
Abstract
Adrenal incidentalomas (AIs) are common and guidelines recommend testing to exclude functioning lesions and malignancy. Their increasing prevalence results in several investigations that are usually conducted in the endocrinology clinic. In 2011, we audited the prevalence and management of AIs identified on computed tomography (CT) imaging of abdomen over 1 calendar month. Consequently, a decision pathway for adrenal lesions was introduced in the radiology department of the Royal Free London Hospital. One year later, we re-audited the local practice. In total, 690 CT scans were reviewed in 2011 compared with 1,264 in 2012. In 2011, 17 (2.46%) patients with AIs were identified, and 26 (2.01%) in 2012. Of those, 1.01% in 2011 and 0.95% in 2012 had newly identified AIs. Only a few patients had been tested to exclude a functional lesion and there was inconsistent terminology in reporting adrenal lesions. Therefore, we support comprehensive reporting of AIs and a selective testing strategy.
Introduction
An adrenal incidentaloma (AI) is defined as a clinically un-suspected adrenal mass, usually >1 cm in diameter, which is discovered on imaging studies conducted for reasons other than investigation of the adrenal glands.1,2 The prevalence of AIs has increased with the use of high-resolution imaging and is cited at 0.4–4.2%.3–6 There are over 44 worldwide reports describing the causes and prevalence of pathologies found in AIs.6 Combining these studies, the aetiology of incidentalomas was as follows: 41% adenomas, 19% metastases, 10% adrenocortical carcinoma, 9% myelolipomas and 8% phaeochromocytoma, with 13% other mostly benign lesions, such as adrenal cysts.6 AIs constitute a common reason for referral in endocrinology clinics and the two main issues to be addressed are whether the lesion is malignant and whether it is functional, both reasons for -adrenalectomy to be considered.7 A series of investigations is normally recommended to exclude cortisol, catecholamine and aldosterone oversecretion, particularly if the patient is -hypertensive.2,7–9
Despite guidance, actual clinical practice appears to differ among centres. In a recent study from Northern Ireland, 51% of patients with an incidentaloma discovered in the radiology department had complete endocrine investigations performed.5 In a similar audit in a different centre, only 2.4–6.1% of patients discovered in the radiology department to have an AI had at least one test to exclude hormone oversecretion from the lesion,10 whereas, in another cohort, 30% of patients with AIs had complete studies for adrenal function.11
Our primary objective in this audit was to discern the prevalence of AIs discovered in modern, high-resolution computed tomography (CT) scans that included the abdomen in an unselected series over a 1-month period. Our secondary objective was to identify the underlying radiological diagnosis and management of the found AIs. Following the initial audit, we devised an investigation and referral pathway to encourage a uniform strategy for reporting and management of incidentally discovered adrenal lesions (Fig 1). One year later, we re-audited our practice and evaluated how well our protocol was being adhered to by the radiology -department.

Decision pathway for newly discovered adrenal adenomas in the radiology department of the Royal Free London Hospital. Myelolipomas are rare benign neoplasms comprising fat and bone marrow in varying proportions; their diagnosis is based on the demonstration of fat within an adrenal mass.15 c/w = consistent with, CT = computerised tomography, HU = Hounsfield unit, pt = patient.
Methods
This audit was conducted in a single tertiary referral centre. Computed tomography (CT) imaging that included the abdomen was reviewed retrospectively for 1 calendar month, March 2011, via our radiology picture archiving and communications system (PACS). Only CT scans examining the abdomen were included, with a maximum slice thickness of 5 mm, encompassing CT scans of abdomen, adrenal glands, virtual colonoscopy, angiography and urography. CT scans of chest were excluded because the adrenal glands were variably imaged in this type of study depending on the phase of respiration and scanning protocol used. In the initial audit, we had a Philips BR 64 and GE Lightspeed CT scanner. In the re-audit, an additional Toshiba Aquilion One CT scanner had been installed in the interim period. The Toshiba is capable of 640, the GE four and the Philips 64 slices per rotation. All CT reports and images were reviewed by three endocrinology trainees (FP, AT and AA) with regard to the appearance of the adrenal glands. The routine radiologists’ reports detailing the abnormal adrenals, including -possible -radiological diagnosis, size of the detected lesions, Hounsfield units (HU), fat content, location of lesion and any relevant previous imaging were recorded. The computerised patient records system (Cerner Millennium), the central laboratory reporting system and patient records were used to ascertain whether these patients had a history of malignancy or were under oncological care, if they were seen in the endocrinology department or if they had any investigations to exclude a functional lesion. The investigation and referral pathway was jointly devised by the endocrinology and radiology departments (Fig 1) following the initial audit. Between April 2011 and the re-audit in March 2012, this pathway was emailed to all reporting radiologists and it featured in the radiology reporting room as a guide for reporting adrenal lesions.
