
Abstract
The clotting screen is an ‘integral’ part of the routine blood tests in most medical wards. It is likely that only with the increasing requests for prothrombin time and activated partial thromboplastin time are abnormal results noted. Interpretation of these results requires good understanding of the coagulation system and problems with the laboratory analysis. Due to variable understanding of this complex system, many misconceptions have arisen in relation to the clinical effects expected from abnormal clotting screens. Some of these are discussed with considerations of appropriate management in those situations.
Introduction
A clotting or coagulation screen to include the prothrombin time (PT) and activated partial thromboplastin time (APTT) is often requested as a routine blood test. Several misconceptions have arisen with respect to the interpretation of clotting screen results. As these tests are meant to assess the coagulation system, abnormalities are considered to be markers of bleeding risk, especially with the possibility of clotting factor deficiencies such as haemophilia. In addition, to avoid any periprocedural ‘mishaps’, a clotting screen is considered a must, and an abnormal result needs correction with fresh frozen plasma before any interventions should go ahead. It is also thought that patients with liver disease and an abnormal clotting screen are at high risk of bleeding. Prolonged clotting results are also a contraindication for pharmacological thromboprophylaxis in hospitalised patients. On the contrary, one of the dreaded coagulation problems, disseminated intravascular coagulation, is considered unlikely in the absence of an abnormal clotting screen. These misconceptions are addressed further with reasons why they should be dispelled.
Prolonged PT and APTT predict the risk of bleeding
Prothrombin time was devised by a famous physician, Armand Quick, in the early part of the twentieth century, while investigating patients with obstructive jaundice.1 Soon after, the cause of haemophilia A was identified as due to the deficiency of coagulation factor VIII, but the PT was normal in these individuals with haemophilia.2 Further attempts to identify a test for haemophilia led to the development of the APTT test.3 Abnormalities of these two tests in families with bleeding tendencies led to the ‘discovery’ of several other coagulation factors and the creation of the coagulation cascade (which has been revised in recent years to the cell-based model of coagulation).4,5 Thus, the PT and APTT were created as a screening test to identify bleeding tendency in patients who may have haemophilia or deficiency of other coagulation factors. They were not devised to determine the bleeding risk in individuals with no personal or family history of bleeding. These tests were certainly not devised to assess bleeding tendencies in patients as a result of surgery or interventional procedures.
The notion that abnormal coagulation predicts bleeding has automatically led to the concept that any interventional procedures (line insertions or biopsies) require a normal clotting screen beforehand. In recent years, there have been several attempts to debunk this myth.6–9 These reports stress the fact that a good history from the patient or family, or their records, is most important in predicting bleeding risk. Anyone who has bled excessively after surgery or a dental extraction in the past is more likely to have a bleeding disorder. In older people, a repeat visit to hospital or the need for a prolonged hospital stay or blood transfusions after an operation would suggest an underlying bleeding disorder. In younger individuals or children, who have not had a surgical or traumatic challenge, a family history of bleeding might be relevant. Absence of personal or family history of bleeding means that the usefulness of a clotting screen is likely to be small.
The limited specificity of the tests for the low prevalence of bleeding disorders can result in a high number of false positives, but, worryingly, false negatives can also occur; these can lead to false reassurance.7 Hayward et al explored the use of PT and APTT among individuals referred for bleeding disorder assessments, using data from a bleeding disorder study to determine sensitivities and specificities. They identified that coagulation defects were uncommon and the APTT detected many non-significant abnormalities.10 Coagulation screening tests were less sensitive to clinically significant abnormalities (1.0–2.1%) compared with more specific tests such as the screen for von Willebrand's disease (6.7%). As most abnormal results can be predicted and significant bleeding disorders can be identified from a good clinical assessment, selective laboratory testing, including clotting screen and further evaluation of coagulation factor assays based on the history, is suggested as being more cost-effective.7,8 Recently, two important scoring tools have been created with the help of expert panels, which will guide in the clinical assessment of patients who may be considered to have bleeding disorders – the International Society of Thrombosis and Haemostasis/Standardization Sub Committee (ISTH/SSC) bleeding assessment tool and the Molecular and Clinical Markers for the Diagnosis and Management of Type 1 von Willebrand disease (MCMDM-1 VWD).11,12 The caveat to the above approach is that some patients may be unaware of bleeding complications from past procedures, especially if carried out when they were young children, and family members may not recall bleeding complications from interventions. Also, a poorly taken family history with no specific and direct questions to assess bleeding manifestations can be an issue.
