
A previously healthy 34-year-old man attended the medical outpatient ward with a 6-month history of shortness of breath, which was worse on exertion. The patient was a chronic smoker but there was no additional history of cough, sputum production, haemoptysis, fever or chest pain. On examination, the patient appeared pallid and had reduced tactile vocal fremitus and breath sounds bilaterally.
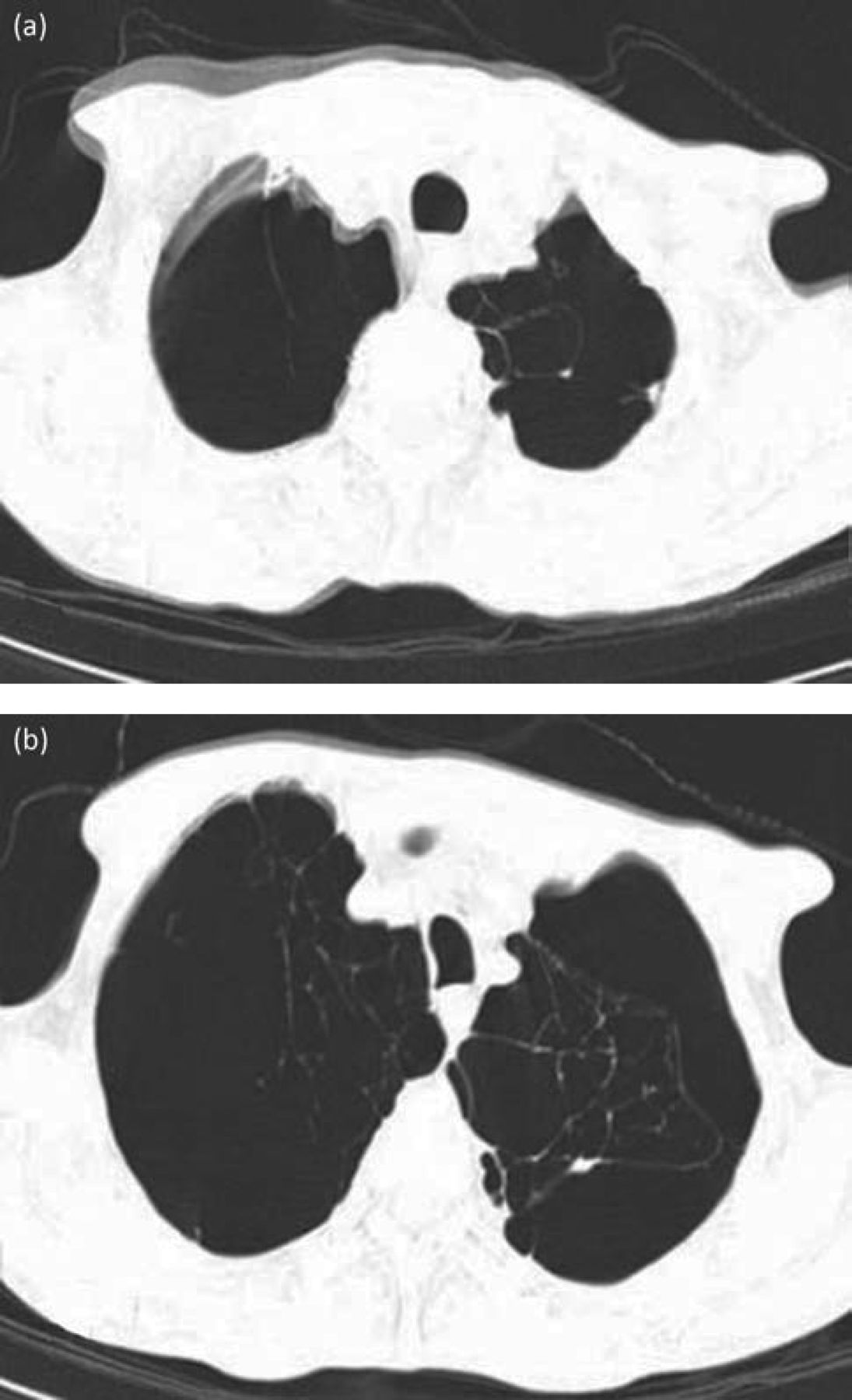
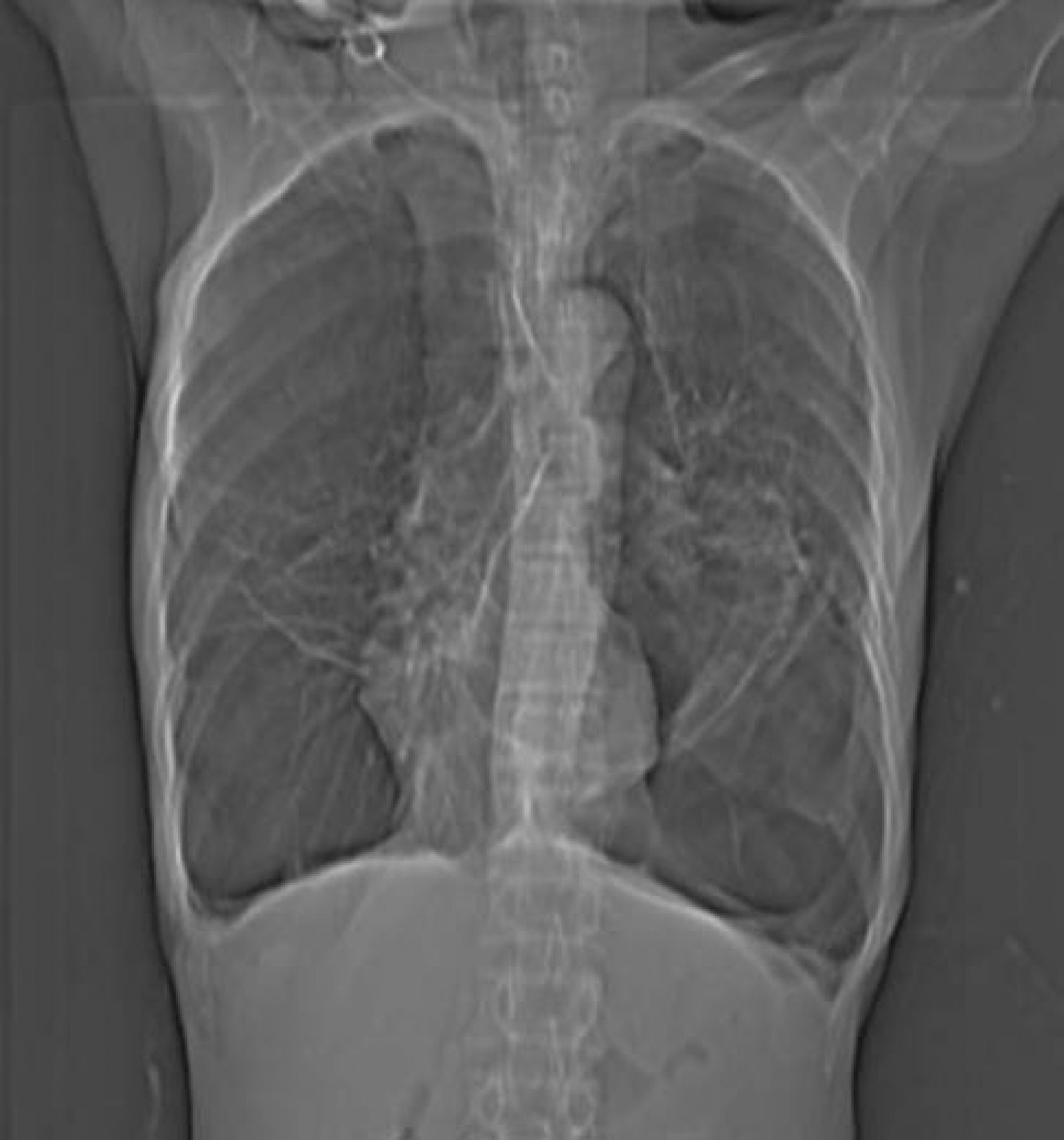
A plain chest X-ray revealed multiple bullae bilaterally (Fig 1). There was no tracheal or mediastinal displacement. A diagnosis of pneumothorax was considered and a tube thoracostomy was planned. A high resolution chest computed tomography (HRCT) scan was organised to confirm the diagnosis. However, this revealed multiple large bullae in bilateral lung fields with gross destruction of the pulmonary architecture (Fig 2 and 3). Pulmonary function tests demonstrated reduced lung volume and the presence of a restrictive deficit.
The diagnosis in this case was vanishing lung syndrome, first described by Burke et al in 1937.1 It is characterised by unilateral or bilateral asymmetric upper lobe involvement with the formation of multiple bullae. It is most commonly seen in young male smokers who present with progressive breathlessness. The pathogenesis of the disease revolves around the destruction of alveolar walls resulting in the formation of sub-pleural plebs with coalesce to create giant bullae and compression of normal lung tissue. The disease follows a downhill course, leading to respiratory failure and eventual death. It can be challenging to differentiate from pneumothorax, which imparts a similar appearance on plain chest X-ray. The ‘double wall sign’ seen in pneumothorax is due to air along both sides of the bullae and can be highly useful in distinguishing between the two entities.2
Treatment of the disease depends on the clinical picture. In the early stages, smoking cessation is important along with supportive management. Advanced cases require surgery. For our patient, a pneumonectomy was recommended, but the patient was not keen to proceed and was thus managed conservatively.

Axial HRCT of the chest through upper lung zones shows multiple bullae replacing the pulmonary architecture. HRCT = high resolution chest computed tomography.

Axial HRCT of the chest through lower lung zones showing giant bullae occupying more than one-third of hemithorax in bilateral lung bases. HRCT = high resolution chest computed tomography.

Frontal chest radiograph showing multiple bullae in bilateral lung fields. However, the possibility of pneumothorax cannot be excluded.
- © 2014 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.