
Abstract
Purulent pericarditis is now rare due to the widespread use of antibiotics. However, it is associated with significant morbidity and mortality, and non-specific symptoms and signs can make diagnosis difficult. We report a patient who presented with left-sided chest pain, mild fever and ST segment elevation on electrocardiography, who required prolonged organ support in the intensive care unit. This lesson highlights the diagnostic difficulties and management challenges that this condition can present.
Case history
A 50-year-old gentleman presented to the emergency department with a 2-day history of intermittent chest pain radiating under his left arm, which was associated with shortness of breath. He had no symptoms of nausea, vomiting, palpitations, cough or fever, and his past medical history was unremarkable.
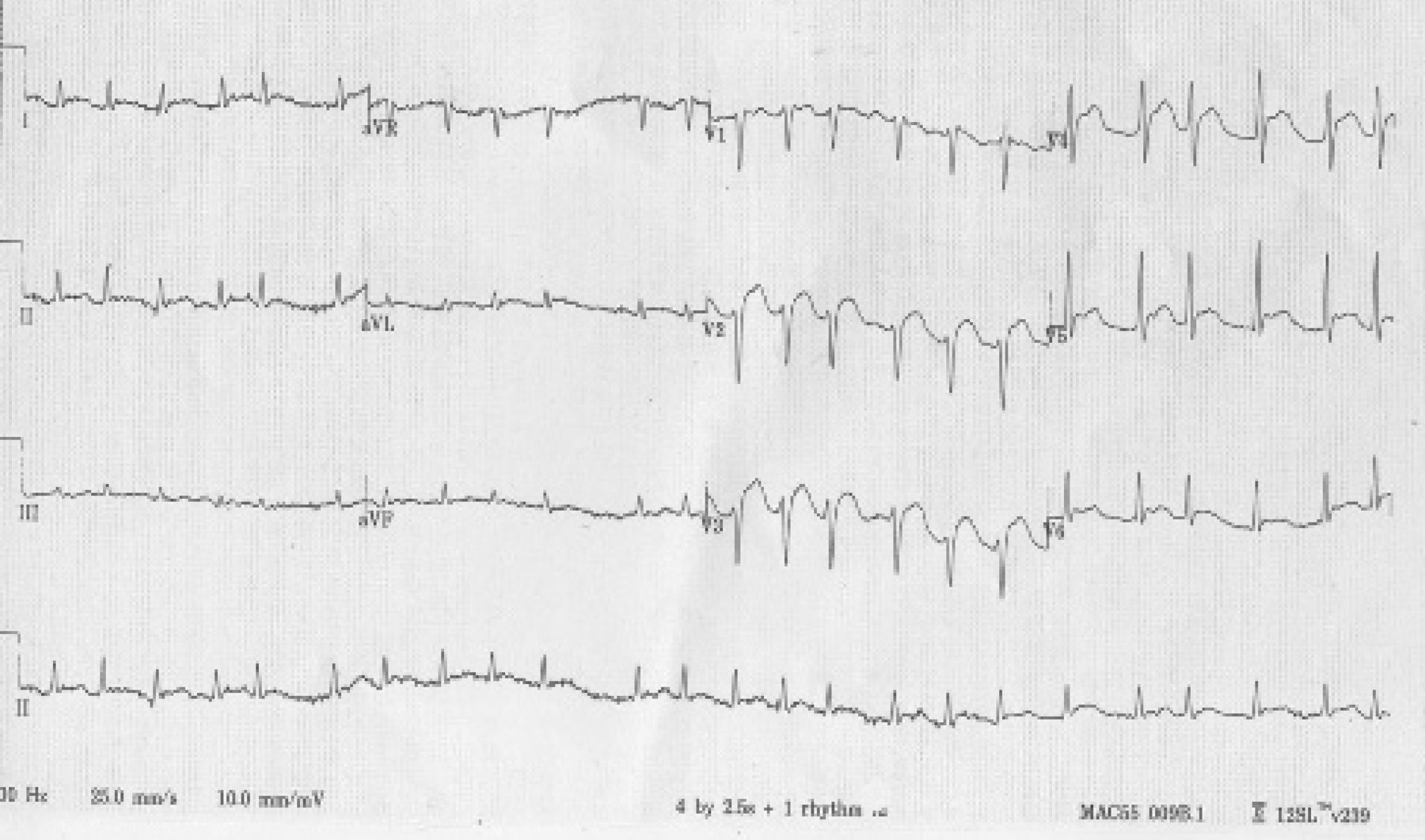
On initial assessment, he had a temperature of 37.5°C, blood pressure of 146/82 mmHg, and tachycardia of 100 beats per minute. His respiratory rate was 36 breaths per minute, and his oxygen saturation was 95% in room air. Examination revealed reduced bibasal breath sounds but was otherwise normal. The initial electrocardiogram (ECG) demonstrated ST elevation in leads V2–6 (Fig 1), prompting urgent transfer to the cardiac catheterisation laboratory for a coronary angiogram; however, this showed only minimal right coronary artery disease.