Prolonged PT and APTT are due to inherited deficiency of clotting factors
So, if the PT and APTT do not predict bleeding risk in a person with an absent bleeding history, why do they become abnormal so often? Table 1 gives a list of the common causes of prolonged PT, APTT or both.13
Causes of abnormal prothrombin time, activated partial thromboplastin time and PT/APTT.
Prolonged PT
An isolated prolonged PT is mostly seen in individuals on warfarin or those who have vitamin K deficiency; in the former instance it is easily noted and discontinued or reversed, whereas in the latter it is easily corrected with replacement therapy. Factor assays are not needed in vitamin K deficiency in the right clinical setting, and if there is a response to vitamin K (eg chronic illness, malnutrition, abdominal surgery, long-term parenteral nutrition, liver disease, malabsorption states, and some drugs such as antibiotics and anticonvulsants). Those patients who have an abnormal PT due to liver disease do not require any special interventions to prevent bleeding as discussed later.14 Congenital deficiency of factor VII can affect the PT in isolation. Although fewer than normal factor VII values (normal values being >50 to 60) can prolong the PT, only levels of around 15 are haemostatically necessary.15 Although defects of the common pathway would be expected to prolong both tests, reagents vary in their sensitivity to different deficiencies, eg factor X deficiency is seen only with particular thromboplastin reagents.
Prolonged APTT
An isolated prolonged APTT is seen in patients with lupus anticoagulant, which interferes with the APTT test.13 Lupus anticoagulant is a very common phenomenon and is often noticed after an infection or inflammatory illness as a transient phenomenon. This is certainly the case in intensive care units, where abnormalities in the clotting screen are most often noted. Wenzel and colleagues looked at the incidence of lupus anticoagulant in critical care units and found an incidence as high as 53%.16 Lupus anticoagulants were found after a median stay of 13 days, with sepsis and/or catecholamine treatment being significantly associated with its development. Interestingly, lupus anticoagulant resolved spontaneously in 63% of the patients after a median stay of 17 days, confirming its transient nature. Rarely there are some inhibitors, which may or may not behave like lupus anticoagulant, that have their predominant effect on the PT due to the sensitivity of the reagent.
Unfractionated heparin, often used to lock central lines and in haemodialysis and filtration circuits, can affect the APTT. Although, low-molecular-weight heparins (LMWHs) are not often thought to affect the PT or APTT, this is not exclusively so. Ip and colleagues noted that three out of the eight APTT reagents that they tried were affected by LMWHs.17 A useful test to confirm whether the APTT prolongation is due to heparin is to perform a thrombin time which will be prolonged by heparin. Prolonged APTT can be seen with deficiencies of coagulation factors VIII and IX, and severe von Willebrand's disease, which are diagnosed in childhood although, very rarely, mild haemophilia and type I von Willebrand's disease often remain undiagnosed until adulthood. Factor XI deficiency can also cause prolonged APTT but may be missed because bleeding may occur only with major surgery. A family history of bleeding and Ashkenazi Jewish ancestry are helpful in this regard because it is an autosomal recessive condition, more commonly noted in individuals with the specific ancestry. Prolonged APTT can also be caused by deficiencies of factor XII, high-molecular-weight kininogen (HMWK) and prekallikrein (PK). Importantly, deficiencies of factors XII, HMWK or PK are NOT associated with bleeding, which is another reason why a good clinical history is relevant, where absent bleeding history but prolonged PT/APTT may lead to a delay in the planned procedures, pending detailed investigations.
