
Knowing is not enough: we must apply. Being willing is not enough, we must do
Leonardo Da Vinci
Introduction
Around half the annual 600,000 deaths in England occur in hospital, with an average of 30 days spent as inpatients during the last year of life, over several admissions.1 Forty per cent of people who die in hospital may have no medical need to be there2 and most would not choose to die in hospital if their care could be delivered in an alternative setting.3 Most people who die in the UK are managed by their general practitioner (GP), together with a range of hospital specialists without referral to specialist palliative care services.
Delivering patient-centred care in the last months of life and enabling people to die in a place of their choosing requires individuals and their families to know that they may be approaching the end of life in good time to be involved in decision-making, and for community support to be in place. Honest conversations about limits of medical treatment must be part of routine care if patients are to have time to consider their choices, as outlined in the General Medical Council (GMC) guidance Treatment and care towards the end of life.4 This requires behavioural change in healthcare teams, influenced and led by consultants, acknowledging that clinicians are largely trained to cure or extend life.5 All physicians need to engage deeply in this challenging area of care and make it a routine part of their practice. Developing practice to embrace this requires more than the transfer of knowledge.
Senior doctors are accustomed to identifying their own learning needs. Recognising the need to change practice around palliative and end-of-life care (EoLC) may result from personal or professional experiences – good or bad – and the need to deliver enhanced curriculum requirements for trainees under their supervision.6
A range of learning opportunities is available, including e-learning,7 and local, regional and national training in EoLC.8 However, raising the bar in EoLC needs more than knowledge, and one-to-one work with specialist palliative care clinicians is a form of learning that is most highly valued.6 This may be a powerful way of learning, but is time intensive and palliative care clinicians do not always appreciate the issues in other specialties. This paper reports on an innovative development programme for senior clinicians that was designed and piloted in two trusts. Box 1 lists the questions to ask when evaluating EoLC.
Development programme in end-of-life care for senior clinicians
Led by consultants in palliative medicine, the pilot study used a range of methods including one-to-one work and action learning sets.
The aim was to enable consultants to identify their own learning needs, engage with the issues, undertake specific technical/clinical learning about palliative care and identify improvements in their own practice. Having increased their expertise, they would share and spread learning to clinical colleagues within their departments.
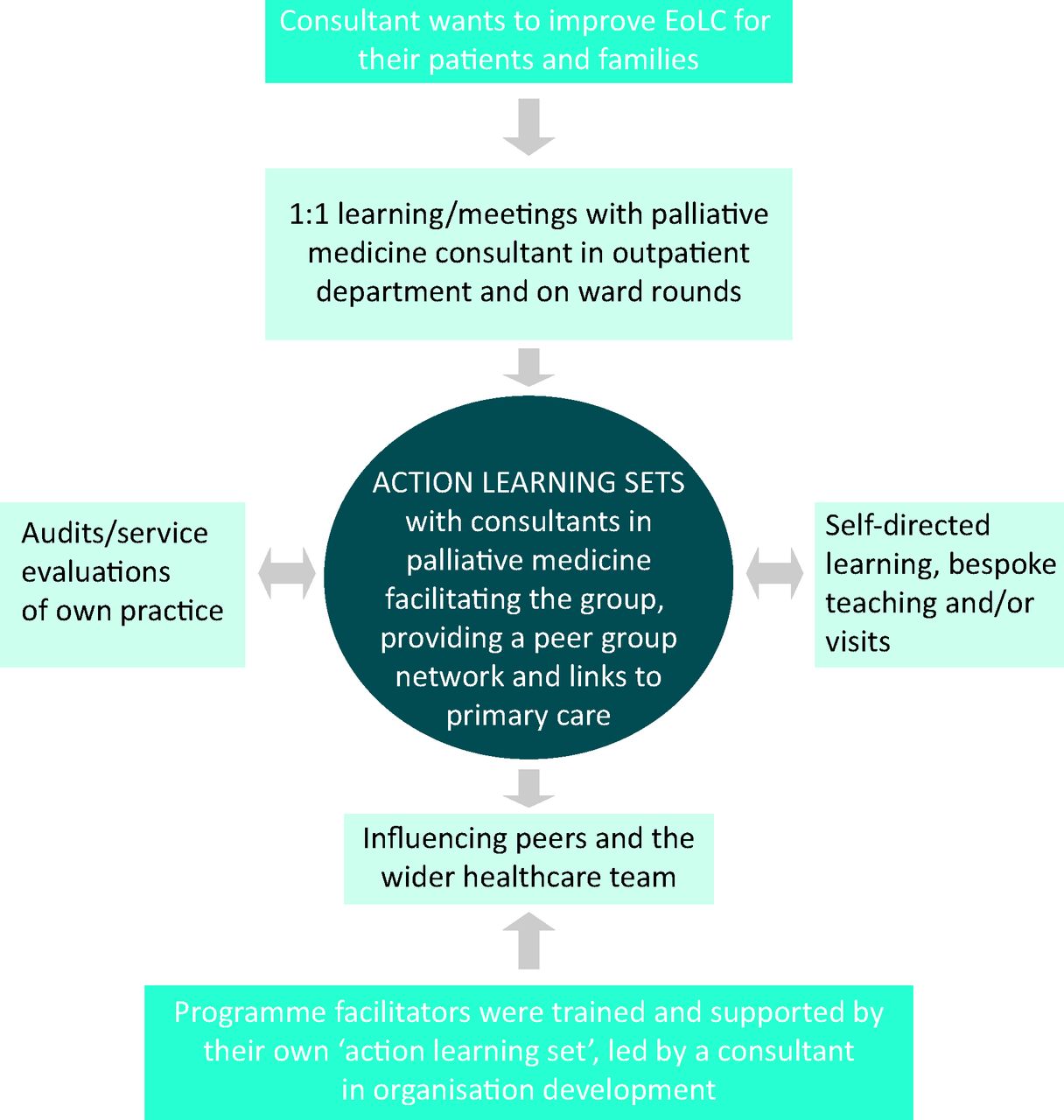
