
ABSTRACT
Cardiovascular magnetic resonance (CMR) is a noninvasive imaging tool with high spatial resolution in the absence of ionising radiation. CMR imaging is routine in the functional assessment of coronary lesions and is widely held as the gold standard in myocardial viability imaging. Its unique tissue characterisation capabilities have revolutionised the assessment of the cardiomyopathies and it is the investigation of choice for cardiovascular surveillance imaging. To date its greatest success has been in the management of thalassaemia major, where the ability to detect myocardial iron loading has significantly improved patient survival.
In the near future, CMR fibrosis imaging may serve as a risk stratification tool for the cardiomyopathies; and the ability to assess interstitial fibrosis may advance this role into other disease processes. Novel methods of tissue characterisation and emerging technical advances present new avenues for this modality, securing its place as the noninvasive imaging tool of the future.
- Cardiovascular magnetic resonance
- coronary lesions
- myocardial viability imaging
- cardiomyopathies
- thalassaemia major
- interstitial fibrosis.
Introduction
Cardiovascular magnetic resonance (CMR) is a clinically established, non-invasive imaging technique that has become the standard reference for assessing several aspects of cardiac structure and function. Technical advances have led to a rapid expansion in clinical indications and the number of scans performed per centre is steadily growing in the UK.1 Here, we discuss the contemporary applications of CMR and its emerging roles for future use.
Contemporary CMR
Myocardial iron overload
