
Case presentation
A 62-year-old man was admitted via the emergency department having been found unresponsive with clenched teeth and open eyes. His family reported deterioration in speech over the previous 7 days that had worsened in the preceding 48 hours. They also reported complaints of dizziness and vertigo. The only past medical history of note was depression and anxiety that had been treated with gabapentin and mirtazapine. At presentation he was hypothermic with a temperature of 34.2°C, maintaining his airway, breathing spontaneously, cardiovascularly stable and with no identifiable biochemical or metabolic cause for a Glasgow coma scale (GCS) of 6. Neurological examination revealed normal tone and intact reflexes; however, power and sensation could not be assessed due to low GCS. The pupils were bilaterally equal and reactive to light.
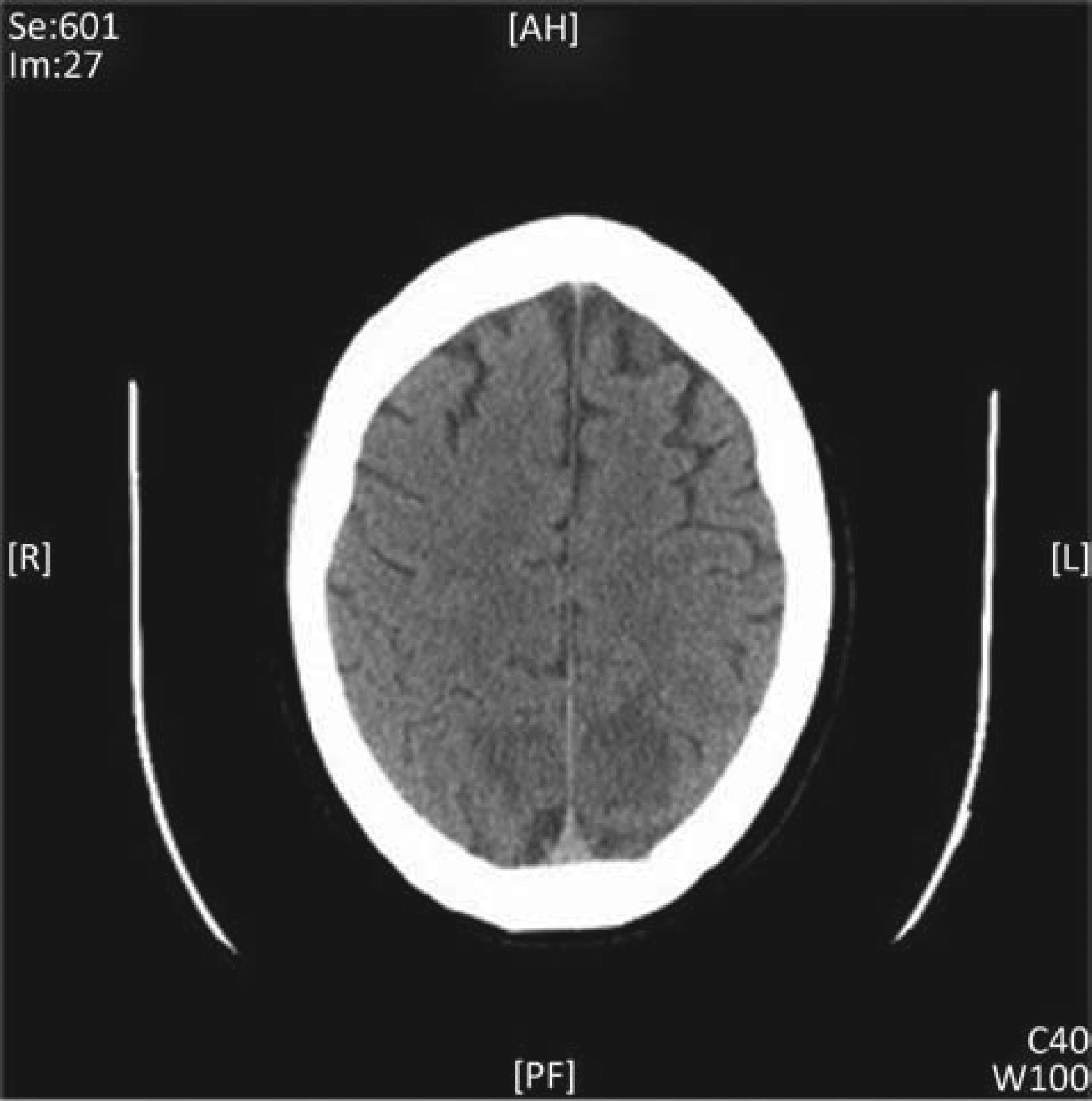
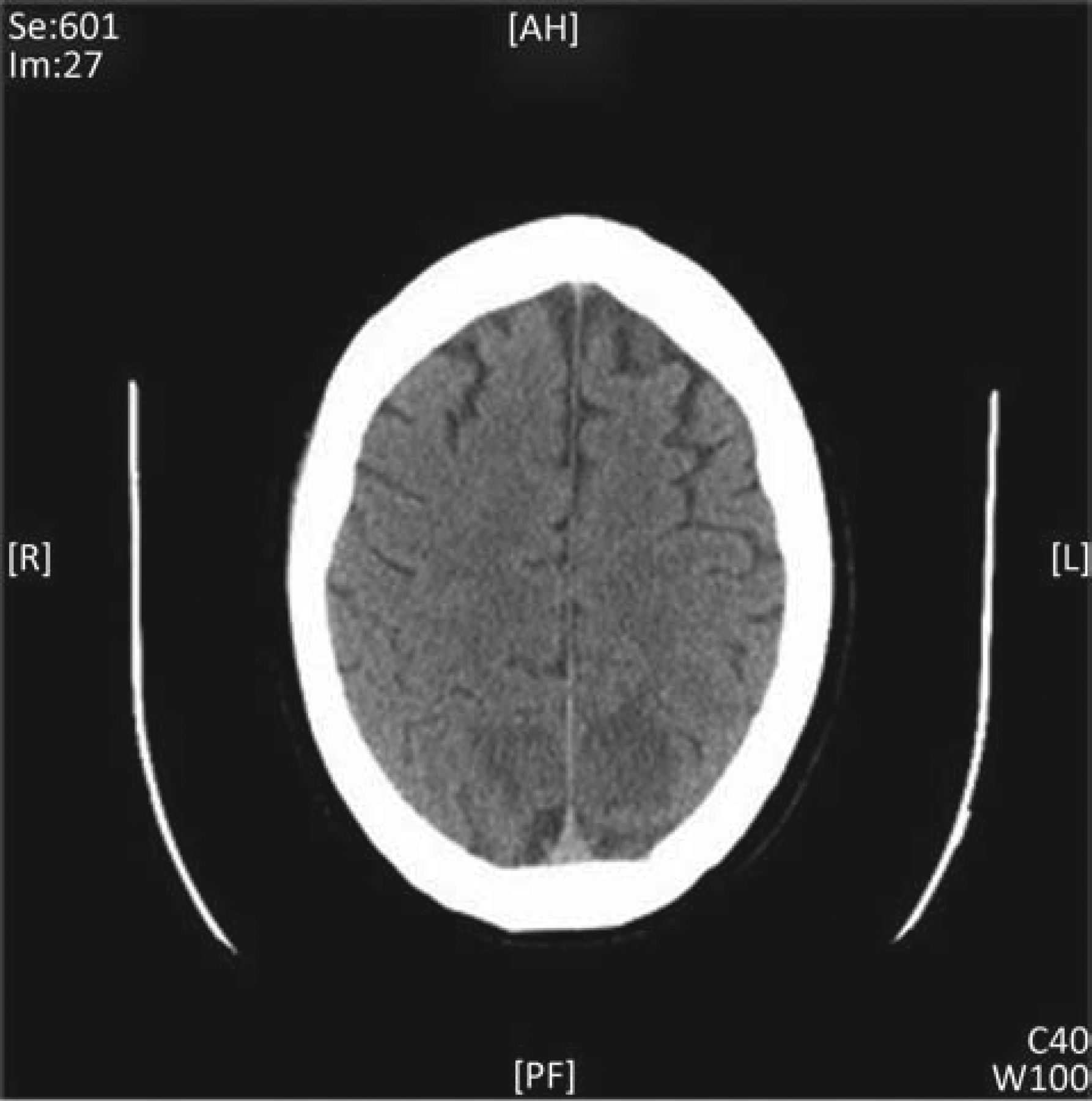
Initial bloods were unremarkable. Non-contrast head computed tomography (CT) scan revealed bilateral occipital infarcts (Fig 1). Magnetic resonance imaging (MRI) was recommended by the radiologist to ascertain the diagnosis. Unfortunately the patient deteriorated into status epilepticus which could not be controlled by lorazepam. His airway was secured by rapid sequence intubation and he was invasively ventilated, sedated with propofol and paralysed with atracurium. A contrast CT angiogram was performed; this demonstrated bilateral ill-defined, non-enhancing areas of low attenuation within the posterior regions of parietal lobes in addition to similar bilateral lesions in the occipital lobes.
