
Abstract
Cholesterol embolisation syndrome (CES) is a rare but serious disease with high mortality caused by the formation of an embolus made up of cholesterol crystals from atherosclerotic plaques. Its clinical presentation is usually initially insidious and it often remains unrecognised because of its non-specific clinical presentation, which can cause delays in treatment and high mortality. The most common physical symptoms are cutaneous. We present a lethal case of CES to increase the awareness about this serious condition.
Case
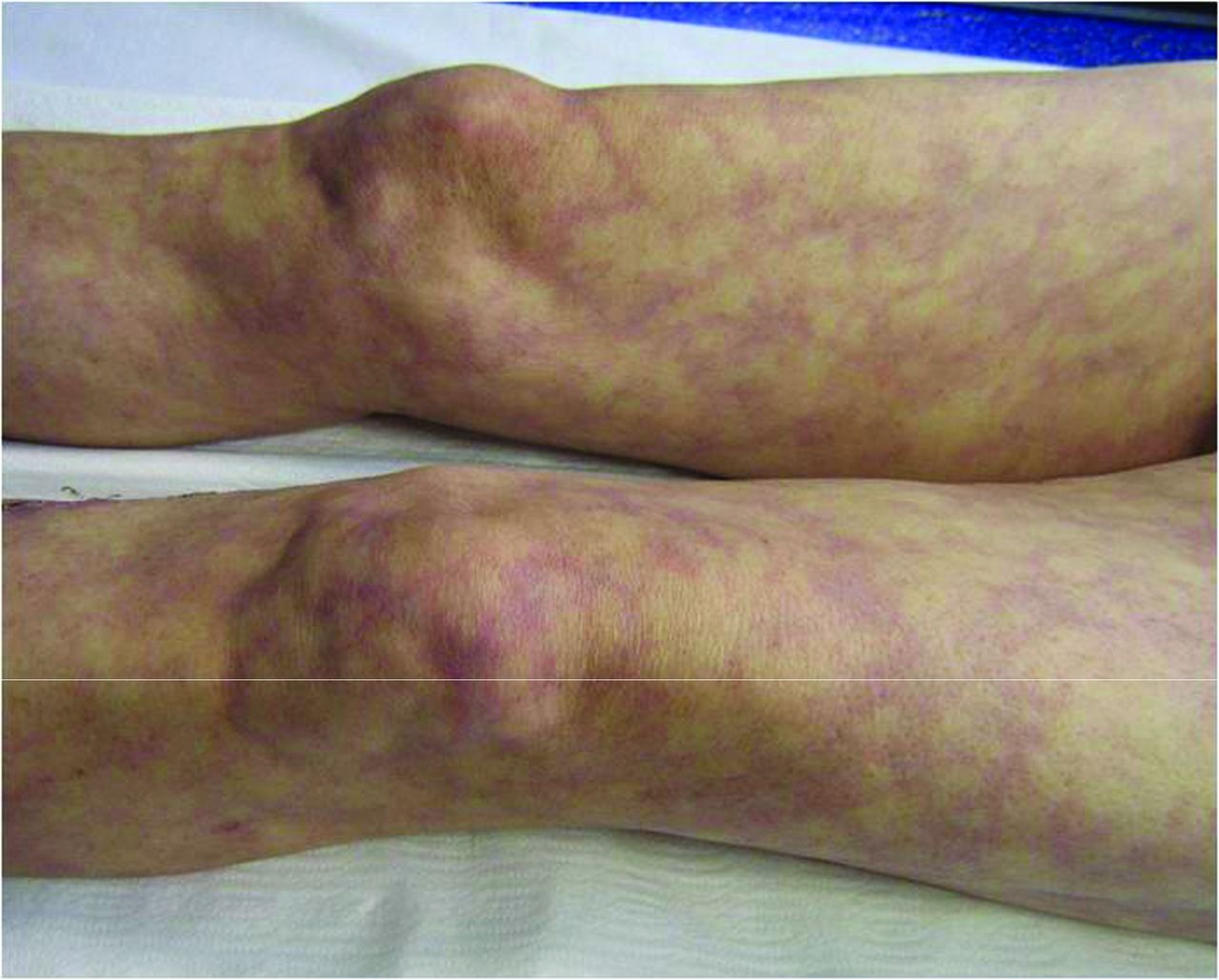
A 65-year-old male presented with a livedoid eruption on the trunk and lower extremities, and cyanosis that had been present for 10 days. He had had a myocardial infarction (MI) 7 weeks earlier. Following the MI, coronary angiography and coronary artery bypass surgery were performed. The patient was being treated with anticoagulant therapy. Dermatological examination revealed cyanosis at the bilateral toes and plantar sides, and livedo reticularis on the bilateral lower extremities and trunk, which became evident after standing for a while (Fig 1–2). Despite cyanotic toes, the patient's peripheral pulses were intact. Laboratory examination revealed acute elevation of serum creatinine at 1.73 mg/dl (0.7–1.2 mg/dl). Histopathological examination of skin biopsy was consistent with a vasculopathic reaction. Cholesterol particles were detected in vitreus during ophthalmological examination. With these clinical findings a diagnosis of cholesterol embolisation syndrome (CES) was made and the patient was hospitalised. Anticoagulant therapy was discontinued, statins were administered and supportive measures were provided. Within 4 days of hospitalisation, the patient was intubated due to the sudden onset of severe dyspnea and haemoptysis. During the patient's time in hospital cardiopulmonary functions deteriorated, renal functions worsened and hemodialysis treatment was started. On day 45 day of hospitalisation the patient died due to multi-organ failure.