One of the most profound CMR successes is in the management of thalassaemia major. Until recently, cardiac failure resulting from transfusion iron overload was the most common cause of premature death. However, conventional serum ferritin and liver iron concentrations poorly predict cardiac iron content. CMR T2*, a relaxation parameter arising from field inhomogeneities resulting from the presence of particulate iron, quantifies myocardial iron and predicts progression to heart failure.2 The use of this parameter to guide iron chelation has been associated with a 71% reduction in heart failure deaths in the UK3 (Fig 1). As a readily measurable outcome, T2* has also greatly facilitated clinical trials of novel chelation agents, with further improvements in clinical care.4
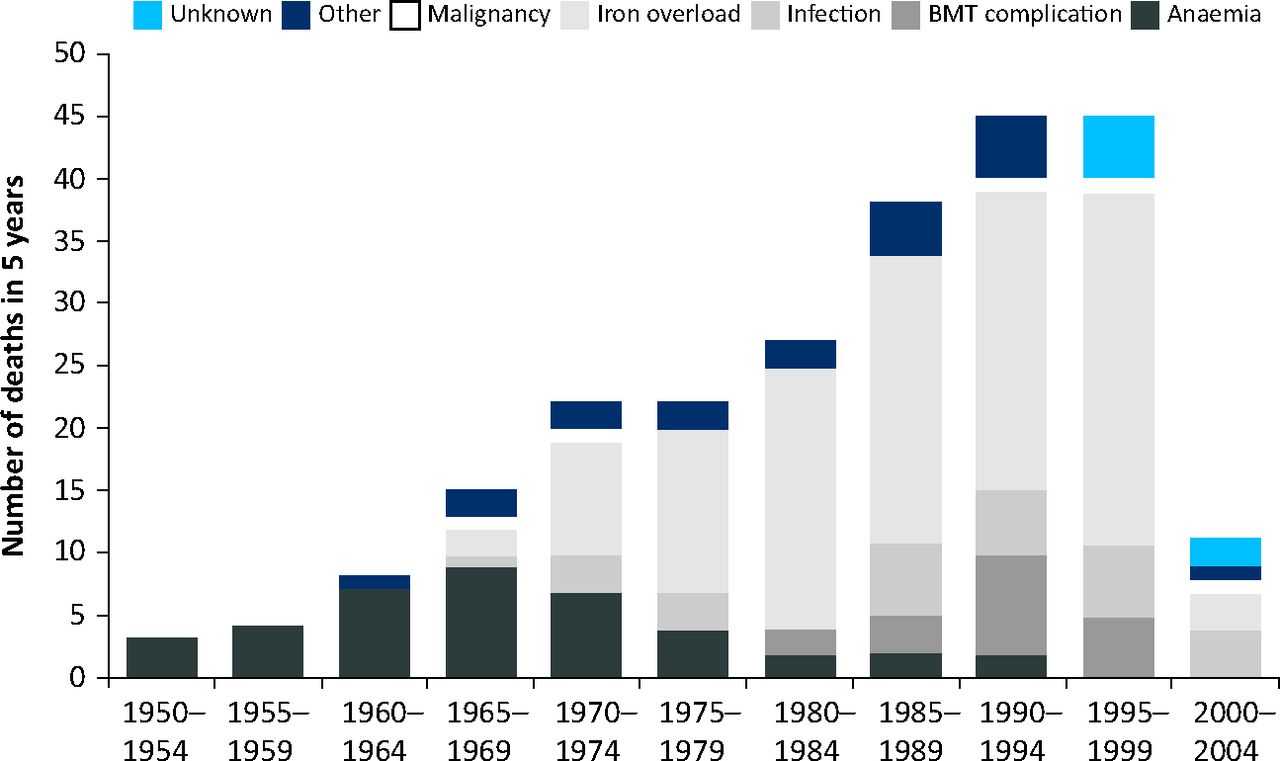
Number of deaths of patients with thalassaemia major in the UK by intervals. The number of deaths in the 2000–2003 interval represents deaths during 4 years and, in all the other groups, the number of deaths is over 5 years. In 1999, cardiovascular magnetic resonance (CMR) T2* was introduced in the UK and utilised to guide patient's iron chelation therapy. There has been a 71% reduction in the annualised death rate from iron overload since 2000. Reproduced with permission from Modell et al (2008).3
Coronary artery disease
In current practice, non-invasive imaging is utilised to risk stratify patients with ischaemic symptoms; to determine the functional significance of established coronary disease; and to assess myocardial viability after myocardial infarction (MI). Together these remain the most common indications for CMR in Europe.5
Myocardial viability assessment with late gadolinium enhancement (LGE) is widely considered the in vivo gold standard.6 The high spatial resolution of CMR enables the detection of small or subendocardial MIs (Fig 2), whereas the transmural extent of LGE predicts myocardial functional recovery following revascularisation.7 In the context of a recent MI, a contrast-free core within an area of LGE is interpreted as microvascular occlusion and is predictive of a poor prognosis.8
