
Abstract
Intensive care is celebrating its 60th anniversary this year. The concept arose from the devastating Copenhagen polio epidemic of 1952, which resulted in hundreds of victims experiencing respiratory and bulbar failure. Over 300 patients required artificial ventilation for several weeks. This was provided by 1,000 medical and dental students who were employed to hand ventilate the lungs of these patients via tracheostomies. By 1953, Bjorn Ibsen, the anaesthetist who had suggested that positive pressure ventilation should be the treatment of choice during the epidemic, had set up the first intensive care unit (ICU) in Europe, gathering together physicians and physiologists to manage sick patients – many would consider him to be the ‘father’ of intensive care. Here, we discuss the events surrounding the 1952 polio epidemic, the subsequent development of ICUs throughout the UK, the changes that have occurred in intensive care over the past 10 years and what the future holds for the specialty.
The history of intensive care
The polio epidemic in Copenhagen resulted in 316 patients developing respiratory muscle paralysis and/or bulbar palsy, with subsequent respiratory failure and pooling of secretions. The Blegham Hospital, the hospital in Copenhagen for communicable diseases, had only one tank respirator (Fig 1) and six cuirass respirators (Fig 2) at the time. This was completely inadequate to support the hundreds of polio patients with respiratory failure and bulbar palsy. The mortality rate from polio with respiratory failure and bulbar involvement was historically 85–90% and, as the epidemic progressed, the situation looked desperate.

Coventry alligator iron lung.

Cuirass shell ventilator.
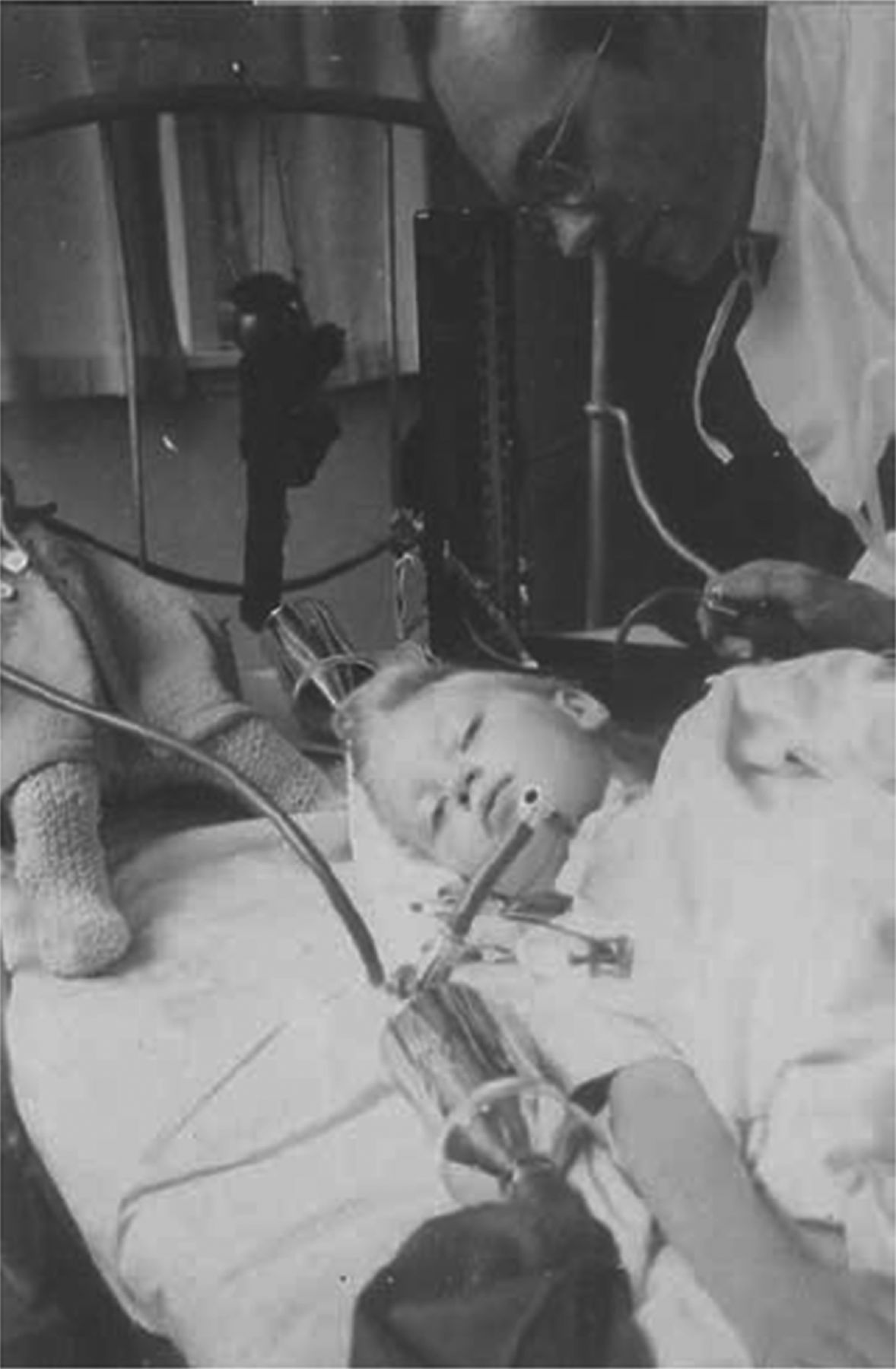
Professor Lassen, chief physician at the Blegdam Hospital, had a strong desire to provide treatment for all polio victims, despite insufficient respirators, and therefore consulted with Dr Bjorn Ibsen, a Copenhagen anaesthetist. Professor Lassen hoped that positive pressure ventilation, as used in modern anaesthesia at that time, might be a solution.1 Two days later, a 12-year-old girl with polio and resultant respiratory failure and bulbar palsy had a tracheostomy formed just below the larynx: a rubber cuffed tracheostomy tube was inserted and positive pressure ventilation successfully delivered manually with a rubber bag (Fig 3). Tracheostomies had been performed in Copenhagen for 4 years before this, but with little beneficial effect on outcome.