Results
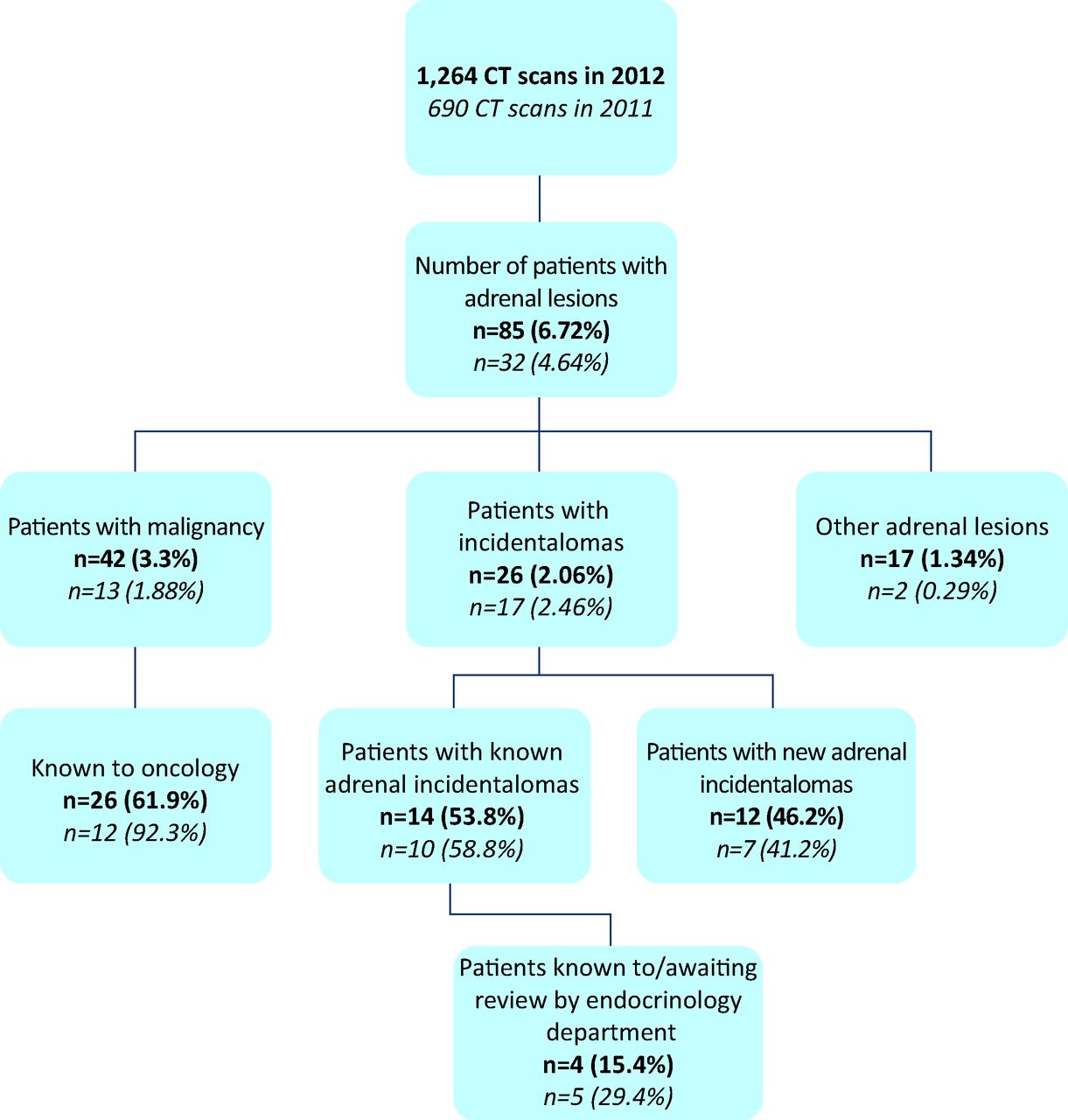
Table 1 and Fig 2 summarise the results for the 2011 and 2012 audits.