CT scan shows bilateral occipital lesions in keeping with infracts. CT = computed tomography.
Differential diagnosis included:
cerebrovascular accident (CVA)
infective encephalitis
autoimmune encephalitis
vasculitis.
Treatment
The patient persisted in status epilepticus with no improvement in GCS in the inter-ictal period. Given the absence of a definitive diagnosis and the suspicion of autoimmune or infective cause for his deterioration, intensive care was provided with a view to establish the diagnosis in the interim by further investigation. Sedation, paralysis and ventilation were continued in addition to the institution of the following neuroprotective strategies;
head up tilt of 15–30 degrees
put in neutral position with no restriction to head and neck venous drainage
MAP of 80–90
haemoglobin of 80–110 gm/l
partial pressure of oxygen (PaO2) of >13 kPa
partial pressure of carbon dioxide (PaCO2) of 4.5–5 kPa
controlling of pyrexia and seizures.
He received a loading and maintenance infusion of phenytoin and sodium valproate to treat status epilepticus. Cerebral oedema, either due to infective or autoimmune origin, as well as status-related persistent hypertension, could not be ruled out. Therefore an infusion of 1 g/kg of mannitol along with dexamethosone was also administered.
Following a discussion with the neurologist and microbiologist (due to the suspicion of meningitis and encephalitis), antimicrobial therapy with aciclovir and cefotaxime were initiated. To establish the diagnosis a lumbar puncture was performed, vasculitis, endocarditis and autoimmune encephalitis screens were undertaken, and antibody screens for voltage-gated potassium channel, N-methyl-D-aspartate (NMDA) receptor, antiGAD and paraneoplastic antibodies were undertaken. Following the optimisation of antiepileptic medication, sedation was turned off with a very slow recovery of GCS to 13/15. Motor power was 2/5 on day 6 to achieve extubation. All results of the investigations were unremarkable.
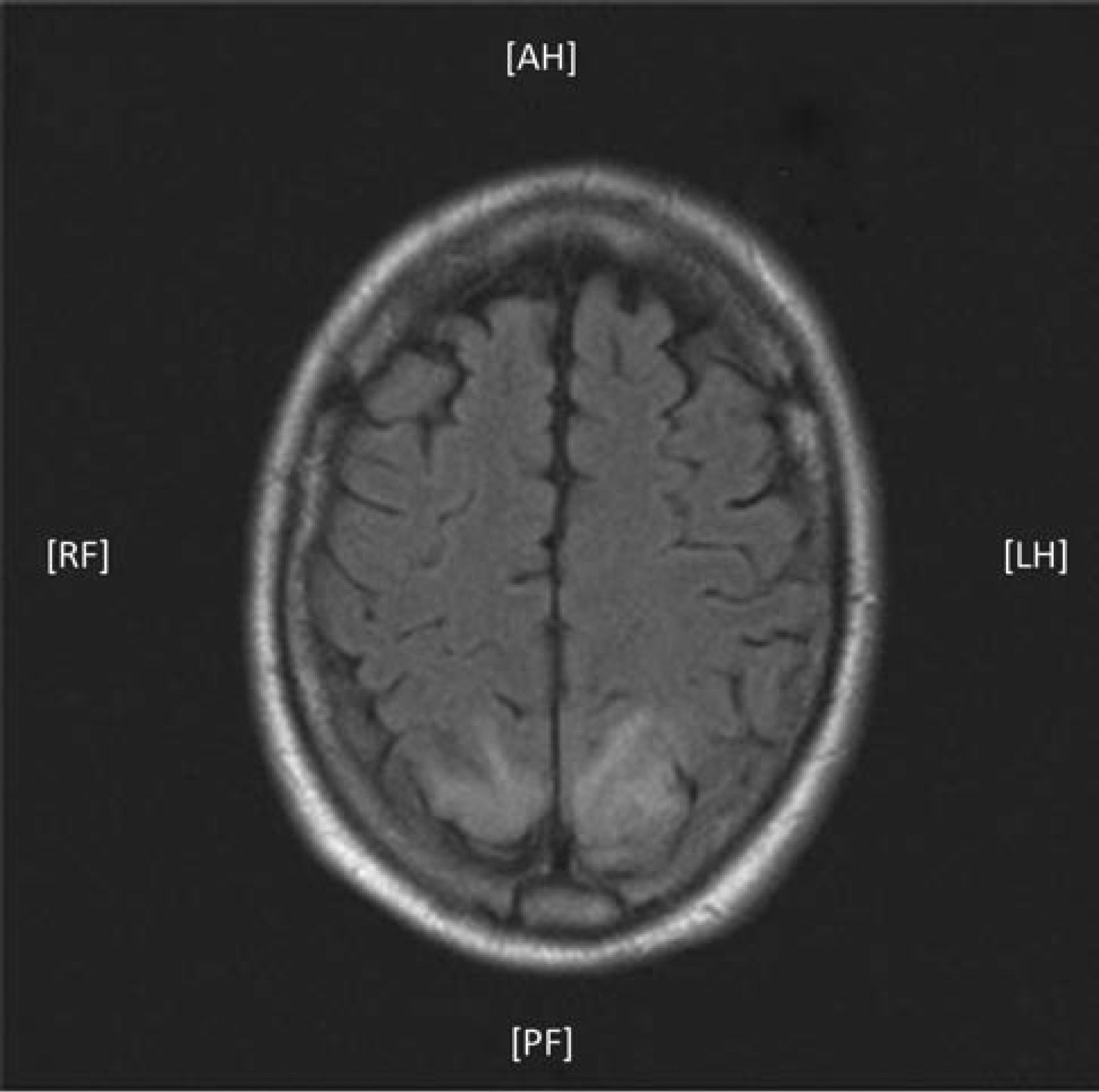