The programme was funded by the Yorkshire and Humber Strategic Health Authority (SHA) for two pilot trusts – one large teaching and one small district general hospital. Six or seven consultants from a range of specialties took part from each trust, with a GP to provide a community perspective. Each participant had a funded programmed activity (PA) for the first year and 0.5 PA for the last 6 months. Facilitation was provided by palliative medicine consultants with 2 PAs shared between them for each site, supported by monthly half-day meetings with a consultant in organisational development from the SHA.9 The programme was evaluated using training needs analyses at the start, middle and end, participant questionnaires collecting anonymous feedback, and audits of practice and service developments. Fig 1 outlines the programme schematically.

Schematic outline of the programme. EoLC = end-of-life care
Key elements of the programme
Individual focus
The facilitators worked with each clinician, attending clinics and ward rounds. This enabled them to see the challenges in practice – personal, clinical and organisational – and led to the development of a bespoke learning plan.
Senior clinicians
The programme was offered exclusively to consultants and senior specialty doctors who provided a natural peer group to explore sensitive and emotive topics. Providing care at the end of life touches us personally as well as professionally, with implications for those in senior medical roles that are rarely discussed. These doctors are in a position to lead change in their departments, working with consultant colleagues, juniors, nursing staff and the wider multidisciplinary team (MDT).
It is really lovely to feel the support of a group of colleagues who are all different but share similar work experiences.
Dedicated time
Provision of dedicated time enabled clinicians to examine their practice through private study, audits, service evaluations, organised teaching, group work and visits. As the programme progressed it enabled them to introduce changes in practice, present information at departmental and other meetings, develop guidelines, introduce new clinical tools, teach and model good practice to junior staff, and contribute to regional and national work.
Group working
The programme brought together senior doctors from a variety of medical and surgical specialties; many had never met although they worked in the same organisation. Shared experiences around delivering EoLC with areas of common ground were quick to emerge. The inclusion of a GP brought an important community perspective.
… the opportunity to meet with colleagues from a number of specialties and share solutions … I think we should suggest that this methodology could be used to address a number of different issues.
… our GPs’ comments and observations have been especially useful.
Action learning
The use of action learning was highly valued by participants, most of whom had never encountered it before. Provision of a ‘safe’ group for open discussion in an environment with appropriate challenges (sets) proved fruitful. Sets were well attended and colleagues readily contributed and challenged each other. Regular meetings provided the impetus to complete tasks as agreed.
The opportunity to discuss problems/issues with colleagues and find ways to ‘try out’ to improve care has been extremely valuable.
Trust board support
The support of the trust boards was a prerequisite of the programme. They agreed to provide practical help in job planning, access to relevant meetings to explain/promote the programme, and help to identify participants who were influential within their departments, motivated to complete the programme, but not necessarily the obvious choice. If institutional issues were uncovered, they undertook to provide active support and intervention to tackle them.
