ESC) advise that an increase in potassium of up to 5.5 mmol/l with ACEi and ARB therapy is acceptable and should be monitored; if potassium increases beyond this, then these drugs should be stopped.3 NICE suggest that a higher potassium threshold of <6 mmol/l is acceptable before stopping.13 With MRA therapy, should the potassium rise to >5.5 mmol/l, the dose should be halved and the drug should be stopped altogether were potassium to rise to >6.0 mmol/l.3
Beta-blockers suppress renin synthesis and can thus worsen hyperkalaemia. They have been shown to augment the rise in potassium seen with supplementation by 30% and to prolong this elevation.26
As important as any ‘threshold’ serum potassium concentration is, the speed with which the threshold has been approached and then exceeded. Many CKD patients can tolerate long-term serum potassium concentrations of 5.5–6.0 mmol/l without incident. If the serum potassium is >6 mmol/l, a discussion with the local nephrology team would be prudent.
Acidosis is common in CKD. It can hasten long-term decline in glomerular filtration rate and exacerbate hyperkalaemia, so use of sodium bicarbonate (500–1000 mg twice daily) can help temper hyperkalaemia, without significant adverse ‘volume’ effect.
Ultrafiltration
Dialysis and haemofiltration are both effective means of fluid removal in patients with CRS. Standard haemodialysis can have a significant haemodynamic impact, but (intermittent) ultrafiltration and peritoneal dialysis may be suitable alternatives for unstable CHF patients.
Evidence from the UNLOAD trial suggests that the selected use of ultrafiltration may safely enable greater fluid loss than can be achieved using intravenous diuretics, with fewer readmissions due to fluid reaccumulation at 90 days.27 One small study of 17 patients with refractory congestive heart failure suggested that peritoneal dialysis improved NYHA functional class at 1 year, as well as reducing hospital admissions.28 Further studies are clearly and urgently needed in this area.
Key points
Despite the prevalence of renal impairment in patients with chronic heart failure and the significant negative impact on prognosis that it conveys, there is limited evidence available to guide the management of cardiorenal syndromes
There is an urgent need for novel biomarkers and new studies regarding the management of cardiorenal syndromes
At present, the key to managing these patients is frequent monitoring of both serum potassium and renal function, with close liaison between cardiology and nephrology
There is increasing interest in the role of ultrafiltration and peritoneal dialysis in the management of acute and chronic heart failure, respectively, but outcome evidence is currently lacking
Kidney failure complications become more severe and more common in chronic kidney disease stage IV, so all patients should be referred to/disclosed with the local renal team
- © 2013 Royal College of Physicians
References








{kind=link}
{kind=link}
Jump to section
- Article
- Introduction
- Epidemiology of chronic heart failure and chronic kidney disease
- Pathophysiology of cardio-renal syndrome type 2 focussing on coincident chronic kidney disease
- Management of chronic heart failure with chronic kidney disease
- Managing renal function while using chronic heart failure therapies
- Managing serum potassium while using chronic heart failure therapies
- Ultrafiltration
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.