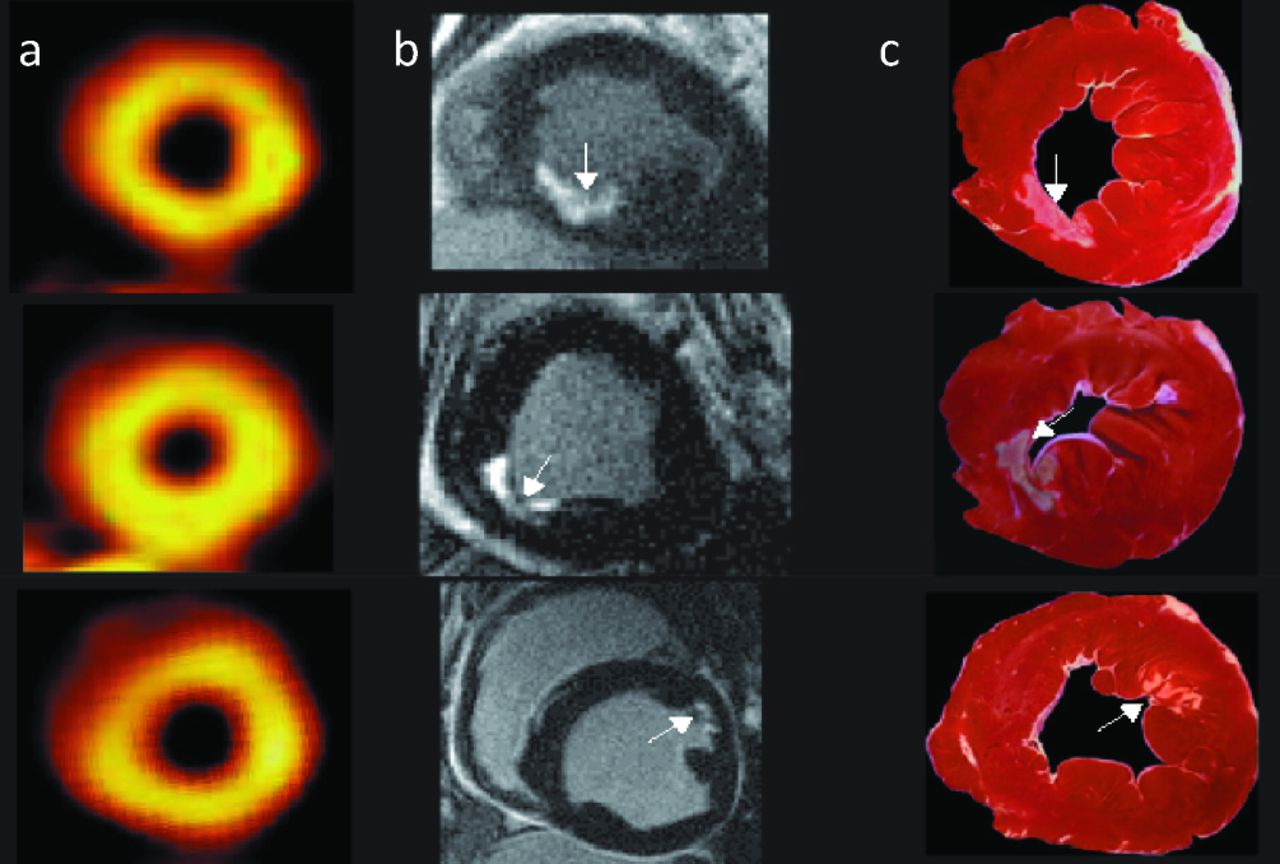
Short axis views from three dogs with subendocardial infarcts. (a) Single-photon emission computed tomography (SPECT) analysis, (b) late gadolinium enhancement (LGE) image and (c) histological analysis in with fibrosis staining. LGE correctly detects the subendocardial infarcts in all three cases, whereas SPECT does not. Reproduced with permission from Wagner et al (2003).39
Stress perfusion CMR follows the first pass of an intravenous gadolinium bolus through the myocardium at rest and during adenosine stress. The superior spatial and temporal resolution of CMR results in high accuracy for detecting myocardial ischaemia.9 This has enabled the detection of subendocardial hypoperfusion associated with microvascular ischaemia.10 In suspected coronary artery disease, the CE-MARC trial demonstrated that CMR had diagnostic superiority over single-photon emission computed tomography (SPECT), without the disadvantage of radiation exposure.11 New high field-strength scanners promise to reduce image artefacts and further improve diagnostic accuracy.
Non-ischaemic cardiomyopathies
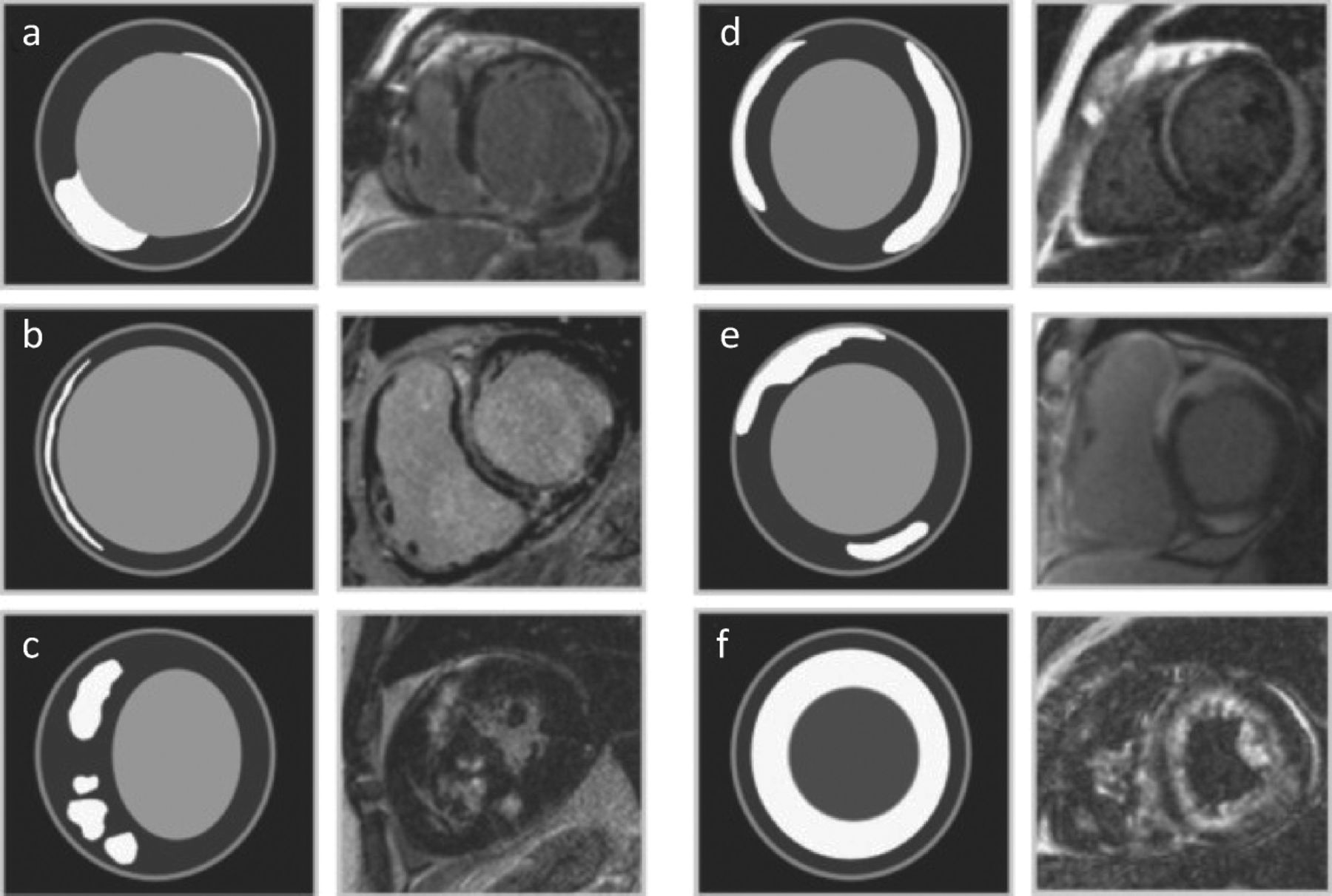
The unique tissue characterisation capabilities of CMR have revolutionised the management of the cardiomyopathies. LGE imaging has led to the recognition of relatively specific patterns of enhancement, with a direct impact on patient management (Fig 3).12 For example, a combination of CMR-detected tissue abnormalities has a diagnostic accuracy for cardiac amyloid of 97%.13
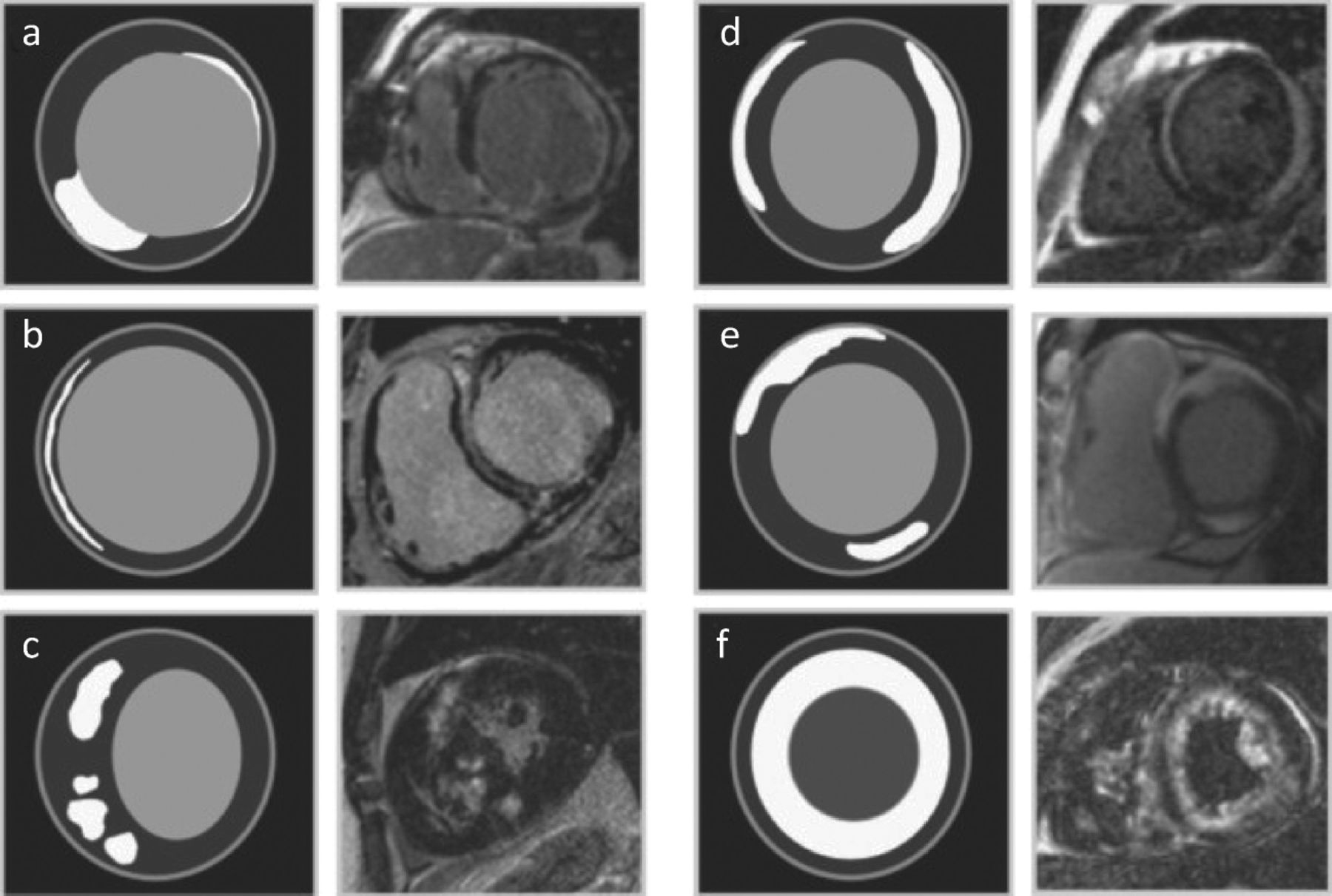