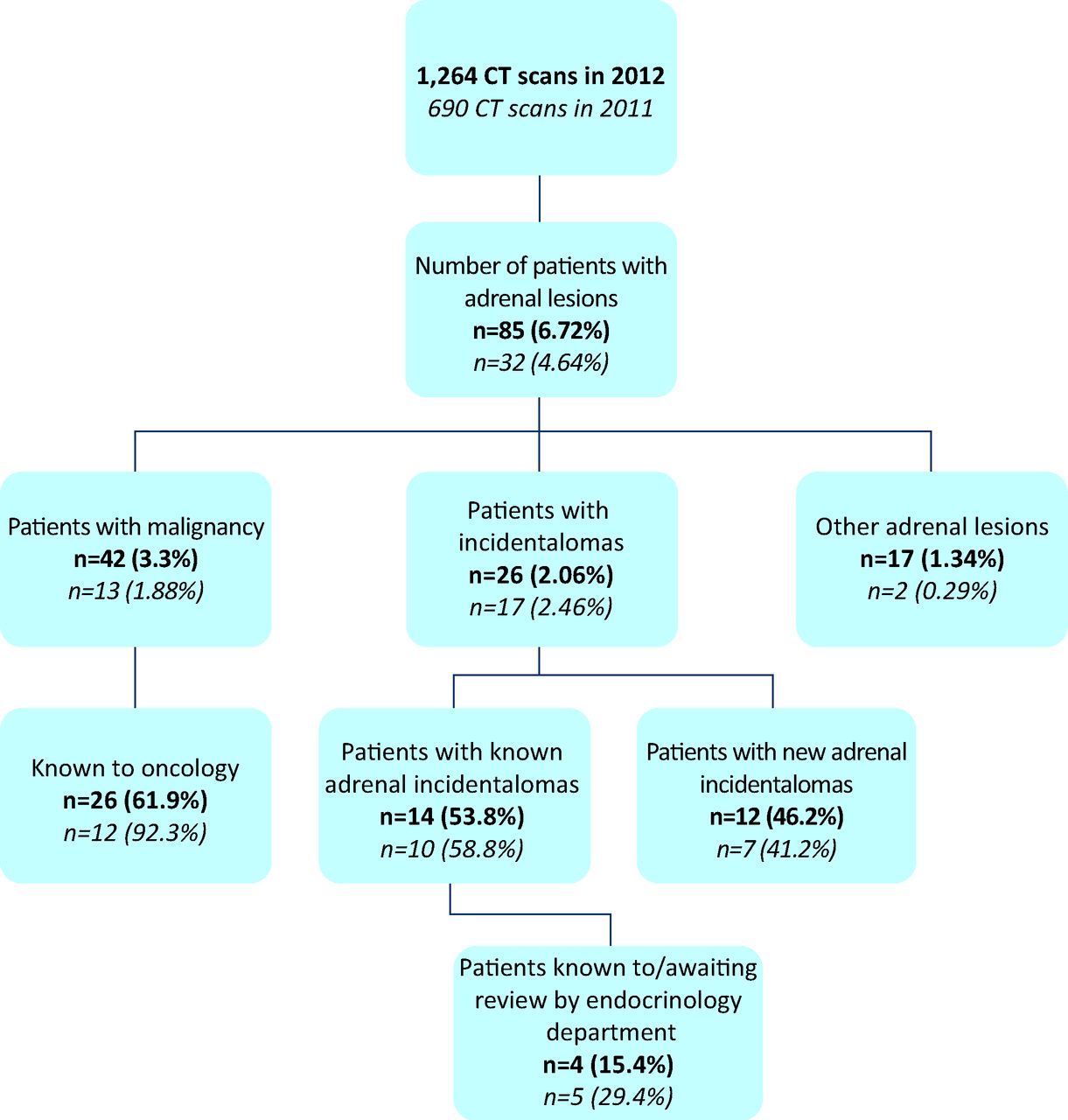
Audit results of 2012 (in black) and 2011 (in red). CT = computerised tomography.
Summary of the characteristics of the two audit cohorts from 2011 and 2012.
