
ABSTRACT
Symptomatic cardiovascular disease is one of the leading causes of hospital admissions in the UK; along with emergency attendances, over 100,000 patients are investigated using treadmill testing via rapid access chest pain clinics each year. With the introduction of new technologies, clinicians have a wide choice of investigations including nuclear perfusion scanning, dobutamine stress echocardiography, cardiac computed tomography and stress cardiac magnetic resonance imaging. These imaging modalities have their strengths and weaknesses, which depend not only on the pre-test likelihood of significant coronary artery disease but also the clinical characteristics of the patient. This article will review the differing imaging modalities, the patient experience, accuracy, prognostic data and future prospects for cardiac computed tomography and magnetic resonance imaging.
Introduction
Cardiovascular disease represents a significant health burden to the UK. Each year there are nearly 500,000 admissions (statistics from British Heart Foundation) for coronary artery disease. Of patients attending an accident and emergency department, 6% will have a presenting complaint of chest pain and over one-quarter of acute hospital admissions are for chest pain.1,2 This represents a significant health burden because the average length of stay for these patients is 2–3 days.3 It is estimated that there are over 1.1 million people living with angina in the UK.2
The National Service Framework for coronary artery disease recommends rapid access chest pain clinics (RACPCs) for the prompt (<2 weeks) assessment of patients with chest pain. Before 2010 this assessment took the form of a clinical history by a member of the cardiology team, followed by an exercise tolerance test (ETT) and/or further investigation in the form of myocardial perfusion scanning or invasive coronary angiography. It is estimated that >107,000 ETTs are performed in RACPCs each year; with the introduction of the 2010 National Institute for Health and Care Excellence (NICE 95) guidelines for the investigation of patients with chest pain of recent onset (Tables 1 and 2), these patients should be diverted to more appropriate and accurate investigations.4 Those with a low-to-intermediate pre-test likelihood of coronary artery disease are investigated with computed tomography coronary angiography (CTCA), patients with an intermediate pre-test likelihood of disease will have a functional imaging test to identify ischaemia (stress magnetic resonance imaging [MRI], echocardiography or nuclear medicine scanning) and those with a high risk of disease proceed directly to invasive coronary angiography.
An estimation of the pre-test likelihood of coronary artery disease. Reproduced with permission from Skinner et al (2010).4
An estimation of the proportion of patients allocated to different investigation pathways. Reproduced with permission from Skinner et al (2010).4
It is estimated that approximately 15% of patients attending a RACPC will fall into the category recommended for investigation with computed tomography (CT), 17% will need a functional test and 15% will proceed directly to invasive coronary angiography (Tables 1 and 2).
Computed tomography coronary angiography
It is now possible to visualise the coronary arteries using cardiac CT. This is an outpatient procedure only requiring intravenous cannulation (rather than a femoral or radial arterial puncture); it takes <30 min and has accuracy greater than any other non-invasive diagnostic test. Its main strength lies in the negative predictive value of 99%.5
Patient experience
The patient needs an intravenous cannula, electrocardiogram (ECG) monitoring during the scan for cardiac gating, β blockade (either intravenously or orally) and iodinated contrast media. There are few contraindications to scanning. To reduce cardiac motion artefact, the images are acquired during mid-diastole (70% of the R–R interval); therefore, for most CT scanners, a heart rate of 60–65 beats/min is required to enable the use of low radiation dose protocols. This is facilitated by the use of intravenous β-blockers. Scanning is possible in patients with a contraindication to β-blockers or those with arrhythmia (atrial fibrillation); however, this comes with a radiation dose penalty that should be taken into consideration by the referring clinician.
Coronary artery calcium scoring
Atheromatous deposits within the coronary arteries become calcified over time; the coronary artery calcium (CAC) scoring was originally developed using electron beam CT, but is now performed on multi-slice CT scanners. In a single breath-hold a scan is taken of the heart – no contrast is used. Specialist software is then used to identify CAC and the volume is expressed as an Agatston score.
An Agatston score of 0 is associated with a 10-year survival rate of 99.4% (in asymptomatic patients) and a score of >1,000 indicates a worse prognosis with a mortality rate of 12.2% over 10 years.6
The 2010 NICE guidelines, Chest pain of recent onset, suggest that in those with a coronary artery calcification score of 0, no further investigation is required.4–7 Since the publication of the guidelines a large, international, multicentre, observational registry reported that a calcium score of 0 did not rule out significant coronary artery disease (CAD) which, if present, was associated with increased cardiovascular events.8 Therefore it is likely that patients referred for cardiac CT will have both a calcium score scan and a full CTCA.