Schematic of typical late gadolinium enhancement (LGE) patterns in patients with ischaemic and non-ischaemic cardiomyopathy. (a) Ischemic cardiomyopathy: patient with transmural inferoseptal LGE and non-transmural lateral wall LGE representing infarctions of the right coronary artery and circumflex territories. (b) Dilated cardiomyopathy: patient with mid-wall LGE throughout the interventricular septum. (c) Hypertrophic cardiomyopathy: patchy mid-wall LGE within the hypertrophied septal wall segments. (d) Viral myocarditis: epicardial-based LGE in the anteroseptal and inferolateral walls. (e) Sarcoidosis: dense epicardial-based LGE of the anteroseptal and inferior walls. This case also shows right ventricular involvement. (f) Amyloidosis: diffuse to global, subendocardial to epicardial LGE involving both the left and the right ventricle. Reproduced with permission from Stirrat et al (2013).12
Dilated cardiomyopathy
CMR patterns of myocardial LGE can assist in the aetiological assessment of patients with heart failure. The identification of subendocardial LGE, despite normal coronary arteries at angiography, is suggestive of prior MI with vessel recanalisation. In contrast, luminal stenosis in the absence in LGE points towards a diagnosis of dilated cardiomyopathy (DCM) with bystander coronary disease. A mid-wall distribution of LGE is recognised in approximately a third of patients with DCM and is consistent with histological descriptions of myocardial fibrosis.14
Hypertrophic cardiomyopathy
Enhanced border definition has improved regional left ventricular hypertrophy quantification in patients with hypertrophic cardiomyopathy (HCM), including the detection of apical hypertrophy, an abnormality often missed by echocardiography. Patchy LGE, most often within the area of maximal hypertrophy, is recognised in up to 80% cases15 and assists in differentiation from other aetiologies of hypertrophy.
Arrhythmogenic right ventricular cardiomyopathy