An 8-year-old girl being hand ventilated via a tracheostomy.
As a result of this success, it became possible for the medical team in Copenhagen to treat potentially every patient admitted with polio. At the height of the epidemic, over 300 such patients were admitted per week, 30–50 per day, with approximately 10% either ‘suffocating or drowning in their own secretions.’1 At times, there were over 70 patients in the hospital requiring respiratory support. Teams of medical students were drafted in and paid £1.50 per shift: 250 medical students came in daily and worked shifts with 35–40 doctors. By using such a strategy, mortality from polio in Copenhagen decreased from over 80% to approximately 40%.
Dr Ibsen had the idea of caring for all such patients in a dedicated ward, where each patient could have their own nurse. Thus, in December 1953, the specialty of intensive care was born.2
Dr Henning Sund Kristensen took over the running of this Copenhagen intensive care unit (ICU) following the epidemic; many patients did not regain respiratory function and required long-term ventilation. Adjusting such ventilation, using blood gas analysis, was made possible by the invention of the first pH, pCO2 and pO2 electrodes by Astrup, Siggard-Anderson and Severinghaus. That the technology of pH monitoring was developed by the Danish brewing industry and, in particular, by the Carlsberg factory in Copenhagen, greatly helped Dr Kristensen and his team. This, together with regular involvement of physiotherapists, improved survival rates further for patients requiring long-term ventilation. It rapidly became clear that teamwork was a vital component of high-quality intensive care.
Max Harry Weil is considered widely as the ‘father of modern intensive care’ – he established a four-bed ‘shock ward’ at Los Angeles County/University of Southern California Medical Center in the USA during the early 1960s.3 During the 1960s and 1970s, ICUs were established in the UK. This was aided by rapid expansion in consultant anaesthetists during the late 1950s, together with an increase in junior anaesthetists who could staff such units around the clock. In the UK, the first full-time intensive care clinician was Professor Ron Bradley, who ran the ICU at St Thomas’ Hospital, London. This ICU, known as Mead Ward, had initially been set up by Dr Geoffrey Spencer in 1966.4 Professor Bradley worked there with Dr Margaret Branthwaite, who herself went on to lead the ICU at the Royal Brompton Hospital, and together they developed the first pulmonary artery catheter.4 The first microprocessor-controlled ventilator was developed in 1971 and this, along with the development of a multitude of new equipment and drugs, stimulated a rapid growth of intensive care medicine.
Over the following 20 years, the specialty grew into the multidisciplinary discipline that it is today, with dedicated ICU nurses, physiotherapists, pharmacists, dieticians, technicians, radiologists and microbiologists. A specific scoring system, the Acute Physiology and Chronic Health Evaluation II score, or APACHE II score, was developed during the 1980s; this enabled case-mix adjustment, which was essential when comparing cohorts in research studies.5 In the UK, the Intensive Care National Audit and Research Centre (ICNARC) was established in 1994.6 From 2000, the number of high-dependency unit (HDU) beds started to increase, the concept of outreach teams and follow-up clinics started, and difficult ethical decisions became increasingly common.4
Developments over the past 10 years
The ability to support temporarily and, in some cases, replace the function of multiple-organ systems in the face of critical illness and injury is the core capability that underpins intensive care medicine. As a result, medical interventions in intensive care are more numerous and more invasive than those in the general ward setting, and the physiology of the critically ill patient is often fragile. This leaves ICU patients particularly vulnerable to iatrogenic harm.