Significant calcification of the coronary arteries can reduce the accuracy of CTCA due to a ‘blooming’ artefact, leading to an overestimation of the severity of coronary stenosis and a subsequent reduction in specificity.9,10 This potential weakness can be overcome with the newer scanners.11
Accuracy
The main strength of CTCA is its high negative predictive value (Table 3); this is the proportion of patients with a negative test who are properly diagnosed. Therefore CTCA is recommended as a ‘rule-out’ test in patients with a low-to-intermediate pre-test likelihood of CAD.
Summary of studies investigating the accuracy of CTCA.
CTCA also plays a significant role in the assessment of patients with a history of revascularisation. The sensitivity and specificity for the detection of coronary artery bypass disease are high.14 Coronary artery stents can cause blooming artefact and reduce diagnostic accuracy due to their high density; however, the accuracy remain good in stents with a diameter of >2.5 mm15 (sensitivity for in-stent restenosis 90%, and specificity 95%). With the use of new generation scanners this is likely to improve.16
Acute admissions
Patients presenting to hospital with chest pain can be risk stratified clinically – with a history, ECG and biomarkers – and then either discharged or referred for appropriate investigations. CTCA has been shown to safely reduce the length of stay of patients with a low–intermediate risk of CAD who present to the accident and emergency department with chest pain.17
Radiation dose
One criticism of CTCA is the perceived high radiation dose from the investigation. This is of particular importance when bearing in mind the cohort of patients most likely to be referred, if following the 2010 NICE guidelines, namely young to middle-aged women. This group is least likely to benefit prognostically or symptomatically from further therapeutic intervention (because the scan is likely to be normal). The radiation dose from cardiac CT using low-dose protocols is equivalent to 1–2 years of background radiation and is estimated at 3–5 mSv per scan, significantly less than invasive coronary angiography.18 A typical chest radiograph has a dose of 0.02 mSv and a CT pulmonary angiogram 10 mSv.19,20
Prognosis
A CTCA scan negative for any coronary atheroma gives an extremely good prognosis (annual all-cause mortality rate of 0.6%) whereas those with high-risk obstructive disease have an annual event rate of 2.7%.21 Patients with non-obstructive atheroma have an annual event rate of 1.1%; this incremental prognostic insight is of importance, with new evidence suggesting that those with even a low clinical risk of major adverse cardiac events may benefit from statin therapy.22,23
Future prospects
The ability of CTCA to image not only the coronary lumen but also the wall makes it an ideal tool for longitudinal assessment of the coronary arteries in clinical trials aiming to demonstrate a reduction in atheroma burden.24 The new generation scanners featured in the 2012 NICE technology guidelines have the potential for improved temporal resolution and image quality.11 Scanners using an oscillating focal spot to acquire the images have a reduction in artefact from material with a high signal such as calcified atheroma or coronary stents16 and show an improved diagnostic accuracy in patients with a high CAC burden. CTCA offers an anatomical assessment of the coronary arteries, but does not give a functional assessment of myocardial perfusion as a consequence of any stenosis. This shortfall may be overcome with two techniques: first mathematical modelling of the coronary artery, which is comparable to invasive fractional flow reserve,25 and second cardiac CT perfusion imaging to delineate perfusion defects.26 These techniques could result in cardiac CT that offers anatomical and functional information about the coronary arteries; however, they are both experimental and need further evaluation before integration into clinical practice.
Cardiac magnetic resonance imaging
Cardiac magnetic resonance imaging (CMR) offers high temporal and spatial resolution imaging of the heart with no limitations on image quality due to patient body habitus. A comprehensive CMR examination delivers a gold standard assessment of left ventricular volume and function,27 along with an accurate assessment of myocardial ischaemia28 and infarction size.29
Indications
The 2010 NICE guidelines recommend functional testing as the first-line investigation for patients with an intermediate pre-test likelihood of CAD. Stress CMR is recommended along with stress echocardiography and single photon electron computed tomography (SPECT). However, CMR has no image orientation constraints, is not affected by patient size and does not expose the patient to ionising radiation.