Prolonged PT and APTT
Both the PT and the APTT will be prolonged in cases of vitamin K deficiency, liver disease, and a combination of the causes of isolated PT or APTT prolongation.13 In addition to liver disease and antibiotic therapy, any reason for gastrointestinal malfunction, including medical conditions (malabsorption, pancreatic disease, poor intake) or surgical interventions, can lead to vitamin K deficiency in a short period of time.18 Early vitamin K deficiency affects only the PT, not the APTT, despite the fact that the vitamin K-dependent factors (II, VII, IX and X) should affect both the intrinsic and the extrinsic pathways. This is due to the difference in the half-lives of the factors, whereby factor VII, the coagulation protein with the shortest half-life, is reduced earliest, reflected by a prolongation of the PT, whereas the reduction in the other factors takes more time, reflected by a delayed prolongation of the APTT in relation to the PT.
Increasingly, patients are being prescribed new oral anticoagulants, in place of warfarin, which can affect the PT or APTT or both. As these patients are at risk of bleeding, especially from the gastrointestinal tract (eg with dabigatran), patients who are bleeding while receiving these agents should be discussed with coagulation specialists.19,20 Table 2 summarises the effects that the new oral anticoagulant agents have on the PT and APTT and another clotting test, thrombin time.
The new oral anticoagulants and their effects on clotting screen.*
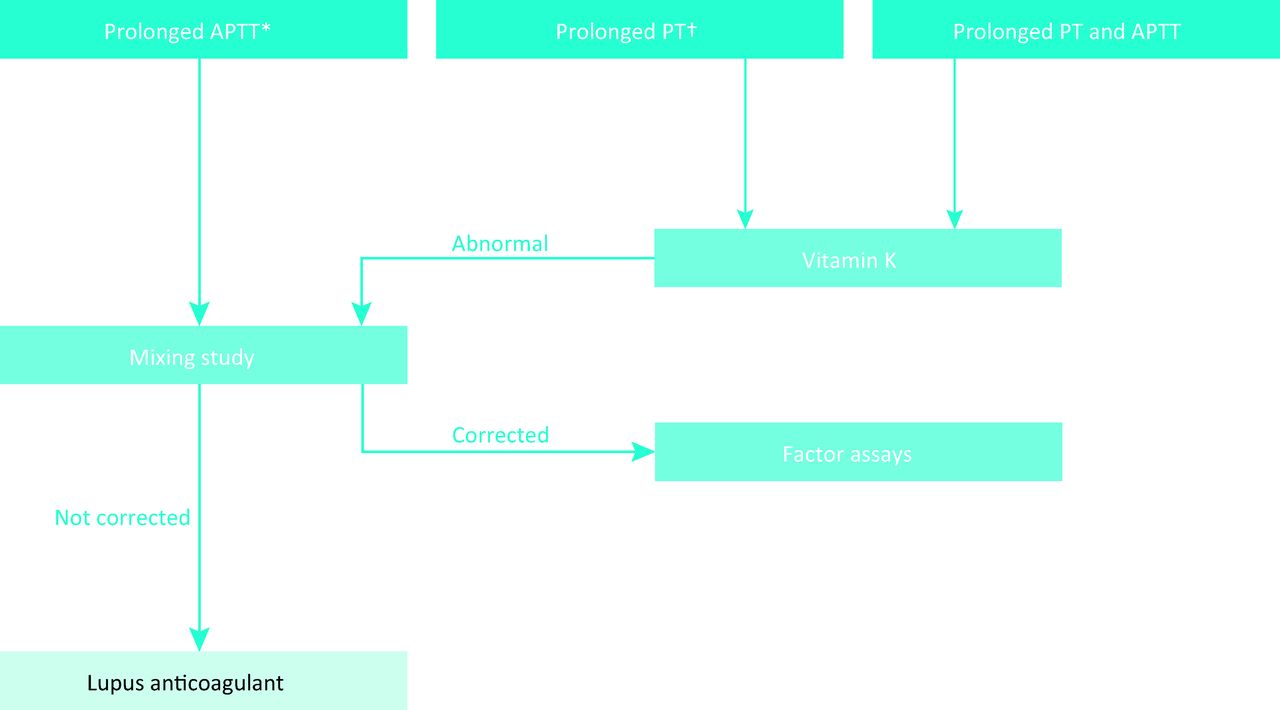
Investigation for prolonged prothrombin time (PT) or activated partial thromboplastin time (APTT) or both. In the case of an isolated prolonged PT, or both PT and APTT, intravenous vitamin K 10 mg may help in ‘diagnosing’ vitamin K deficiency and correct the abnormal tests. A mixing study involves mixing the plasma of an individual with known normal levels of coagulation factors with that of the patient. If the tests normalise it suggests deficiency of a clotting factor. If it does not, it suggests, commonly, lupus anticoagulant or, rarely, an inhibitor to coagulation factors. The latter is time and temperature dependent, ie an initial correction of APTT to normal may be noted but on continued incubation at 37°C, it becomes prolonged again. *One of the most common reasons for an abnormal APTT with a normal PT is inadequately filling the blood specimen tube. Repeating the test after ensuring that the specimen tube is appropriately filled is advisable before proceeding to further work-up. †Lupus anticoagulants can prolong the PT in some instances through anti-prothrombin activity. In such cases both the PT and the APTT are prolonged. PT = prothrombin time; APTT = activated partial thromboplastin time.
Preanalytical variables that can affect the clotting screen.
Patients with liver disease bleed due to abnormal PT and APTT