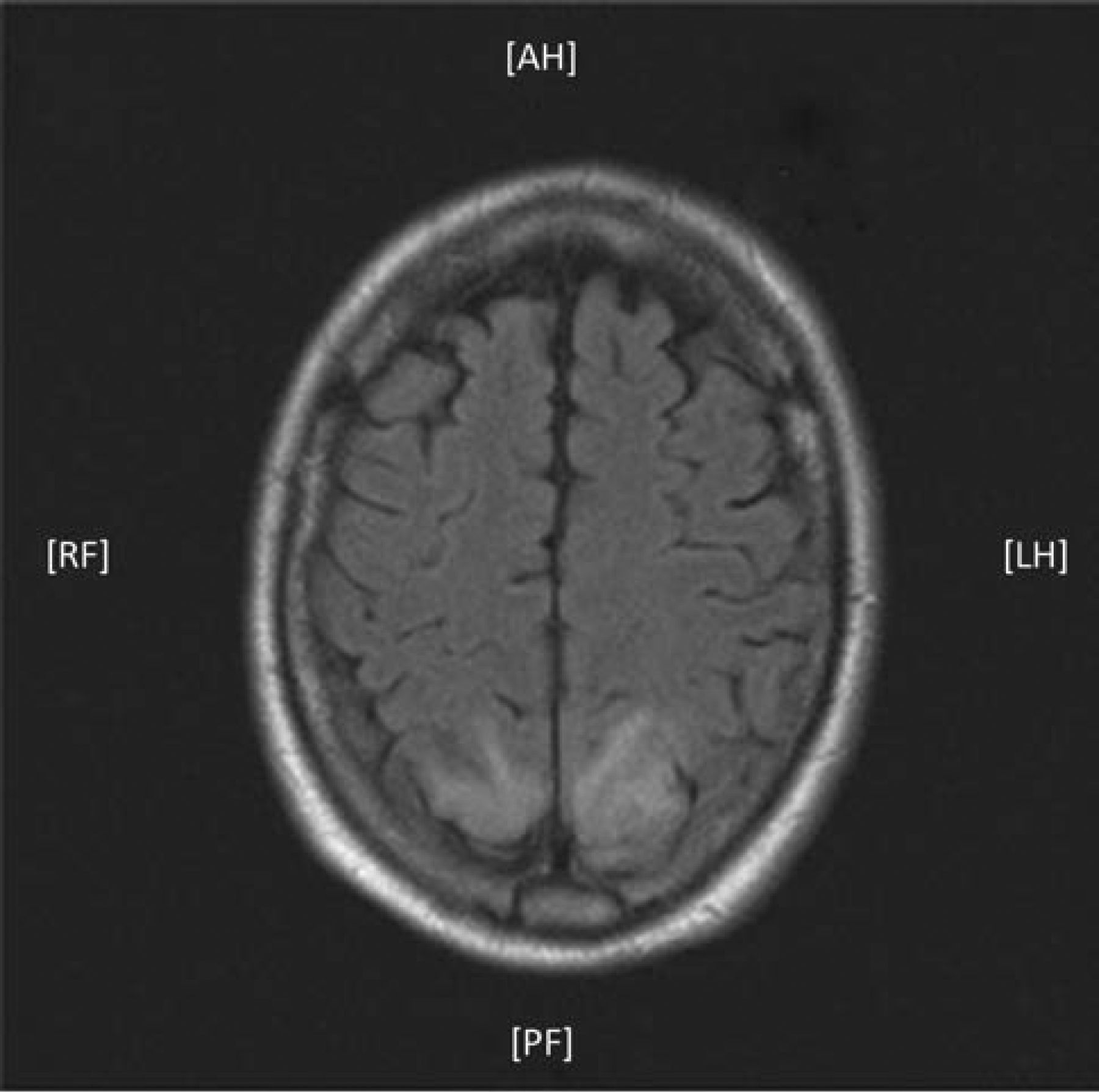
On day 7 of intensive care an MRI was performed, which demonstrated an increased signal intensity in the parietal lobes bilaterally in the watershed areas – appearances in keeping with infarcts (Fig 2). The patient's GCS improved steadily to 15/15 along with an improvement in his power to 5/5 by day 14 with general nursing care, chest and whole body physiotherapy. On discharge from the critical care environment he showed remarkable neurological recovery and recovered normal speech. There was no demonstrable long-term neurological impairment.
MRI scan shows bilateral areas of increased signal intensity in the watershed areas. MRI = magnetic resonance imaging.
In light of patient presentation, clinical course, the characteristic radiological findings and complete neurological recovery in consultation with the neurologist, a retrospective diagnosis of posterior reversible encephalopathy syndrome (PRES) was established.
Discussion
Posterior reversible encephalopathy syndrome (PRES) as a diagnosis has been known to exist for at least 15 years. It is a neurological syndrome characterised by typical clinical and radiological findings. Combinations of seizures, visual disturbance, headache and altered consciousness have been described as the key features and have been pointed out in previous case reports.1–3
Severe neurological deficit at presentation warrants a CT scan, but symmetrical hemispheric hypodensities, a classic feature of PRES, is only demonstrated in 50% of cases.1 In light of this MRI and fluid attenuated inversion recovery (FLAIR) imaging is arguably a better imaging modality, since the bilateral bright lesions provide a distinct picture.1,4 The final piece of the PRES puzzle is the rule of complete recovery from severe neurological deficit combined with radiological resolution in the subsequent weeks.1–3