Patient experience
A stress CMR protocol (including left ventricular function and scar assessment) lasts 45 min. Contraindications to scanning include the generic obstacles to MRI (such as a permanent pacemaker, cerebral and peripheral vascular devices), moderate-to-severe asthma and high-degree atrioventricular (AV) block when using adenosine as the vasodilator stress agent. During the examination, maximum coronary hyperaemia is achieved with an infusion of adenosine. First-pass perfusion imaging for ischaemia and late gadolinium enhancement are achieved with gadolinium contrast agents; the risk of allergy is small, but there is a small risk of nephrogenic systemic fibrosis (NSF) in patients with significant renal impairment (glomerular filtration rate <30 ml/min). NSF is a very rare disease characterised by induration and thickening of the skin, and is associated with progressive, irreversible, internal organ fibrosis, which is invariably fatal; it has not been definitively reported with the newer cyclic gadolinium agents in patients with normal renal function30 and in some case series there is a low incidence in patients with chronic kidney disease.31
The patient requires two intravenous cannulae along with haemodynamic and ECG monitoring. ECG gated images are acquired during a breath-hold of up to 15 seconds and this is repeated throughout the period of the examination. During the adenosine infusion most patients will experience some transient minor symptoms of flushing, dyspnoea and chest pain; however, these are very well tolerated and rarely lead to early termination of the examination. At the end of the adenosine infusion a bolus of gadolinium is infused followed by a saline flush.
Left ventricular function
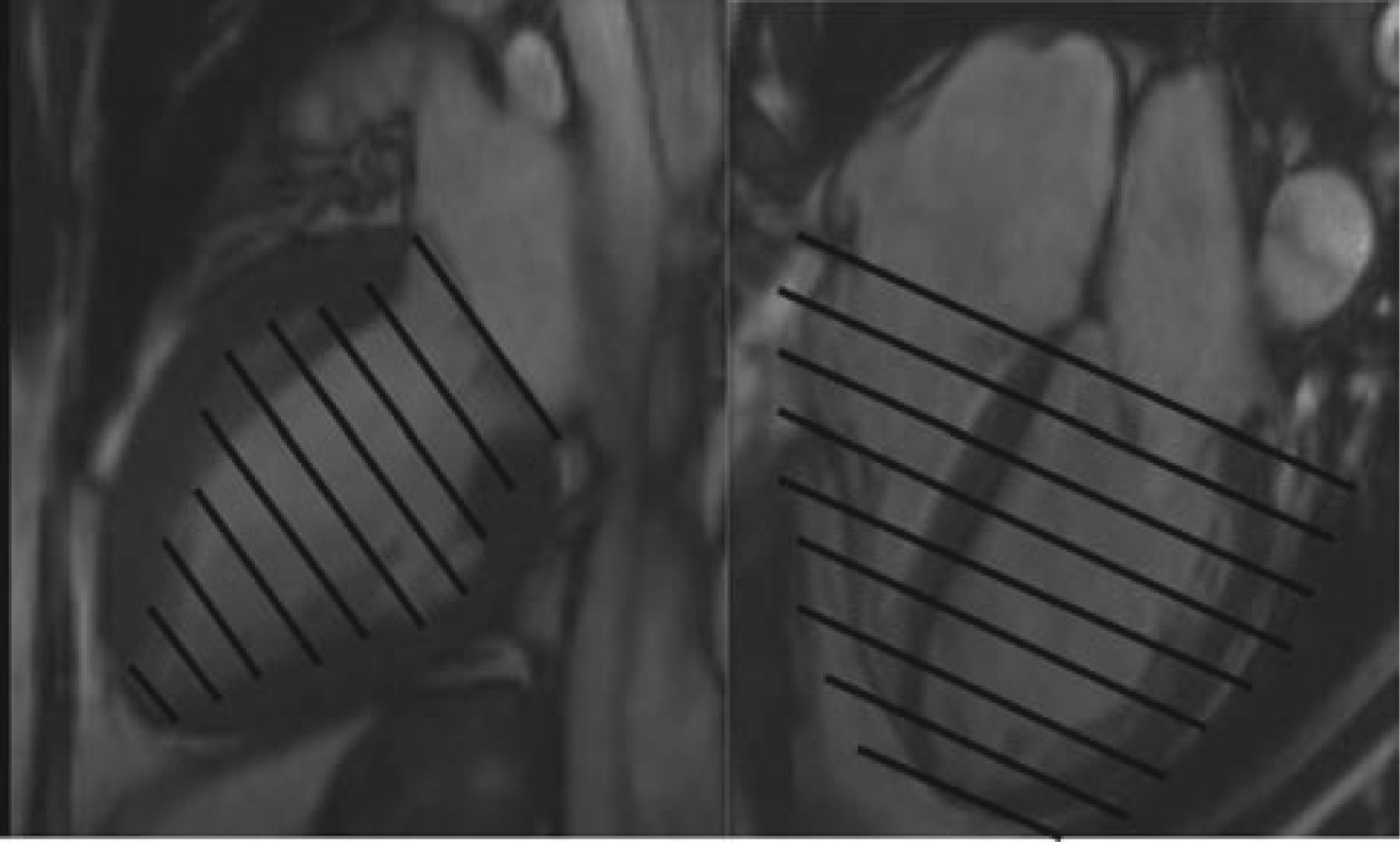
Left ventricular (LV) systolic function is the most important prognostic marker in cardiac disease. CMR offers the gold standard in terms of accuracy and reproducibility compared with other imaging modalities.27 To assess the LV volumes, mass and function, a stack of cine/moving images is taken in the short axis of the ventricle (Figs 1 and 2).