Patients with liver disease often have abnormal clotting screens. It has always been taught in medical schools that these patients are ‘auto-anticoagulated’ because their PT and APTT are often prolonged.22 It is no surprise that these tests are abnormal because the liver is the main organ for the synthesis of coagulation factors. However, in the same way, the liver also synthesizes all the endogenous coagulation inhibitors that exist in the circulation to regulate the clotting process. This simultaneous decrease in procoagulant and anticoagulant factors means that there is a balance in liver disease patients whereby they are not a higher risk of bleeding from the prolonged PT or APTT.23 Liver disease patients also often have thrombocytopenia and associated platelet dysfunction. However, Lisman and colleagues demonstrated that an increase in von Willebrand's factor, seen in these patients, may compensate for defects in platelet numbers.24 Although this research study has shown that platelet count and dysfunction may be clinically irrelevant in liver disease, this finding needs confirmation from prospective well-designed clinical trials before widespread acceptance.
This balanced haemostatic state in liver disease is evident from the fact that bleeding that often occurs in liver patients is related to variceal bleeding, when urgent gastroscopy is the best acute strategy rather than correction of an abnormal clotting screen.20 The other contributors to liver disease = related bleeding include associated renal impairment, sepsis and anaemia from bleeding itself.23,25,26 This paradigm shift in medical understanding is now well researched and several publications attest to the fact that abnormal PT and APTT in liver disease patients do not correlate with bleeding in any way.23,25,27 For this reason, fresh frozen plasma administration to correct these results is probably futile and will only delay any procedures that may need to be carried out urgently.27,28 In this regard, the position paper on liver biopsy of the American Association for the Study of Liver Diseases states: ‘the use of prophylactic or rescue strategies such as plasma, fibrinolysis inhibitors, or recombinant factors should be considered in specific situations, although their effectiveness remains to be established (Class IIa, Level C).’29
The exact contribution of coagulopathy in liver disease can be identified only by global coagulation assays that take into consideration the haemostatic system as a whole. which includes both the procoagulant and the anticoagulant factors. Although, currently, validated global coagulation testing is not yet available, the technique of TEG (elastography) or RoTEM (elastometry) or thrombin generation testing, available in some specialised laboratories, looks promising.30
Another caveat in this regard is the usage of the international normalised ratio (INR) in place of the PT as part of the clotting screen for patients with liver disease. It is often forgotten that the INR was created to standardise patients who receive warfarin across different laboratories and, for this reason, uses an international standard from patients stabilised on warfarin. As such, it is incorrect to use the INR in patients with liver disease, where the same standard cannot be used. There have been attempts to make an INRliver, although this does not yet have widespread acceptance.