The difficulty in establishing this diagnosis is reflected in the complex multicomponent ‘Modified Task Force Criteria’. The ability of CMR to provide an accurate assessment of right ventricular size and function underpins its inclusion in these diagnostic criteria. Although accurately making or excluding an arrhythmogenic right ventricular cardiomyopathy (ARVC) diagnosis remains difficult, the use of CMR has been shown to increase significantly the sensitivity of the Modified Task Force Criteria.16
Myocarditis
Myocarditis is another of the cardiomyopathies for which CMR has had a revolutionary impact. Myocardial oedema imaging with short TI inversion recovery (STIR); early-phase gadolinium enhancement; and LGE have made it possible to identify areas of myocardial inflammation non-invasively for the first time. Many cases of myocarditis were previously incorrectly diagnosed as ischaemic events;17 the use of CMR may therefore prevent many patients from receiving costly and potentially dangerous treatments for coronary disease. CMR diagnostic criteria have been proposed but further validation remains necessary.18
Adult congenital heart disease
Advances in surgical techniques have led to a steady increase in the number of patients with congenital heart disease surviving to adulthood. Patients have complex anatomy requiring lifelong follow-up in which CMR has established a key role. Multiplanar imaging of vascular anatomy with velocity flow mapping and contrast angiography can be repeatedly performed in the absence of ionising radiation. In adults with congenital heart disease (ACHD), CMR evaluation of right ventricular anatomy and function, a crucial assessment in this field, has advantages over echocardiography in light of the superior resolution and reproducibility. This, combined with the evaluation of fibrosis with LGE imaging, enables CMR to contribute to decision-making regarding interventions.