March 2011 audit
In March 2011, all 690 CT scans in our centre that included the abdomen were reviewed and 32 patients (4.64%) were identified with adrenal lesions. From these patients, 13/32 (40.6%, 1.88% of all scans) had another malignancy or adrenal metastasis and all but one were -followed up by the oncology department. We excluded patients with malignancy because these patients are at higher risk of adrenal metastasis and therefore do not constitute true ‘incidentalomas’. Excluding patients with malignancy, 19 had adrenal lesions, of which 17 (2.46%) had true AIs, and two (0.29%) had bilateral adrenal hyperplasia or ‘bulky’ adrenals (Fig 3a).
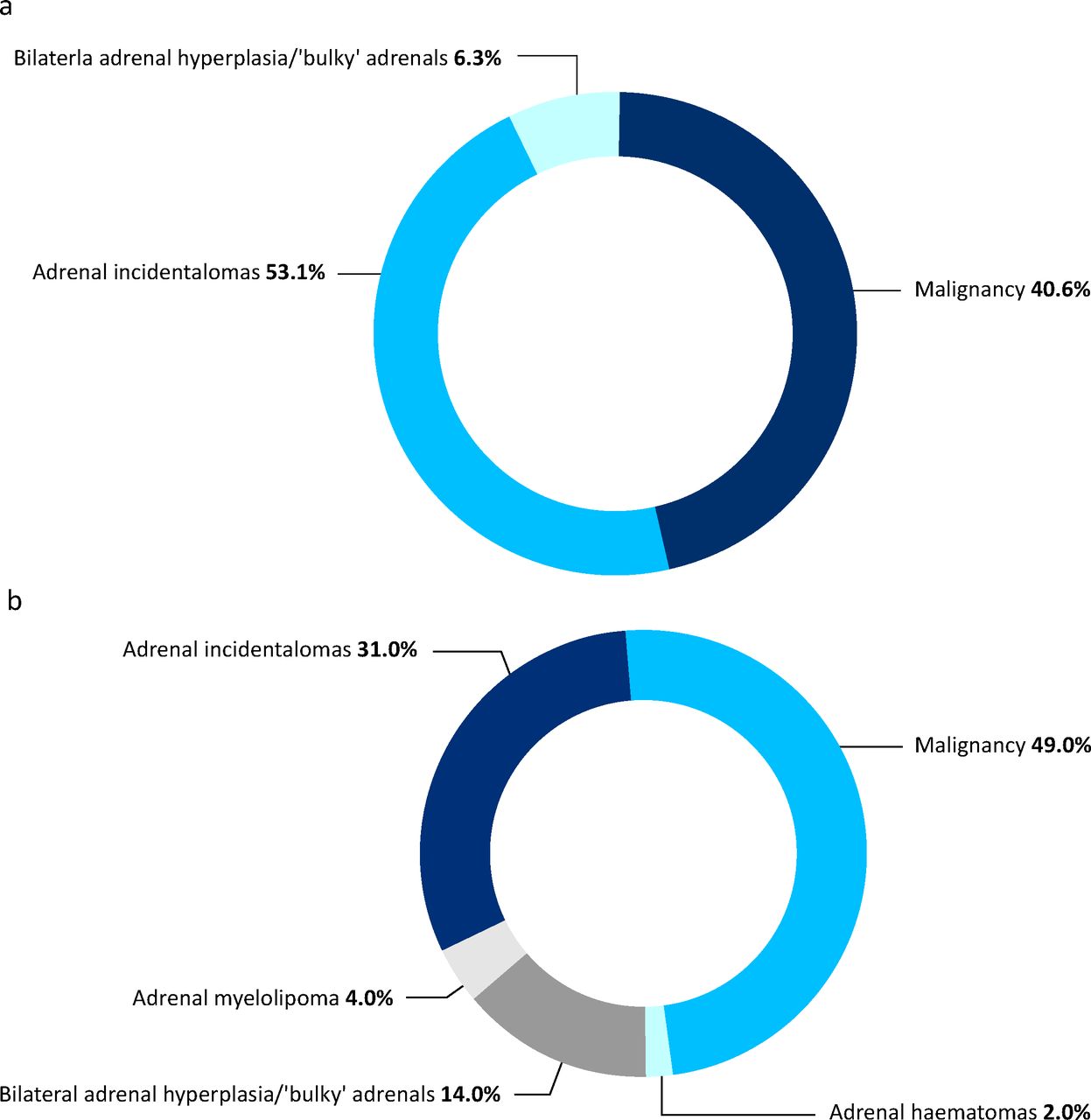
Radiological diagnosis in the two cohorts of patients with adrenal lesions in 2011 (a) and 2012 (b).