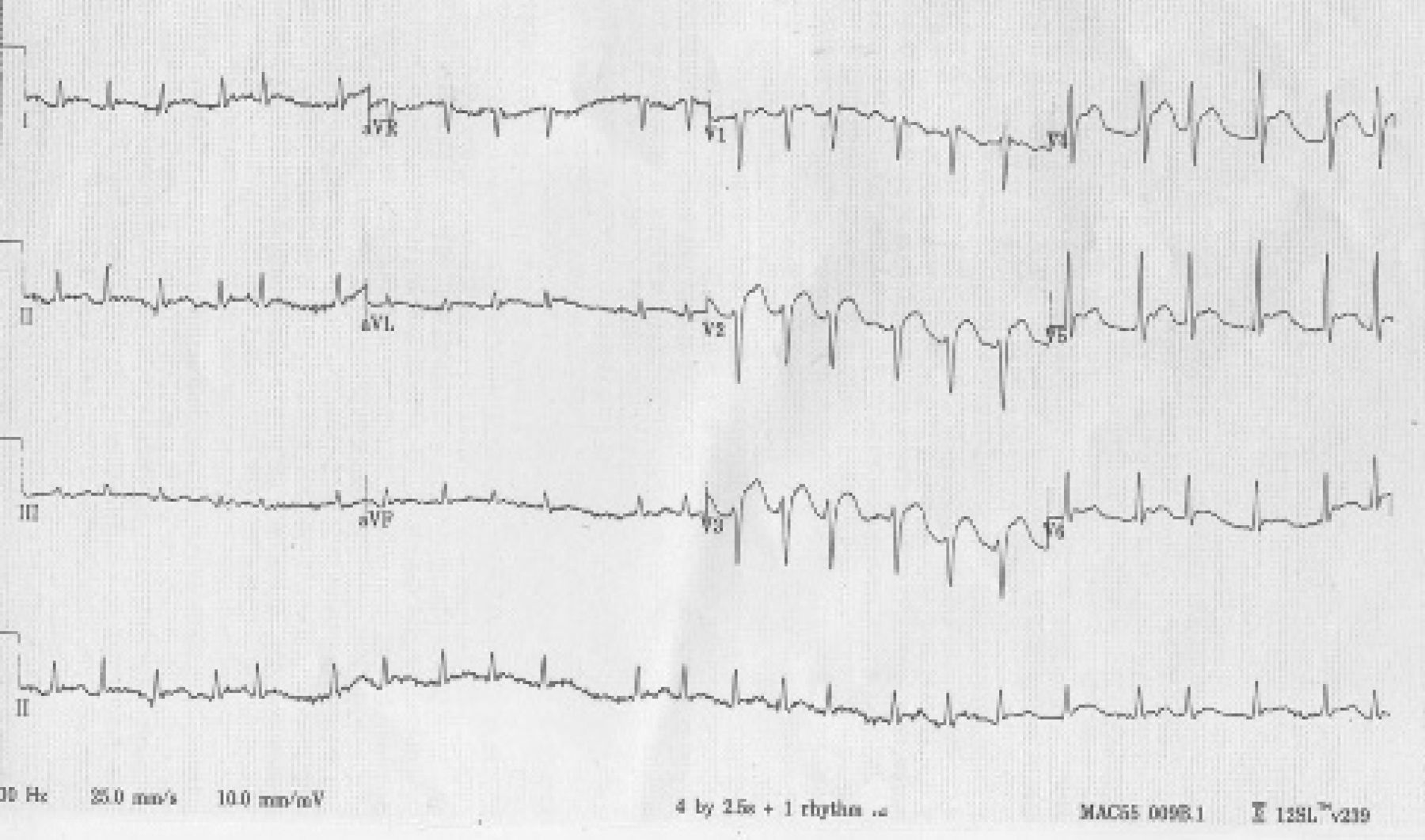
ECG showing ST elevation in leads V2–6. ECG = electrocardiogram.