Cyanosis at bilateral toes and both plantar sides immediately after standing for a while.
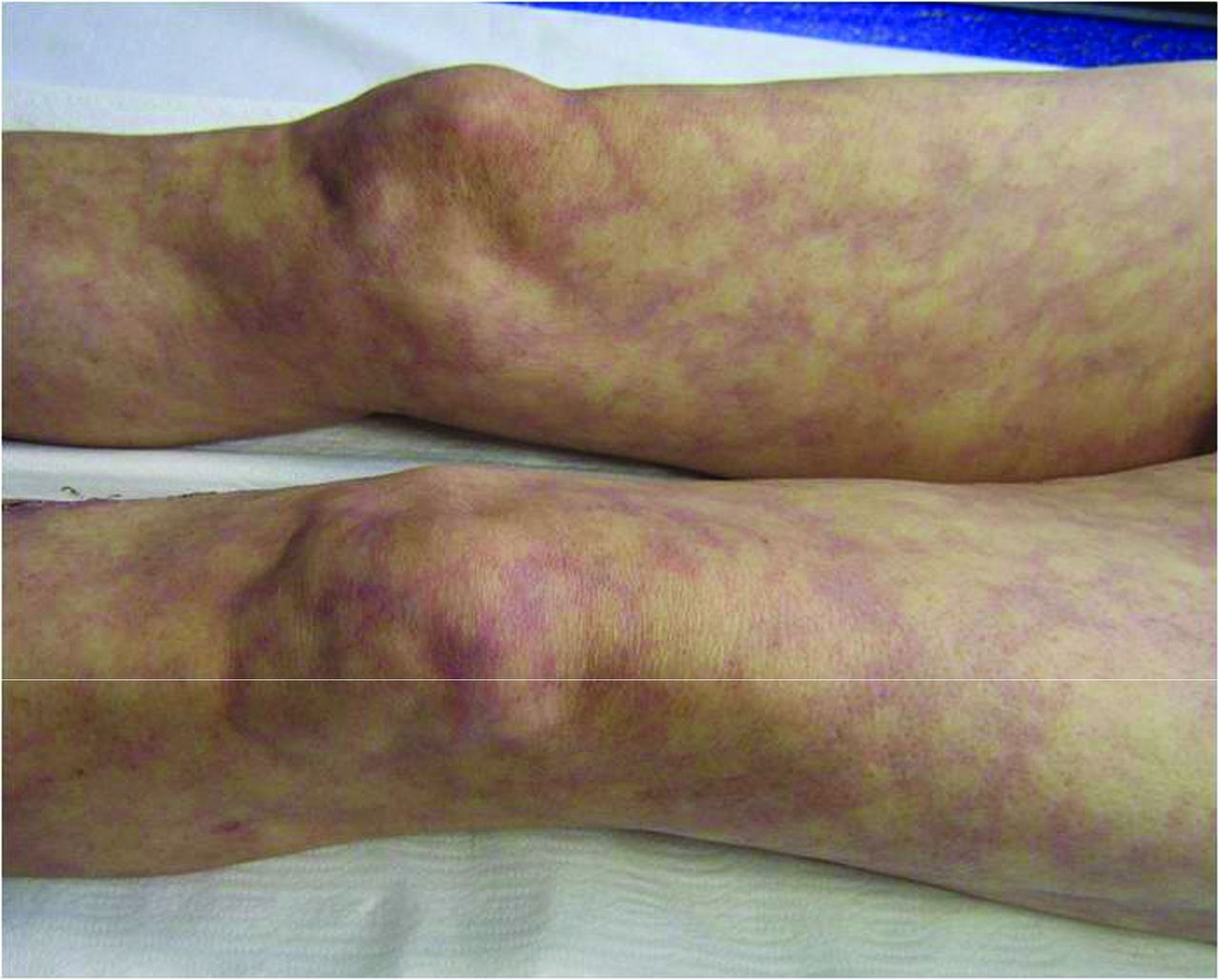
Livedo reticularis on bilateral lower limbs immediately after standing for a while.
Discussion
Cholesterol embolisation syndrome (CES) is a rare but serious disease with high mortality caused by the embolisation of cholesterol crystals from atherosclerotic plaques.1,2 It is mainly seen in males aged over 60 years who are suffering from atherosclerosis.2,3 Although it can occur sporadically (in 20% of cases), it usually develops after iatrogenic manipulation via invasive vascular procedures such as arteriography, angioplasty, surgery or drug therapies such as anticoagulants or thrombolytics.4 Although any organ can be involved in CES, the most commonly affected organ systems include the skin, kidneys and gastrointestinal system.5
Cutaneous manifestations are observed with a frequency ranging from 35% to 100% in different studies and mostly include livedo reticularis, cyanosis and ulcerations. Occasionally, a few nodules or purpura may ocur.6–8 In almost all cases the lower extremities are affected. Livedo reticularis, the most common cutaneous symptom, develops suddenly and bilaterally in the majority of cases. It can extend to the thighs, trunk or even the arms.6 In some cases cutaneous signs can be subtle and, as in this case, may become more evident in an upright position.9 A typical clinical sign of CES is normal distal pulsation as is found in this case.8