The mean size of AI identified in 2011 was 19.43 mm (range 6–40 mm) and 6/17 nodules were bilateral (Fig 4). Mean patient age in this group was 73 years (range 37–89 years) and 8 (47%) were men. Of the 17 patients with AIs, 10 (1.45%) had known and seven (1.01%) had newly identified lesions. Reviewing the reporting of radiological characteristics of the lesions, the electron density in HU was documented in 9/17 AIs and in another 5/17 other terms that implied low electron density, such as ‘fatty adenoma’, were included in the radiologist's report. In 9/10 previously identified lesions, a comparison with previous imaging was made by the reporting radiologist. In all but one case (where the nodule diameter increased by 4 mm, from 9 mm to 13 mm), there was no change in the imaging characteristics of the lesions. In 3/7 of the newly detected adrenal lesions, the reporting radiologist recommended repeat imaging to better characterise the adrenals and in 1/7 cases a referral to the endocrinology department was recommended.
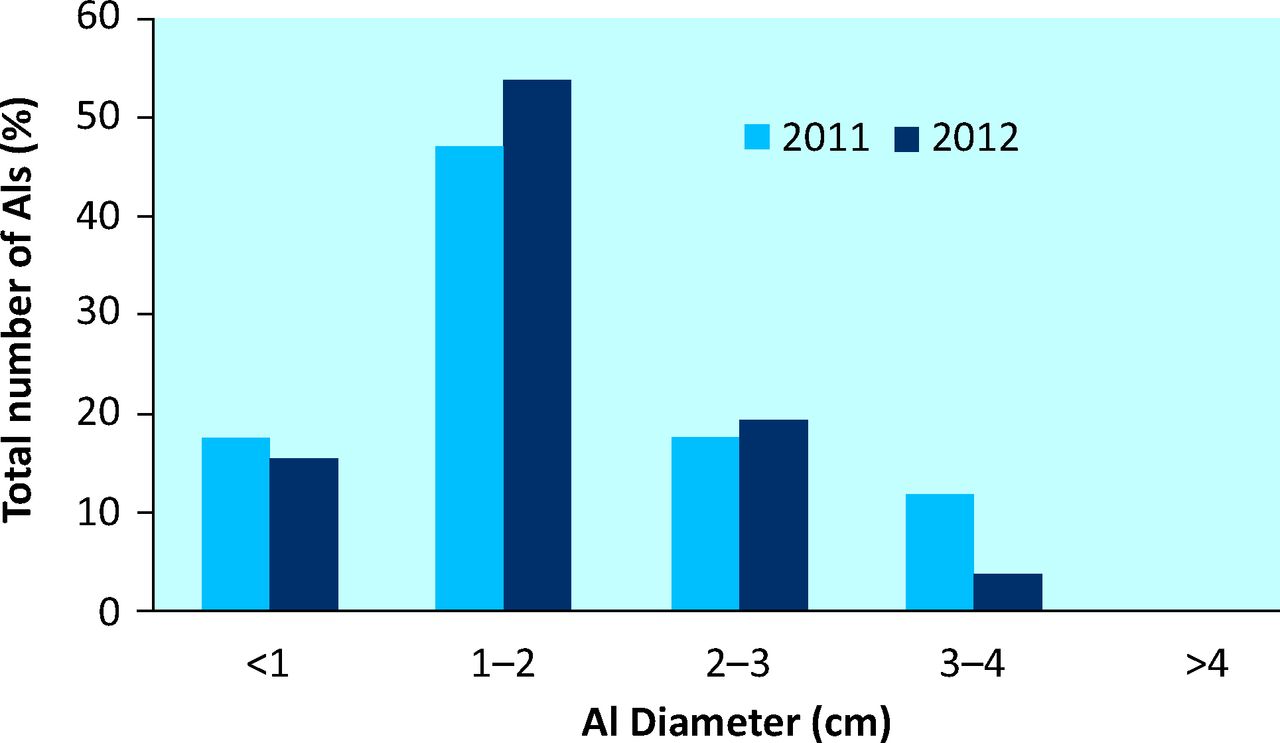
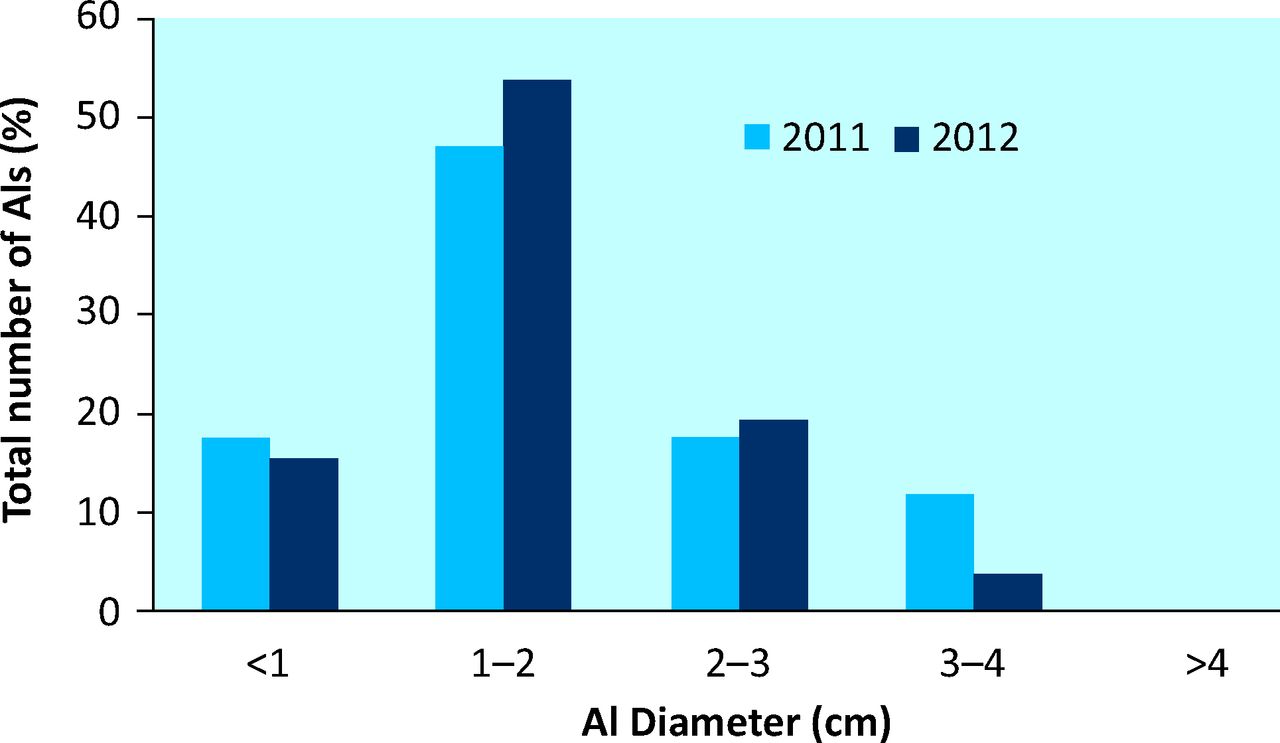
Size distribution of adrenal incidentalomas in the two cohorts from 2011 and 2012. AI = adrenal incentaloma.
From all patients with AIs, 5/17 (29.4%) patients were seen in the endocrinology clinic and all five of these patients had investigations to exclude a -functional lesion. One of the patients seen in the endocrinology clinic was found to have primary hyper-aldosteronism. After excluding the patients seen by the oncology and endocrinology teams, and patients with other radiological diagnosis, 12/17 patients were identified with AIs on imaging criteria. Reviewing all pathology records for these patients, none of them had any investigations to exclude a functional lesion.
March 2012 re-audit
In the re-audit, all 1,264 CT scans carried out in March 2012 were reviewed. Of these, 85 (6.7%) patients were reported to have abnormalities of the adrenal glands. Of these 85 patients, 42 (49.4% or 3.3% in overall re-audit cohort) had a known malignancy. Of the 43 remaining patients, 26 (2.06%) were true AIs, three (0.24%) were adrenal myelolipomas, two (0.16%) were adrenal haematomas and 12 (0.95%) were termed ‘bulky’ or had adrenal hyperplasia (Fig 3b). Two adrenal haematomas were included in this cohort, one in a patient 8 days post liver transplant and one in a patient 2 weeks post left hepatectomy.