On return from the catheterisation suite, a bedside echocardiogram was performed, revealing a small pericardial effusion (1.5 cm). There was no evidence of cardiac tamponade and biventricular function was good. Blood results showed raised inflammatory markers (C-reactive protein 324 mg/l, white cell count 24.3 × 109/l), hyponatraemia (116 mmol/l), and deranged clotting (international normalised ratio 1.4 and platelets 131 × 109/l). Computed tomography (CT) of the thorax confirmed the pericardial effusion, and bilateral pleural effusions and right basal consolidation were also noted (Fig 2).
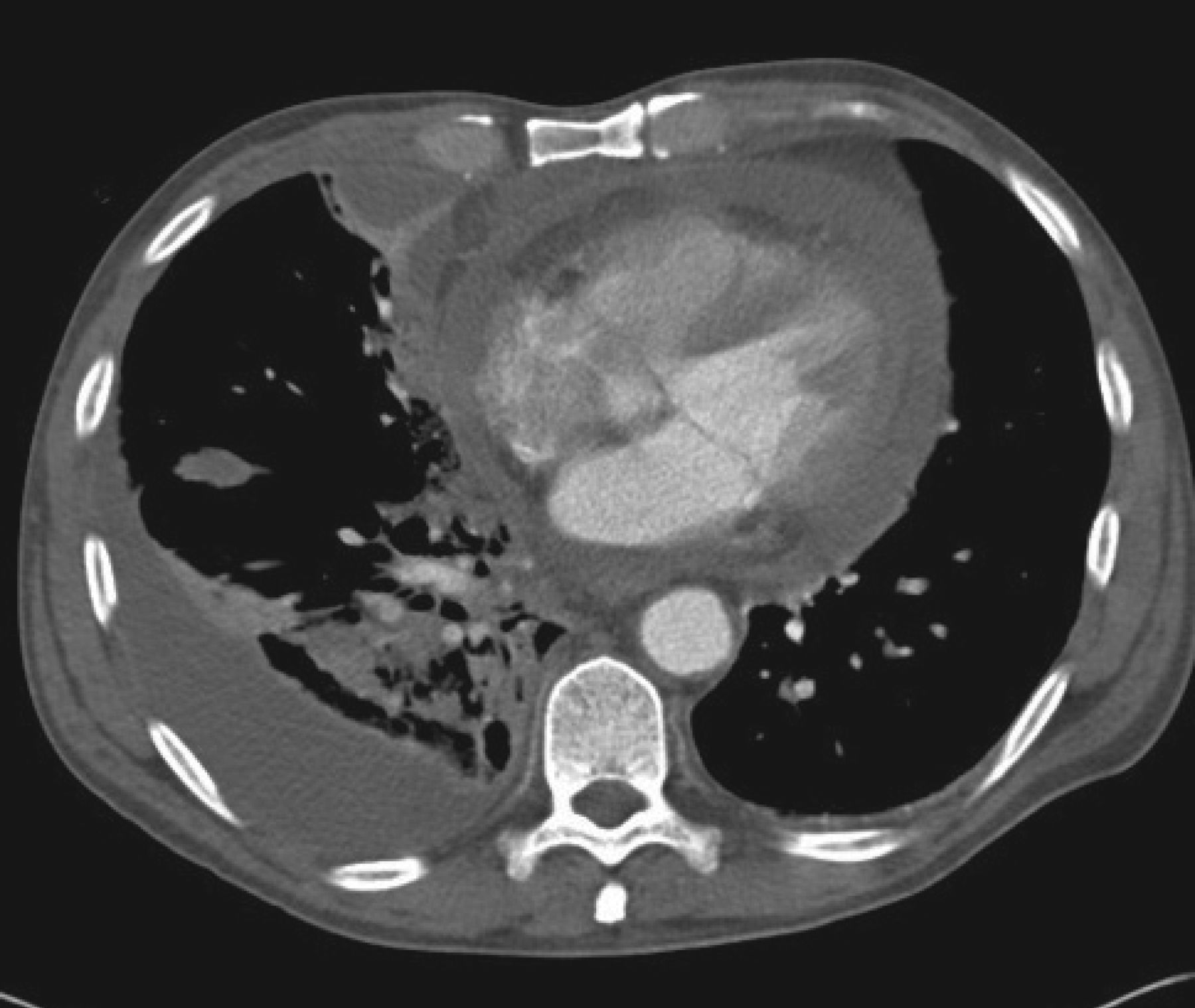
CT thorax demonstrating pericardial and pleural effusions, and right basal consolidation. CT = computed tomography.
