
Abstract
This concise guideline summarises the key recommendations from the recent National Institute for Health and Care Excellence (NICE) clinical guideline on the assessment and management of psoriasis (CG153) that are relevant to the non-dermatologist. The aim is to highlight important considerations for assessment and referral of people with psoriasis, including identification of relevant comorbid conditions. Psoriasis is a common inflammatory skin condition and, especially when severe, can be associated with increased risk of cardiovascular disease, diabetes and depression. Functional, psychological and social morbidity can also be encountered, and the extent of the disability is frequently underestimated. Importantly, highly effective treatments are available. Appropriate assessment and referral of people with psoriasis therefore has the potential to improve outcomes by correctly identifying the appropriate treatment pathway. Assessment should involve not only disease severity but also the impact on patient well-being and whether the patient has any comorbid conditions, such as psoriatic arthritis, which requires rapid referral to a rheumatologist.
Introduction
Psoriasis is an inflammatory skin disease that typically follows a relapsing and remitting course. The prevalence of psoriasis is estimated to be about 1.3–2.2% in the UK1 and it is associated with joint disease – psoriatic arthritis – in a significant proportion of patients (13.8% in one study).2
The different phenotypes of psoriasis include:
plaque psoriasis (about 90% of cases): well-delineated red, scaly plaques
guttate psoriasis: an acute eruption of small papules, which is often preceded by streptococcal infection
pustular psoriasis: localised or generalised.
Distinctive nail changes occur in about 50% of all those affected and are more common in people with associated joint disease. People with psoriasis, particularly those with severe disease, are also at increased risk of a number of comorbidities, including depression, alcohol-related problems, cardiovascular disease, metabolic syndrome and non-melanoma skin cancer.3–7
Many people with psoriasis experience profound functional, psychological and social morbidity, with consequently reduced levels of employment and income. Factors that contribute to this include:
symptoms related to the skin (for example, chronic itching, bleeding, scaling and nail involvement)
problems related to treatments, many of which can be messy and time consuming
psoriatic arthritis
the impact of living with a highly visible and stigmatising skin disease.
Doctors, including dermatologists, often fail to appreciate the extent of disability, and many people with psoriasis are dissatisfied with their treatment, although highly effective and cost-effective treatments are available.8 The National Institute for Health and Care Excellence (NICE) clinical guideline on psoriasis, which was published in 2012,9 provides comprehensive recommendations on the assessment and management of all types of psoriasis, with information on the spectrum of available active interventions – from simple creams and ointments through to phototherapy and standard systemic and biologic treatments.
Although most people with psoriasis are managed in primary care, healthcare professionals working in acute and/or non-dermatological specialist settings are also highly likely to come into contact with affected patients. Psoriasis is common and will be a coincidental finding in many patients; specialist input may be requested in relation to comorbid conditions or complications from treatments for psoriasis – for example, patients may develop tumour necrosis factor (TNF) antagonist-related reactivation of tuberculosis or methotrexate-related hepatotoxicity and patients with very severe and unstable disease may become systemically unwell and require inpatient or intensive care management. Improved awareness of the condition among non-specialist clinicians thus will benefit people with psoriasis.
Scope and purpose
This concise guideline summarises some of the key recommendations detailed in the full NICE guideline.9 It is intended for use by all healthcare professionals who encounter patients with psoriasis and focuses on assessment and referral as relevant to the non-dermatologist, including identification of relevant comorbid conditions. A summary of the overall care pathway is also included to provide some context. Please refer to the full NICE guideline9 for recommendations on the use of specific treatment options.
The recommendations
Holistic assessment of patients with psoriasis presenting to any healthcare professional should encompass the psoriasis itself and the impact the disease has on the individual's well-being. Both dimensions are important to ensure that patients are directed towards appropriate services and treatments to meet their individual requirements and minimise morbidity. Currently, there are no biomarkers for disease activity in psoriasis, so ‘measurement’ is based on clinical evaluation of the skin. In addition, the impact of psoriasis on an affected person's well-being can be underestimated by clinicians managing skin disease, even in specialist settings, which makes formal assessment important. Early assessment for psoriatic arthritis is also important to ensure timely access to rheumatology services and to minimise associated progressive joint damage and loss of function.10 Similarly, identification of those at risk of cardiovascular disease is key to early management of modifiable risk factors.