Of the 26 AIs, 12 (46.2%, overall 0.95%) were new lesions and 14 (53.8%, overall 1.11%) were seen on previous imaging. Of 13 of the 26 AIs, this information was documented in the report. Mean patient age in this group was 67 years (range 26–98 years) and 14 (54%) were men. The mean size of the AIs was 15.76 mm (range 4–36 mm; Fig 4). In two reports from 2012, there was no documentation of size of the AI.
In total, 24/26 of the AIs were unilateral and in two patients they were bilateral. A measure of attenuation, in the form of HUs, was included in 8/26 reports of AIs. In the other 18 reports, nine included other terminology suggestive of the lesions being adenomas, such as ‘fat containing’, ‘low density’ or ‘lipid rich’. Of the 26 reports, two included relative washout percentages of the AIs. Of the patients, 3/26 (11.5%) were known to the endocrinology department, one was awaiting an endocrine appointment and 22/26 were unknown to our services.
Regarding patients with newly detected AIs, 3/12 were advised by the reporting radiologist to have further imaging for further characterisation, none had a recommended referral to the endocrinology -department and 9/12 had no recommendations included in their report regarding clinical assessment, surveillance or further classification. Of the known AIs, 12/14 were documented as being previously identified, with 11 of these reports including comparison of size from the last imaging. None of these known lesions were documented to have increased in size from the last imaging.
Discussion
In this audit, we initially assessed the prevalence of adrenal lesions discovered in the radiology department, introduced a referral and management pathway, and subsequently re-audited local practice. We have defined ‘incidentalomas’ as discrete adrenal nodules. Therefore, in our analysis, we excluded patients with incidental adrenal hyperplasia or ‘bulky adrenals’ in the absence of nodules.
Both the audit and the re-audit cohorts share some common interesting characteristics. First, a high proportion of the patients with abnormal radiological appearances of the adrenals had a past or current malignancy and were under oncological care (40.6% in 2011 vs 49.4% in 2012). Furthermore, although the number of CT scans in the re-audit was almost double those reviewed in the initial audit, the prevalence of AIs was comparable (2.46% in 2011 vs 2.06% in 2012, or 1.01% vs 0.95% for newly identified lesions only). The increase in the absolute number of scans performed is mainly the result of the -acquisition of a new high-speed CT scanner in the centre during the intervening time. The prevalence of AIs on unselected CT scans of abdomen was greater than some other imaging cohorts,3,5,6 but consistent with others.10 The advanced age of the patients scanned (mean 73 years in the initial audit, 67 years in the re-audit), the use of high-resolution CT scanning and the inclusion of lesions <1 cm, which are excluded in some cohorts, have probably contributed to the higher proportion of patients identified.
In the two audit cohorts, 1% of all patients scanned had a newly discovered adrenal lesion (ie seven patients in March 2011 and 12 patients in March 2012), of which four patients in March 2011 and eight patients in 2012 had lesions >1 cm in diameter. We estimate that the annual number of patients found to have AIs with a diameter >1 cm found yearly in our centre lies between 48 and 96, and this equates to one to two referrals per week to the endocrinology clinic for assessment of adrenal lesions, assuming a 100% referral rate. Investigation is primarily indicated for patients who exhibit hypertension and/or hypokalaemia, because such patients are more likely to have hormonal excess. To address this issue, we introduced the investigation and referral pathway shown in Fig 1. This pathway states that, for lesions sized between 1 cm and 4 cm, the reporting radiologist recommends to the referring physician assessment of their patient for hypertension and hypokalaemic, and a referral to the endocrinology department if required.
The re-audit showed that, in the radiology reports, no recommendations for screening to the requesting clinician, if clinically indicated, were included and, therefore, the pathway we scripted was not adhered to. However, we note that none of the patients identified in the 2011 and 2012 cohorts had an adrenal lesion with a diameter >4 cm, a size for which a more proactive approach would be expected in view of the increased risk of adrenal carcinoma.6 To address the issue of inconsistent reporting, the completed audit cycle was presented in the radiology department audit meeting. The findings of the audit and the reporting protocol were discussed. It was agreed to introduce an ‘adrenal autotext’ to ensure comprehensive reporting and a uniform policy. All of the radiology department, including non-attendees of the meeting, were informed of the agreed conclusions and actions.