Laboratory findings of CES are generally non-specific and are related to the end organ damage and inflammation. A histopathological hallmark of CES is the presence of cholesterol clefts in the lumen of blood vessels.6,8 These clefts are distributed focally and are therefore difficult to find; often a deep biopsy of multiple sections is needed to reveal them. In many instances only fibrin thrombi are observed.8 Therefore, whether histopathological confirmation is necessary for diagnosis is debatable. The presence of a classical triad of precipitating events (vascular intervention or procedure), renal insufficiency and cutaneous findings mimicking vasculitis suggests a diagnosis of CES.4,10
The overall mortality rate of CES is 60–87%, and the cause of death is usually multifactorial.2 Early diagnosis and aggressive supportive care are suggested to be associated with reduced mortality.2 As yet there is no specific treatment of CES. Further vascular procedures and treatment with anticoagulants is recommended to be discontinued because they may aggravate or worsen the disease. Hydration, control of hypertension and haemodialysis has been reported to help lessen organ damage.10 Although not proven, pentoxifylline, statins and high-dose corticosteroids have been suggested to have a potential benefit in the treatment of CES.6,10
Conclusion
The diagnosis of CES should be considered in patients with underlying atherosclerotic disease who develop vasculitis-like cutaneous signs with unexplained renal impairment, especially after vascular procedures such as arteriography, angioplasty or surgery or therapies such as anticoagulants or thrombolytics. Cutaneous signs can be subtle and, as in this case, may be more evident in an upright position. We believe that recognition of cutaneous findings may help early diagnosis of this serious disease.
- © 2014 Royal College of Physicians








{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.