Future directions
The future of CMR is lies in the clinical validation of current techniques, outcome studies using established parameters; and the development of new technologies with the potential to offer new insights into cardiovascular disease processes.
Near future
Risk stratification in DCM
The prognosis of patients with DCM remains poor owing to progressive heart failure and arrhythmic sudden death, with 5-year mortality as high as 20%.19 Implantation of a cardiac defibrillator can improve survival;20 quantification of a patient's risk of life-threatening arrhythmias is therefore a key component of management.
Contemporary practices, which rely heavily on assessment of left ventricular systolic function, can underestimate risk in those with mild or moderate systolic impairment. Recent reports demonstrate that mid-wall LGE is an independent risk factor for all-cause mortality, cardiovascular death and sudden death (Fig 4). The inclusion of mid-wall LGE into assessment algorithms has been shown to improve risk stratification regardless of the ejection fraction.22
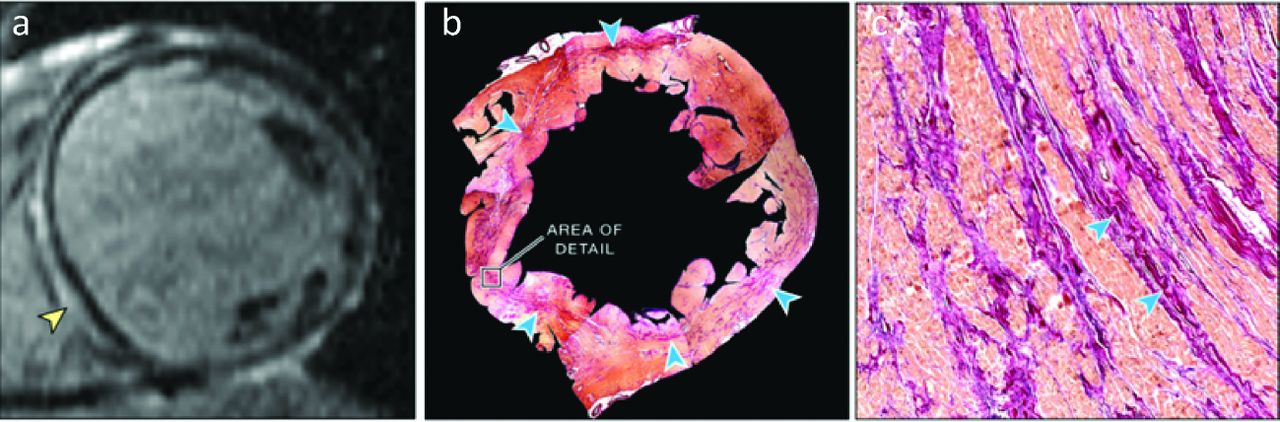
Patient with midwall fibrosis who experienced sudden cardiac death. (a) Pre-mortem late gadolinium enhancement (LGE)-cardiovascular magnetic resonance (CMR) demonstrated a near-circumferential pattern of mid-wall LGE (yellow arrow) at mid-ventricular level. (b) Picrosirius red staining in the corresponding post-mortem macroscopic short-axis section revealed a prominent linear band of collagen (blue arrows), which mirrors the distribution of LGE on CMR. (c) Microscopic examination confirmed the presence of extensive replacement fibrosis (blue arrows) in an area of staining seen on the macroscopic section (area of detail in (b)); magnification × 300. Reproduced with permission from Gulati et al (2013).22
Risk stratification in HCM
HCM is a relatively common inherited cardiomyopathy, affecting approximately 1 in 500 of the population.23 Despite a benign clinical course in many patients, an important subset are at risk of disabling symptoms, arrhythmic sudden death, thromboembolic disease and progressive left ventricular impairment. As with DCM, contemporary risk prediction algorithms are limited and recent research also suggests that LGE imaging provides additional, prognostically useful information.
Histological studies have established that LGE correlates with regions of myocardial interstitial fibrosis in HCM.24 The extent of LGE is greater in patients with progressive disease and with conventional risk factors for sudden death.25 The presence of LGE can predict cardiovascular events such as ventricular tachycardia, and, in a recent meta-analysis, was found to correlate with a composite outcome of cardiovascular and all-cause mortality.27 Future research will need to dissect out how these findings relate to the aetiology of the heart muscle disease, how and if LGE predicts disease complications and ultimately determine whether CMR can help improve patient outcomes.