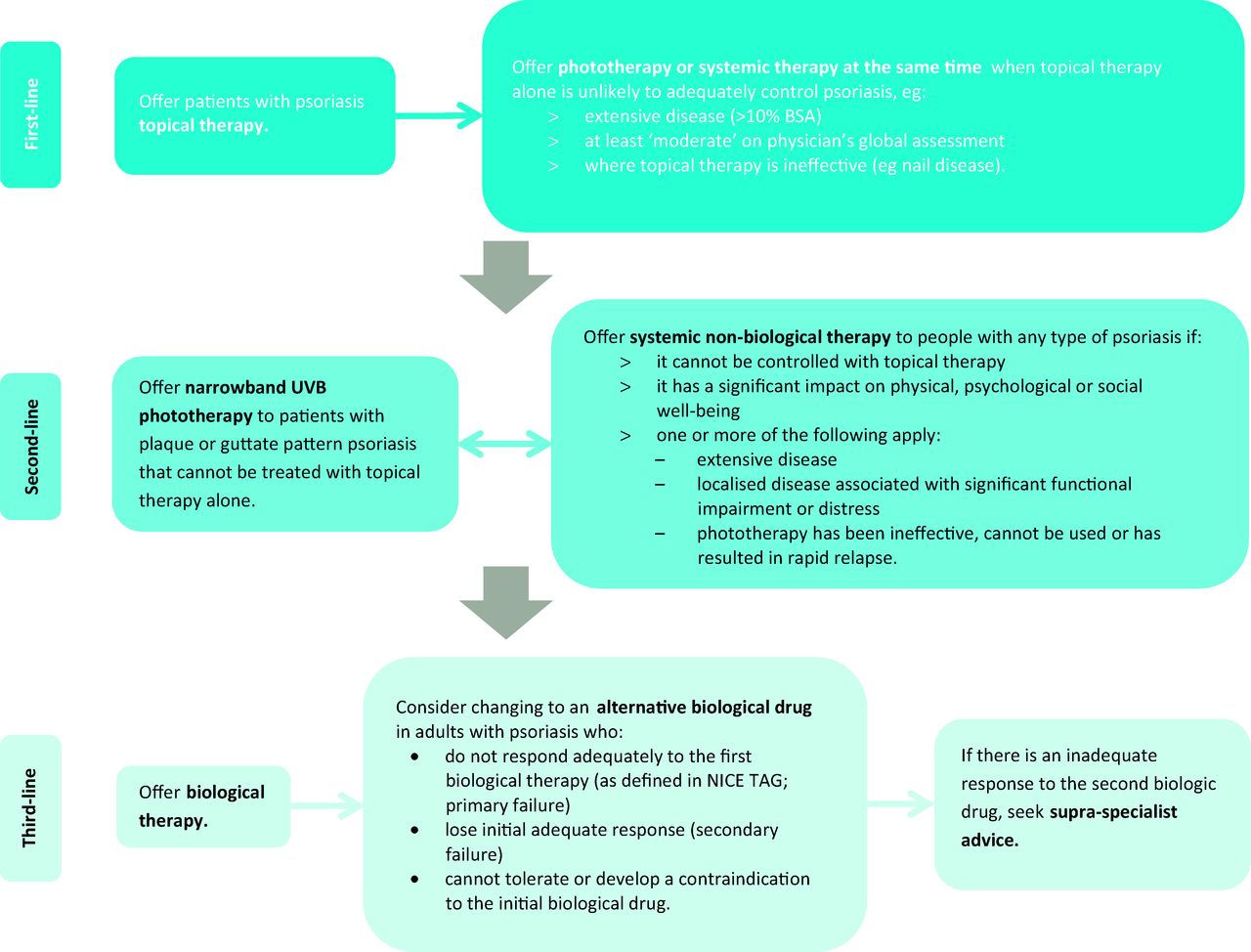
Formal assessment will determine the optimal treatment approach. To date, no treatment has been shown to alter the overall prognosis, so choice of intervention is strongly influenced by how much the psoriasis is bothering the patient, the extent and site of disease, and the presence of arthritis. Topical therapy (first line) is the mainstay of treatment for mild-to-moderate psoriasis. Second-line therapy includes phototherapy with broad- or narrow-band ultraviolet (UV) B light or psoralen plus UVA light (PUVA) and systemic non-biologic agents such as ciclosporin, methotrexate and acitretin. Third-line therapy comprises biologic therapies such as the TNF antagonists (eg adalimumab, etanercept and infliximab) and ustekinumab, which have revolutionised the treatment of severe disease, with a consequent 90% reduction in demand for inpatient management (Fig 1).

Treatment approaches to psoriasis recommended in NICE's CG 153. BSA = body surface area; CG = clinical guideline; NICE = National Institute for Health and Care Excellence; TAG = technology appraisal guidance; UVB = ultraviolet B.
Based on these principles and the available evidence, CG153 made 109 recommendations. Table 1 highlights those of particular relevance to non-specialist clinicians, especially those that, when implemented, might generate referrals outside of the dermatology setting.
Key recommendations of NICE's CG 153 relevant to non-specialist clinicians.9
Limitations of the guideline
Although the recommendations in the NICE guideline9 are based on the best available evidence, consensus recommendations were required in a number of key areas due to a lack of available evidence, particularly surrounding assessment tools in primary care and all aspects of paediatric care for psoriasis.
Recommendations can be based only on the best assessment methods currently available, although these are not without fault. For example, estimating body surface area (BSA) involvement can be difficult, especially with small plaque or guttate psoriasis, and there were gaps in the evidence. However, the benefits of considering the extent of disease and the clinical utility of this tool for all types of psoriasis in all settings outweigh this limitation.
When considering the optimum approach to assessment and referral for psoriatic arthritis, the guideline development group weighed up the healthcare setting, the time taken to complete assessments and the degree of expertise required to use and interpret the scores. The psoriasis epidemiology screening tool (PEST) questionnaire11 was considered to offer the best overall balance, being simple and easy to administer and having good sensitivity. However, uncertainty remains about the most appropriate tool due to the paucity of data.
In all of these areas, therefore, further research is required, and the guideline may need to be updated accordingly. The guideline therefore elaborates on best practice based on the current evidence. Clinicians need to judge on a case-by-case basis the most appropriate timing and method to assess comorbidities in order to offer preventive advice while avoiding unnecessary anxiety in people with psoriasis.
Implications and implementation
The main barrier to successful implementation of this guidance is likely to be insufficient training or understanding about psoriasis among healthcare professionals, as dermatology training is not compulsory. Formal assessment of psoriasis may represent a substantial shift in approach, and the recently published quality standards24 and implementation tools that will be developed will support its application in practice.
- © 2014 Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.