Patients with disseminated intravascular coagulation have abnormal PT and APTT
Disseminated intravascular coagulation (DIC) is a clinicopathological syndrome, where over-activated procoagulant pathways from endothelial damage or over-abundance of circulating prothrombotic substances exceed the capacity of the endogenous anticoagulant mechanisms, resulting in excess thrombin. Activation of the coagulation system in DIC in the initial stages may cause a shortening of the APTT due to the high levels of coagulation factor VIII released from activated endothelium, and other factors such as elevated levels of von Willebrand's factor.31,32 In a study of 346 patients with DIC, factor VIII was elevated in most of the cases, with a decreased level noted in only 9% of patients studied.31 Interestingly, it has been reported that APTT and PT are abnormal only in <50% of the cases of DIC.33 By the time that a considerable prolongation of PT and APTT has occurred in cases of DIC, the consumption of clotting factors into the thrombi, disseminated to the different organs, would have become extreme. In support of the fact that DIC is a dynamic process, the International Society of Thrombosis and Haemostasis has suggested the use of a scoring system that has been recommended for purposes of DIC diagnosis34 (Table 4). As the coagulation screening tests are not very sensitive to the presence of DIC, a combination of tests is preferred and the choice of clotting test in the ISTH criteria is the PT, which is more likely to be affected than the APTT. An important message of this scoring system is that a change (prolongation) in the laboratory values is more important than the actual values of the PT in DIC.33,34 As in the other cases of abnormal clotting screen discussed before, when DIC can be diagnosed in the right clinical setting, fresh frozen plasma administration is NOT advisable unless active bleeding exists.35,36 In these situations, a PT or APTT ratio >1.5 is recommended as a threshold before considering transfusions, based on consensus.36
International Society of Thrombosis and Haemostasis (ISTH) diagnostic criteria to diagnose disseminated intravascular coagulation (DIC).
Conclusion
In conclusion, a better understanding of what the PT and APTT actually measure is important in providing better care to medical patients with abnormal clotting results. Most often, an elevated PT or APTT is not due to the inherited deficiency of coagulation factors. In individuals with an absent bleeding history, abnormal results do not signify an increased bleeding risk either. In a similar way, the concept that an abnormal clotting screen in patients with liver disease increases their bleeding risk is also a myth. On the contrary, one of the feared coagulation disturbances such as DIC can present without abnormal PT or APTT, and a changing trend in the laboratory values should be given more importance for its diagnosis.
Key points
Abnormal clotting screens do not predict bleeding risk and are also not always due to coagulation factor deficiency
Although the clotting screen is often abnormal in patients with liver disease, this does not correlate with bleeding in these patients
The clotting screen is often not abnormal in patients with disseminated intravascular coagulation
A simple scheme for investigation of prolonged PT and APTT is given in Fig 1. Several preanalytical variables need to be considered in the evaluation of the PT and APTT. These are given in Table 3. In these cases, repeating the tests taking these variables into account is crucial to avoid errors.21
- © 2014 Royal College of Physicians
References








{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- Prolonged PT and APTT predict the risk of bleeding
- Prolonged PT and APTT are due to inherited deficiency of clotting factors
- Patients with liver disease bleed due to abnormal PT and APTT
- Patients with disseminated intravascular coagulation have abnormal PT and APTT
- Conclusion
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.