Interstitial fibrosis quantification by T1 mapping
Myocardial fibrosis, with expansion of the interstitial space, is the final common pathway in several cardiovascular diseases. Whereas macroscopic areas of focal fibrosis can be identified by LGE, diffuse fibrosis is undetected by this technique. T1 is a magnetic resonance parameter with tissue-specific characteristics; an increase in myocardial T1 is detected in many cardiovascular disease processes. Cardiac T1 ‘mapping’ is a rapidly developing technique that measures T1 values of the entire heart. Histological validation against myocardial biopsies demonstrates that post-contrast T1 mapping closely correlates with the degree of interstitial fibrosis,28 with evidence of disease-specific variability. The reproducibility and reliability of pre- and post-contrast imaging techniques have been established and a range of normal values in vivo have now been published.29 The future is promising for this technique, which could improve understanding of the natural history of cardiovascular pathologies and pave the way for disease-modifying interventions.
Not so near future
Diffusion tensor imaging
Diffusion tensor imaging (DTI) is an established magnetic resonance technique for imaging tissue fibre architecture. Diffusion-based techniques exploit the ability to detect MR signal changes due to the diffusion of water molecules in a magnetic field, which occurs preferentially in parallel to the long axis of cells or fibres. Histological studies demonstrate that, in health, the long axis of cardiac myocytes is aligned in gradually changing orientations between the epicardium and endocardium.30 The loss of integrity of this architecture is seen in diseases such as HCM, where myocardial disarray has been demonstrated histologically. Ex vivo DTI studies of healthy and diseased myocardium demonstrate an association between DTI findings and histological fibre orientation.31 Formidable technical challenges remain, not least because of difficulties in detecting and quantifying microscopic magnitudes of diffusion in a moving target organ, consequently there is a paucity of in vivo cardiac data. Recent technological developments in CMR sequence design, combined with high-field strength (3 Tesla) scanners, have rendered it feasible to acquire in vivo human, cardiac DTI data for the first time. Images depicting the progression of fibre orientation through the myocardium dramatically demonstrate the potential of this technique (Fig 5), and numerous clinical applications have already been proposed. clinical applications have already been proposed. Early reproducibility data from healthy volunteers,32 and in hypertrophic cardiomyopathy33 have been encouraging and technological development continues at pace.

Diffusion tensor imaging (DTI) tractography of the heart in vivo at end diastole (a,c) and end-systole (b,d). Fibre tracts are viewed from their subepicardial (a,b) and subendocardial surfaces (c,d) and are colour coded by their median helix angle. Fibre tracts in the subepicardium at end systole become more oblique (red) as the myocardium contracts. However, at end diastole, as the left ventricular outer circumference expands, the subepicardial fibres assume a more right-handed (less oblique) orientation. Reproduced, with permission from Nielles-Vallespin et al (2002).32
Further into the future
Interventional CMR