Our referral pathway is more conservative in its testing strategy compared with professional guidelines,8,9 the rationale being to select patients with a higher likelihood of secreting or malignant lesions, while minimising the proportion of patients who undergo unnecessary investigations for benign non-secretory adenomas. Evidence suggests that only a few patients will benefit from early detection of incidentalomas, whereas most will suffer the anxiety, adverse effects (eg from ionising radiation exposure) and opportunity costs of further investigation and treatment of an ‘abnormality’ that would not have otherwise led to symptoms or early death.12 By contrast, it is unreasonable to support a strategy where none of the patients with an incidentally discovered lesion would be assessed for hyperfunctionality or malignancy. Indeed, our previous audit, in accordance with other similar cohorts, showed that a proportion of patients with AIs harbour functional lesions, with a reported incidence of phaeochromocytomas of 1–4% and of primary hyperaldosteronism of 1%.2,7 In any case, the value of a selective testing approach can only be shown with long-term prospective follow-up data, which are generally lacking.
The size of AIs is a strong predictor of malignancy risk.6 The mean size of AIs in our cohorts was 19.43 mm in the initial audit and 15.76 mm in the re-audit. This compares with a median diameter of 30 mm in 1,004 incidentally discovered adrenal masses,13 a mean diameter of 26 mm in 37 patients from a single centre5 and a mean of 23 mm in a single centre study with 376 patients.14 We speculate that the use of high-resolution CT, particularly with the new scanner that was installed in between audits, is responsible for the decreases in mean size that we report. It is interesting that the mean lesion diameter in our cohort of 125 patients with AIs referred and reviewed in the endocrine clinic was 19.8 mm.7 This suggests that the population referred for review in clinic does not differ, at least as far as the nodule size is concerned, from unselected patients identified in the radiology department. In our radiology protocol, no investigations are recommended for benign lesions <1 cm. We chose this pragmatic cut-off point because, in our experience, small lesions on initial unenhanced CTs do not often represent true lesions on dedicated adrenal scanning. Indeed, two nodules in the 2011 audit cohort measuring 6 mm and 8 mm could not be seen on subsequent scanning and another was almost invisible. Although some functional nodules can present as small lesions, this number is small overall, and would result in detailed investigations, for little additional gain.
CT features are valuable for assessing AIs. Attenuation thresholds have shown a better performance to diagnose adrenal malignancy and non-adenomas compared with size or subjective criteria.6 An attenuation of less than 10 HUs on an unenhanced scan is suggestive of an adrenal adenoma because intracytoplasmic adipose is often abundant in adenomas. A >50% washout 10 min post contrast administration was 100% sensitive and specific for an adenoma in a comparison between patients with adenomas and those with carcinomas, phaeo-chromocytomas or metastatic disease.2 Not all radiology reports of the AIs in this audit included HU and, in the absence of a specific HU measurement, a description suggestive of a lipid-rich benign lesion was only detailed in a few cases.
A few patients with AIs were seen in the endocrinology clinic (29.4% in 2011 vs 15.4% in 2012). It seems that none of the patients outside the endocrinology clinic had investigations to exclude a functional lesion, although we cannot exclude the possibility that patients might have had testing at a different centre following the discovery of the adrenal nodule. This is similar to the experience reported from cohorts of other centres.5,10,11
Conclusions
Adrenal incidentalomas are common and, in our centre, 1% of all patients scanned monthly had a newly described adrenal lesion. The imaging phenotype cannot predict hormonal function, but it does predict the underlying pathology. Therefore, it is paramount that radiology reporting of AIs is comprehensive and standardised. Selective referral and assessment of patients with AIs and co-existent hypertension and/or hypokalaemia is warranted. Education of radiologists and medical practitioners regarding this matter will ensure informed reporting and structured -management.
Key points
1% of all patients scanned monthly in our centre had a newly discovered adrenal lesion
AI size, HUs and comparison with previous imaging can help decision making
Lesions with a non-contrast CT HU of >10 should be scanned with dedicated adrenal CT scanning or magnetic resonance imaging to exclude malignancy
Testing to exclude a functioning AI is recommended for patients with hypertension, hypokalaemia or features of Cushing's syndrome
A structured approach in AI reporting and management can identify individuals with a high likelihood of important underlying pathology
A radiology ‘adrenal autotext’ for radiology AI reporting might prove useful
AI = adrenal incidentaloma; CT = computed tomography; HU = Hounsfield unit.
- © 2014 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}
{kind=link}