
Editor – We read with interest the article by Leong et al exploring complication rates in the 12 weeks after pacemaker implantation in a UK district hospital (Clin Med February 2014 pp 34–7). We highlight a later complication that can occur and how to avoid it using a technique which will also be of interest to all physicians performing central venous access techniques.
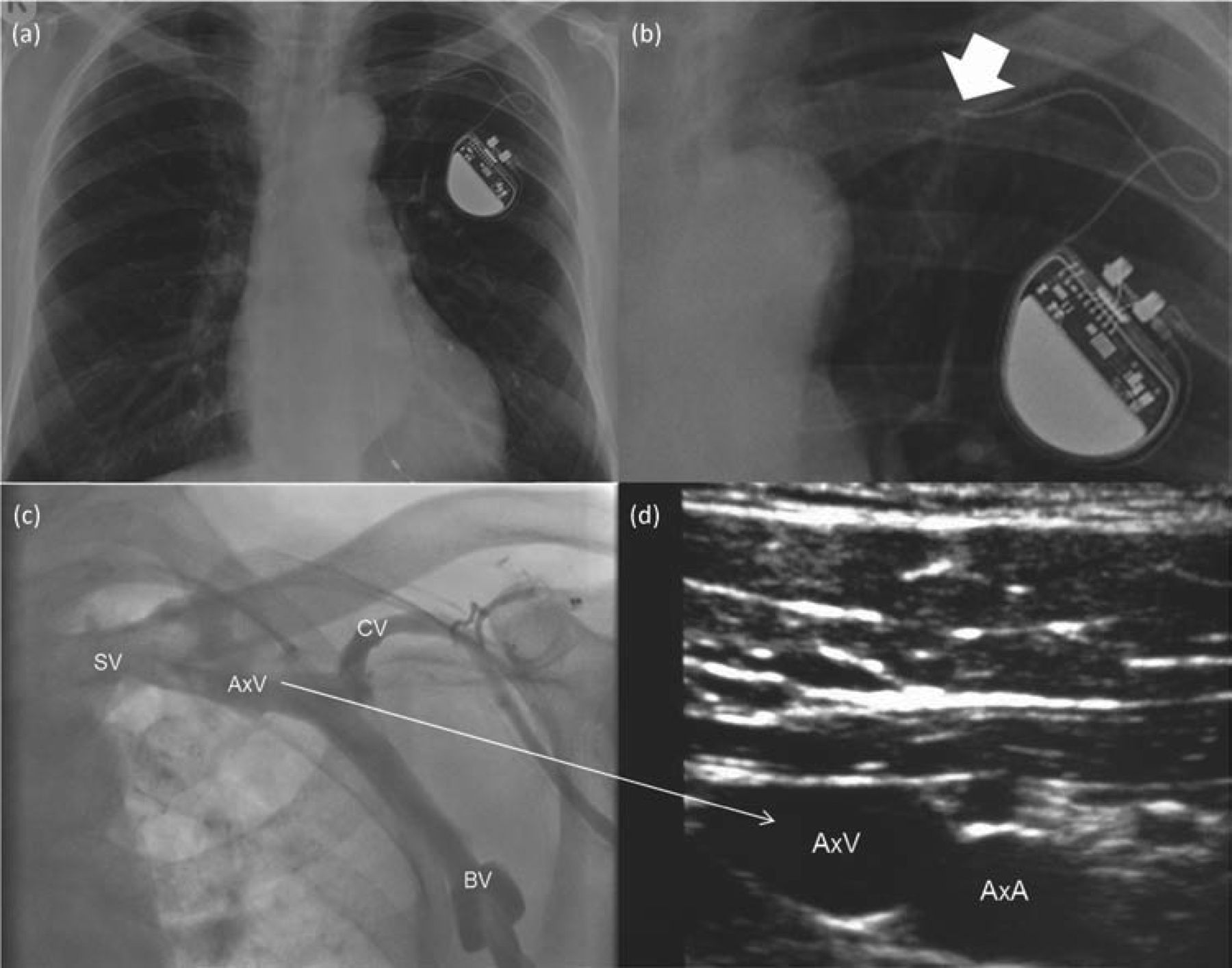
In the Leong study the subclavian vein was the most frequent route utilised for venous access. As found in this study there is a small risk of pneumothorax. However, in the longer term it also conveys a small risk of a ‘crush’ injury to the pacemaker lead.1 This is thought to be a result of pressure exerted between the first rib and the clavicle on the lead just before it enters the vein. The first author of this letter has experience of this complication, resulting in transection (Fig 1a and b).