Although the spatial and temporal resolution of CMR is inferior to that of X-ray techniques, interventional CMR offers many advantages, including adjustable soft tissue contrasting and rapid multiplanar imaging with a 3D display. Catheter-derived signals from embedded receiver coils can be displayed in colour against the grey-scale myocardium and gadolinium contrast can be used to highlight the position of inflatable devices. Other potential features include automated image plane selection in response to catheter movement. The lack of ionising radiation makes this technique particularly attractive for paediatric interventions and, to date, has been successfully used to perform several interventional procedures in animal models34 and select procedures in humans.35
Carbon-13 hyperpolarisation
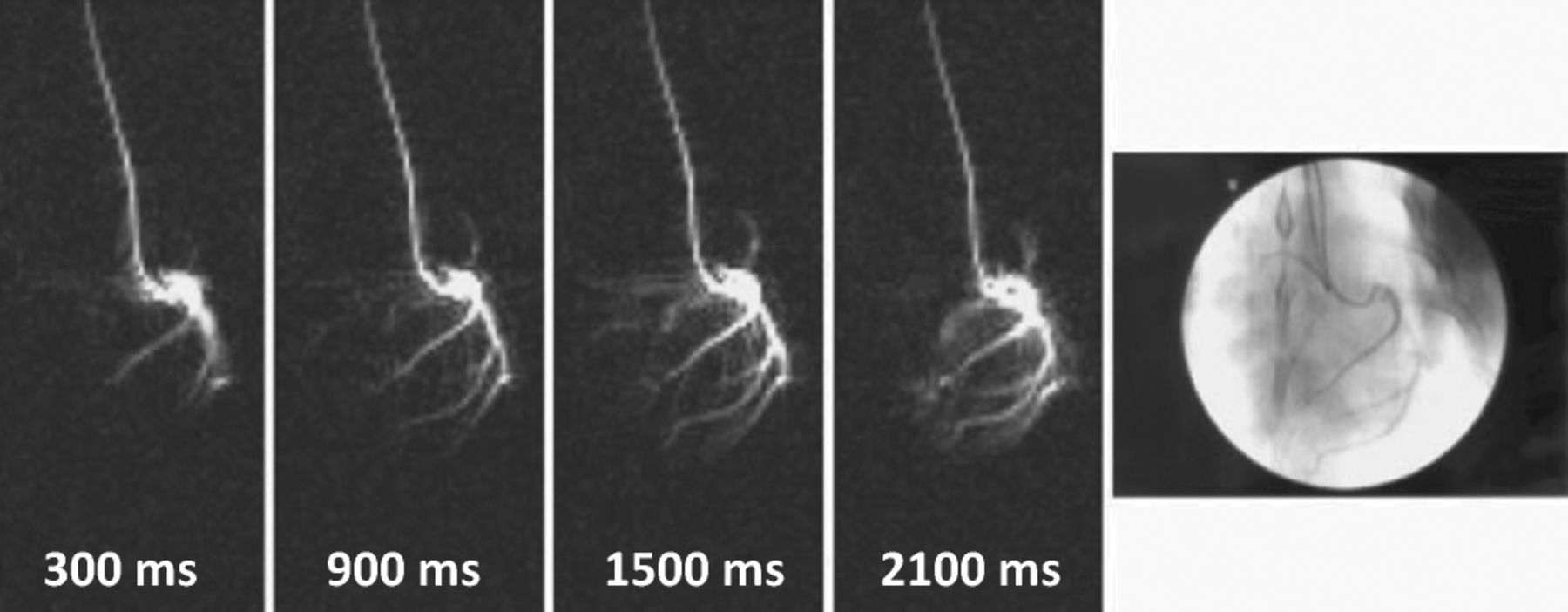
MRI relies on signals generated from hydrogen nuclei that are polarised when placed in a magnetic field; however, only one in 105 nuclei contributes to the detectable signal. Hyperpolarisation is a novel technique whereby the nuclear spin polarisation of an element can be greatly increased, resulting in images derived from alternative nuclei, such as carbon-13 (C13). The high signal produced from this tracer combined with the absence of competing background signal generates high-image contrast36 (Fig 6). Perfusion imaging with C13 is also possible, and imaging with C13-labelled glucose could serve as novel way of assessing myocardial viability.37

The coronary arteries of a pig visualised during arterial catheter injection of hyperpolarized C13. True fast imaging with steady-state free precision (trueFISP) images with 300-ms scan time were acquired continuously during the infusion (0.6 ml/s). The rightmost X-ray image shows the position of the catheter and the coronary arteries after injection of X-ray contrast media. Reproduced with permission from Månsson et al (2006).37
Genotype–phenotype characterisation
Developments in genetic analysis with next-generation sequencing have increased the number of genes linked to the inherited cardiomyopathies.38 To date, there has been little phenotypic characterisation by CMR of patients with individual gene mutations of individual genes; therefore, it is largely unknown whether myocardial fibrosis, structural cardiac abnormalities or other phenotypic features have a genetic causation. In tandem, advances in tissue characterisation capabilities of CMR have lead to the description of new ‘subgroup’ cardiomyopathy phenotypes, prompting the search for their genetic basis. CMR and genetic analysis combine synergistically in the characterisation of the inherited cardiomyopathies and will advance understanding of the role of genetic abnormalities in cardiovascular disease.
Concluding remarks
CMR has proven invaluable both as a research tool and in the clinical assessment of patients across the spectrum of cardiovascular diseases and in research. In vivo tissue characterisation remains its strength and technical advances will ensure continued evolution of these capabilities. CMR has already significantly impacted on survival in thalassaemia major and promises to fulfil a central role in the management of the cardiomyopathies. The potential for microstructural imaging with DTI combined with novel methods of magnetisation ensure that CMR is well placed to remain the most important non-invasive cardiac imaging modality of the future.
- © 2013 Royal College of Physicians
References








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.