The etiology and pathophysiology of PRES are still unclear. The first reported cases of PRES occurred in eclampsia/pre-eclampia of pregnancy.1 The most commonly reported cause has been acute changes in blood pressure; however, a variety of other conditions have also been associated with PRES, such as infection, sepsis, autoimmune diseases and following chemotherapy.
Evidence suggests that cerebral oedema is most likely vasogenic due to severe acute hypertension.1,4 However, a case report by Puglies et al in 2010 reported PRES occurring from hypotension.2 The absence of poor blood pressure control or infective/autoimmune cause in this case could suggest a still-unidentified cause for cereberal oedema,2 the classic feature of PRES on CT and/or MRI scans.
PRES characteristically resolves spontaneously with no neurological deficit in the presence of minimal or no definitive treatment.5 However, in the acute stage, when neurological compromise is at its greatest, supportive measures from critical care may be essential in facilitating complete recovery and avoiding any secondary insult. Facchini et al suggest the use of intracranial pressure (ICP) monitoring, along with goal-directed therapy for high-risk patients.5 Our case supports this suggestion that neuro-protective strategies may facilitate full recovery.
Conclusion
A key point that can be drawn from this case is that early suspicion of the diagnosis of PRES in the presence of the characteristic symmetrical radiological findings should prompt early escalation to institute measure to prevent secondary insult either in or outside the critical care environment.
Learning points
Posterior reversible encephalopathy syndrome (PRES) often demonstrates severe neurological disease, but complete patient recovery is the rule
To recognise PRES we need a low threshold of suspicion in patients who present with severe neurological deficit and bilateral symmetrical changes on imaging
Early recognition and admission to ICU is important to optimise recovery and prevent further brain injury
ICU = intensive care unit; PRES = posterior reversible encephalopathy syndrome.
- © 2014 Royal College of Physicians








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.