Outcomes
Examining individual practice
Each participant examined his or her own practice, what the staff were doing well and where improvements could be made, through peer discussion, audits and service reviews. A common theme was identifying people in the last year/days of life and judging the right time to initiate conversations about EoLC preferences, such as preferred place of care and death.
The prediction of terminal disease in patients with diagnoses other than cancer is much more difficult.
Examining learning needs
Participants developed their own learning plans but several common themes emerged. A number identified lack of confidence in talking about death and dying, so advanced communication skills training courses were run akin to the 2-day ‘Connected’ model.10
I am now much more open in discussing end-of-life care issues with patients and their relatives.
The primary/secondary care interface
At the outset there was little knowledge among hospital clinicians of systems in the community that support EoLC, leading to a lack of effective communication and coordination of care.
[My clinic/discharge letters had] lack of clarity about further treatment options and plans if they fail, lack of clarity about what I had discussed with patients, no clear steer to primary care about when to start planning end-of-life care and failure to communicate with district nurses.
Clinic and discharge letters now include information about prognosis and EoLC planning. Systems designed to embed this within routine practice are being developed and implemented in a number of specialties. In addition to identifying the need for such changes, the participants themselves worked together to make the necessary improvements, ie changing practice.
Confidence in community-based care
Concern was expressed at the outset that community services can be fragmented and may not manage some of the complex patients currently receiving EoLC in hospital. Visits to community staff helped hospital doctors to see what was available and increased their confidence in the ability of services to cope. Hospital clinic and discharge letters are now copied or sent on to district nurses who coordinate care for patients at home. Closer working has also been evident with community and hospital specialist palliative care services.
Box 1. Evaluating individual practice in end-of-life care.

Increased knowledge of … community care … more willing to put plans in place to prevent hospital readmission.
Systems and tools
Clinicians reviewed departmental systems to enhance EoLC for patients and families. For example, team mortality and morbidity meetings have been altered to include a holistic review of care against the aims of the EoLC strategy, rather than focusing on the narrower ‘medical model’. A checklist has been introduced to post-take ward rounds on the stroke unit to prompt decisions on ceilings of care, and patient and carer information has been made available on wards and in outpatients.
Comments about missed opportunities to avoid hospital admission, delays in initiating end-of-life care until after expensive and unnecessary investigations are now a regular feature of our mortality and morbidity meetings.
In addition, participants have embraced the ‘Transforming end-of-life care in acute hospitals’11 national programme, leading implementation of new tools in their wards and departments.
Self-confidence
Participants have grown in confidence, influencing colleagues who may be more senior than themselves, and trusting the process of action learning. They have debated areas of ‘accepted practice’ by bringing issues to the group, finding where they are of common concern, learning from each other's areas of expertise, reaching agreement and having the confidence to challenge others’ decisions.
Becoming experts
Participants have developed expertise in the end-of-life aspects of care for their patient groups – largely those with non-malignant conditions. Colleagues now look to them to share their expertise within their departments.
Transfer of changes across the multidisciplinary team and junior staff
Participants are working with nursing and other MDT colleagues to implement changes on wards and outpatients. They influence junior staff through modelling good practice, communicating with primary care, setting expectations around discharge and clinic letters, changing the focus of some departmental meetings and delivering formal teaching sessions. New MDT meetings have been developed.
… one of the major changes is the impact that it is having on junior doctors. Junior doctors are certainly influenced by the way their supervising consultants practise. I have had a number of juniors come and talk to me about EoLC issues and potential projects.
Trust-wide influence
Participants have become an expert reference group for delivering improvements to EoLC within their trusts, contributing to diverse projects such as a survey of bereaved carers and DNACPR (do not attempt cardiopulmonary resuscitation) implementation.
Key points
Learning with peers in a well-facilitated experiential action learning set has produced improvement in the identification of the end of life, communication skills and knowledge about end-of-life care (EoLC)
Specific audits and service evaluations looking at the experience of patients and families in EoLC lead to changes in service delivery by senior clinicians
Increased understanding of community services leads to systematic improvements in communication with primary care, including EoLC wishes and advance care planning
Consultants in many specialties can become an expert resource in EoLC and influence colleagues, junior doctors and the wider team in the best practice of EoLC
The combination of bespoke one-to-one work and action learning can produce substantial changes to clinical practice in this challenging area of medicine
- © 2014 Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.