The patient was started on broad-spectrum intravenous antibiotics, and Streptococcus pneumoniae was subsequently isolated from blood cultures. Serology testing for human immunodeficiency virus (HIV) was negative. Unfortunately, the patient developed acute kidney injury (urea 22.5 mmol/l and creatinine 273 μmol/l) within 48 hours of admission and became hypoxic and hypotensive, precipitating admission to the intensive care unit (ICU) for inotropic, ventilatory and renal support.
Due to ongoing haemodynamic instability in the ICU, pericardiocentesis was performed and 600 ml of frank pus was drained. Over subsequent days, frank pus continued to drain from the pericardium and inflammatory markers remained high. Repeat CT of the thorax showed that the pleural and pericardial effusions were increasing in size. Bilateral chest drains were inserted, and thoracotomy was performed to create a pericardial window. Despite this, the patient remained tachycardic and dependent on vasopressors. A repeat echocardiogram suggested constrictive pericarditis, which was confirmed by right and left heart catheterisation. Although pericardectomy was considered, the patient was felt to be too unwell to undergo surgery. He underwent aggressive diuresis and was slowly weaned from mechanical ventilation. He was eventually discharged from the ICU after 47 days and from hospital 6 days later. On subsequent review in clinic, the patient was progressing well on medical management, and a repeat echocardiogram 4 months after discharge showed no evidence of constriction and normal right ventricular systolic pressure.
Discussion
Purulent pericarditis or pyopericardium is diagnosed when pus is present in the pericardial space or when culture of pericardial aspirate yields bacteria. It is rare since the introduction of antibiotics1 and is often diagnosed late.2 It is most often caused by haematogenous or contiguous spread of infection from elsewhere in the body.3 Risk factors include chest trauma, thoracic surgery and immunosuppression. Common causative organisms include Staphylococcus aureus, Streptococcus pneumoniae, Haemophilus influenzae and Streptococcus viridans.
Purulent pericarditis most often presents with signs and symptoms of sepsis and acute cardiovascular collapse. Classic signs such as pericardial rub, high central venous pressure, pulsus paradoxus and enlarged cardiac silhouette on chest radiography are frequently absent,1,3–7 which can make diagnosis challenging. The most consistent signs are non specific, such as tachycardia and pyrexia, and the diagnosis of pyopericardium may not be considered when a source of infection is identified elsewhere.8
Changes on ECG are also frequently non-specific and may cloud the diagnostic picture by indicating alternative diagnoses. In the case reported here, the findings on ECG raised suspicion of myocardial infarction, prompting urgent angiography. Similarly, other cases in the literature report non-specific ECG findings or changes suggestive of acute myocardial infarction.1,9 A review by Hall found that only 23% of cases of purulent pericarditis demonstrated ‘classic’ ST segment elevation.7 For these reasons and despite the advances of modern medicine, diagnosis of purulent pericarditis remains challenging and a high index of suspicion is therefore required to ensure timely diagnosis and treatment.
Management of pyopericardium involves prompt antibiotic treatment in combination with drainage of the pus from the pericardium.5,9,10 Prolonged antibiotic courses are used, with most published reports documenting successful treatment with 2–4 weeks of antibiotics.11 Open pericardial drainage may be preferable to pericardiocentesis,12 but repeated pericardial aspiration in combination with antibiotics has been reported to be effective in isolated cases.13,14 Prognosis is largely dependent on the timeliness of diagnosis and treatment,10 with early recognition and treatment reducing the mortality from almost 100% to less than 20%.4,9,15
Conclusion
Pyopericarditis is rare now but presents a diagnostic challenge as the classic symptoms and signs are often absent. Changes on ECG are unreliable for predicting pericarditis and the presence of a pericardial effusion, and may even suggest alternative diagnoses such as myocardial infarction. In febrile patients with ST elevation on ECG and a normal coronary angiogram, purulent pericarditis should be considered, particularly when they have coexistent infection or predisposing factors. Optimal management requires a combination of prolonged antibiotic therapy, pericardial drainage and, in some cases, pericardectomy. Early diagnosis and treatment significantly improves outcome.
- © 2014 Royal College of Physicians
References








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.