A different approach utilises the axillary vein (Fig 1c). As the puncture is extra-thoracic, there is no longer a risk of crush injury and the risk of pneumothorax is reduced. A number of methods allowing access to this vessel have been described. It can be identified using ultrasound (Fig 1d) with a number of papers describing ultrasound guided insertion with up to 100% success rates, short operator learning curves and low complication rates.2,3 Various fluoroscopic approaches have been described with very high success rates.4
We therefore believe that axillary venous access is safe, useful, easy to learn and therefore of use to all physicians performing central venous access techniques.
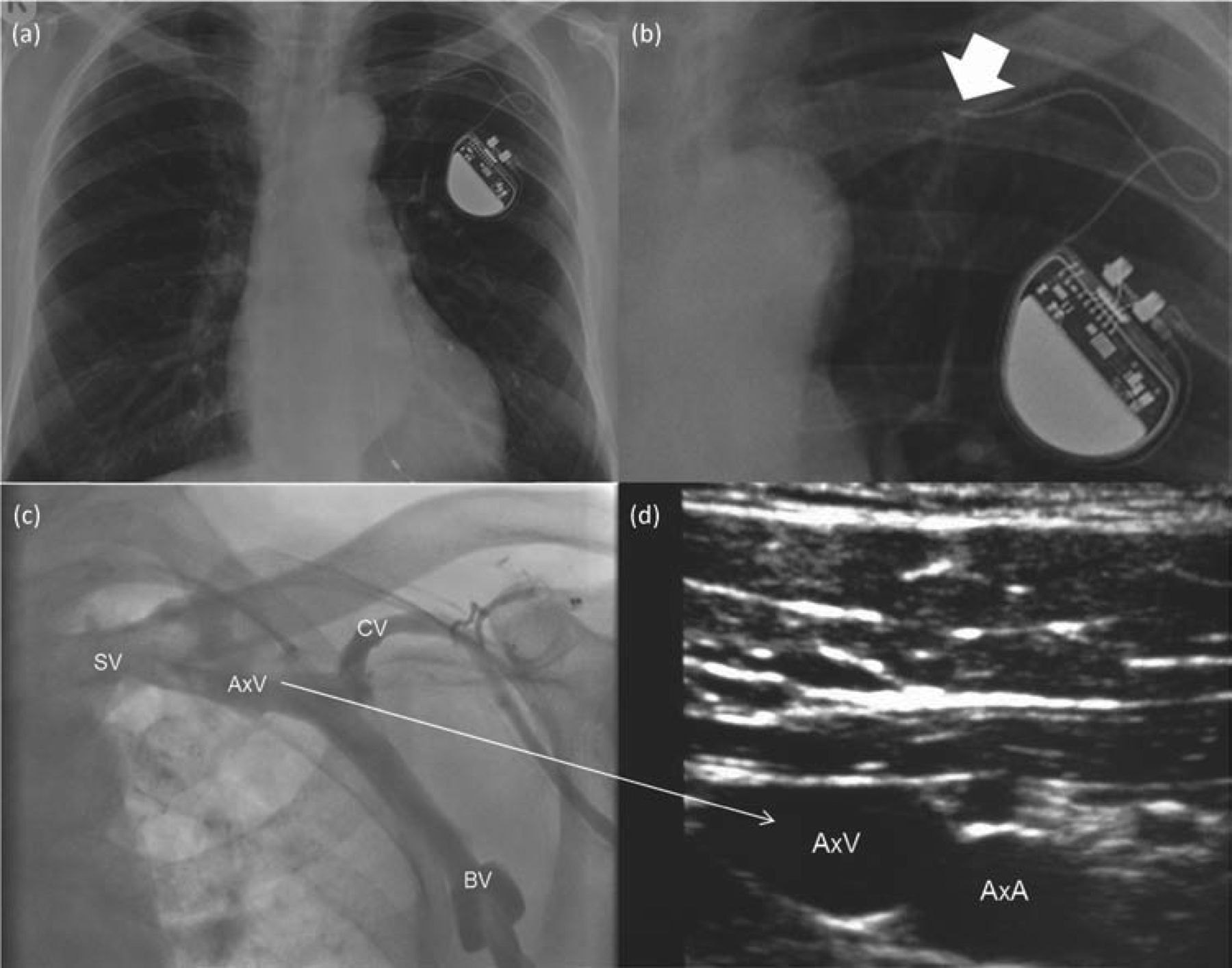
(a) and (b) A crush injury a number of months following insertion of a right ventricular pacemaker lead. The lead is transected (arrow). (c) Venogram showing the basilic (BV), cephalic (CV), axillary (AxV) and subclavian (SV) veins. (d) Ultrasound taken at the level shown by the arrow showing the axillary artery (AxA) and vein. The venous nature of the vessel is confirmed using colour doppler and its compressibility under pressure applied to the probe.
Footnotes
Please submit letters for the editor's consideration within three weeks of receipt of Clinical Medicine. Letters should ideally be limited to 350 words, and sent by email to: clinicalmedicine{at}rcplondon.ac.uk
- © 2014 Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.