More recently, there has been a ‘less is more’ shift in many intensive care interventions. Lung protective mechanical ventilation strategies, using lower tidal volumes and lower peak and plateau airway pressures, cause less injury to a patient's lungs.7 Supranormal oxygen values are now considered harmful, although recent evidence supporting this in patients who have had a cardiac arrest is controversial.8 We accept lower mean arterial blood pressure and cardiac output values than we did 10 years ago.9–11 Patients are sedated less heavily than they were in the past, with the aim of keeping them comfortable instead of comatose,12 and daily sedation holds are undertaken where possible.13 We transfuse less blood14 and it has been suggested that we should give less nutrition.15
A culture of quality improvement has become standard, with more reliable care, the use of care bundles and ‘doing the simple things well’ to make patient care safer.16 Care bundles are groups of four to five measures that, when performed together, have been shown to improve outcome: the two most established care bundles in intensive care concern the care of the ventilated patient and the central venous catheter (CVC). Previously, hospital-acquired infections were common in ICU patients because of their reduced immune system function, use of multiple catheters and cannulae, and treatment with broad-spectrum antibiotics. A dramatic decrease in such infections has occurred throughout the UK and elsewhere in the world.16
Ventilators have improved considerably over the past 10 years. Previously, a patient needed to generate a pressure drop within the ventilator circuit to trigger a breath from the ventilator. In more modern ventilators, inspiration is typically triggered by a subtle change in flow,17 which is more sensitive and makes ventilatory support more comfortable for a patient. As a result, ICU patients tend to need less sedation than in the past.18 Peri- and postcardiac arrest care has undergone major changes since 2000, and it is now common to cool out-of-hospital cardiac arrest survivors at 32–34°C for 24 h.19
There has been an increase in large, multicentre intensive care trials that are not industry funded, which undoubtedly has contributed towards an ever-increasing drive to raise standards of care. Survival for intensive care patients in the UK has been improving year on year, with ICNARC twice recalibrating its risk prediction model because of increasing survival rates (personal communication, ICNARC data on file). This improvement is despite a trend to admit patients with more comorbidities to intensive care, as patient, family and even medical expectations rise. Ethical issues are common in ICU because patients are often unconscious and, therefore, legally incompetent, and because decisions made by intensive care doctors have immediate consequences.4
Finally, possibly the most important change in the UK has been the establishment of intensive care as a stand-alone specialty, with the birth of the Faculty of Intensive Care Medicine (FICM) in 2010. A stand-alone training programme started in August 2012, and this should make intensive care training more accessible to trainees from respiratory medicine, renal medicine, cardiology and emergency medicine, as well as from the more traditional route of entry via anaesthesia.
Possible changes in intensive care over the next 10 years
A major change that is already affecting intensive care medicine is the ageing population, with demand for intensive care rising alongside increasing expectations from patients, their families and doctors from other specialties, and an increase in the illnesses that are deemed treatable. Combined with a steady rise in obesity and other comorbidities, it is likely that the demand for ICU care will rise exponentially.
However, the current economic climate affects intensive care just as it does the rest of the health service. The current numbers of critical care (ICU plus HDU) beds in the UK is among the lowest in Europe at 6.6 beds per 100,000 population, compared with 29.2 beds per 100,000 population in Germany.20 Given that countries with a greater number of ICU beds have lower levels of ICU mortality than those with fewer beds,21,22 there is pressure on the UK Department of Health to increase critical care capacity.
The increase in the number of HDU beds is likely to continue, because the ethos of admitting sick patients who are at high risk of deteriorating before they become critically ill becomes more widespread. This is a strategy that is associated with lower mortality, fewer complications, reductions in mortality and probably a reduced length of stay in hospital and reduced cost.23,24 High-risk surgical patients admitted to critical care areas for their postoperative care have mortality rates five times lower than those returned directly to a ward.25 Elective cardiac surgical patients are all cared for in ICU postoperatively and have mortality rates of <2%.25 By contrast, emergency surgical patients, often with predicted mortality rates of >50%, are being cared for on general surgical wards immediately after their operation. In the UK, a major expansion in HDU beds is required to accommodate all patients with a ≥10% predicted mortality to be admitted to critical care.24
A future expansion of outreach services would enable early identification of patients in need of critical care support and would provide follow-up care for those recently discharged from critical care.
The use of electronic monitoring systems within intensive care is set to rise, with many units now using patient data management systems with computerised patient notes and prescription systems for all patients. This enables data to be easily accessible for audit, research, and quality improvement, and for the development of more sophisticated and accurate risk prediction models. The latter could ultimately enable admission to intensive care to be restricted to those who are likely to benefit most from this expensive, invasive treatment.
It is likely that more subgrouping of major disease groups, such as sepsis and acute respiratory distress syndrome, will occur, with more individual tailoring of therapies. Such subgrouping might well involve genomics26 and/or bedside testing, with treatment planned accordingly. Antibiotic resistance and the development of multidrug-resistant organisms will be increasingly important. Continuing emphasis is likely to be placed on holistic aspects of intensive care, with daily planning boards, patient diaries, better family communication, early mobilisation and early rehabilitation.27
Increasing regionalisation of ICUs seems likely over the next 10 years in an attempt to concentrate expertise in fewer, larger centres around the UK.28 Such regionalisation already exists for paediatric intensive care and for major trauma.
Finally, given the current economic climate, it is likely that there will be continuing emphasis on quality improvement and the ethos of doing the simple things well, rather than on expensive new drugs and interventions.
Conclusion
Intensive care has undergone enormous change since the establishment of the specialty 60 years ago, and further changes will undoubtedly be seen in coming years.
Acknowledgements
We thank the Dr Geoffrey Spencer for permission to reproduce the photographs included in this article, and to ICNARC for permission to reference their data.
- © 2014 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}