Left vertical long axis view (two chamber) and right horizontal long axis view (four chamber), with black lines demonstrating the imaging planes for a stack of short axis images for a normal left ventricle (see Fig 2). This produces a set of cine images from which the diastolic and systolic areas are calculated using semi-automated software.

Short axis images of the left ventricle in diastole (a) and systole (b), with the area of each slice drawn in black.
The method used in these figures does not calculate the ejection fraction based on assumptions of the shape of the left ventricle and uniform contraction and therefore does not overestimate the LV systolic function in the presence of regional wall motion abnormalities; this makes it particularly useful in the assessment of patients with known ischaemic heart disease.
Stress
After the infusion of adenosine to produce a hyperaemic response, a first-pass perfusion sequence is performed to track a bolus of gadolinium-based contrast agent through the myocardium. Stress and rest images are compared to identify areas of hypoperfusion indicating ischemia.
A recent meta-analysis of stress perfusion MRI demonstrates a sensitivity of 91% and specificity of 80% for the diagnosis of obstructive CAD; the specificity was significantly higher than using SPECT and the overall diagnostic accuracy better than perfusion stress echocardiography.28 The prognosis for a normal scan is good, with a 3-year event rate of 2.3% compared with 16.3% in those with a perfusion defect (Fig 3).32
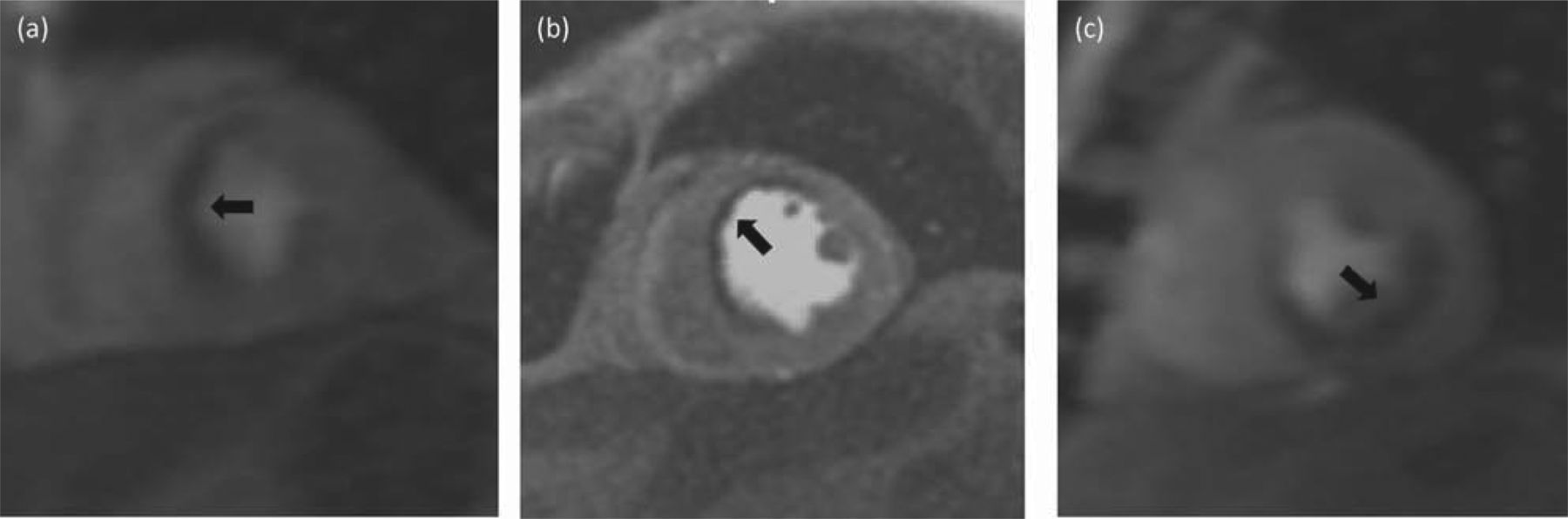
Perfusion defect (dark arrowed areas) in the (a) septal, (b) anterior and anteroseptal, and (c) inferior and inferolateral territories.
For futher investigation into the accuracy of stress cardiac MRI a recent study carried out a head-to-head comparision with SPECT. The study demonstrated the superiority of stress cardiac MRI over SPECT in terms of diagnostic accuracy and cost-effectiveness.33,34
Late gadolinium enhancement
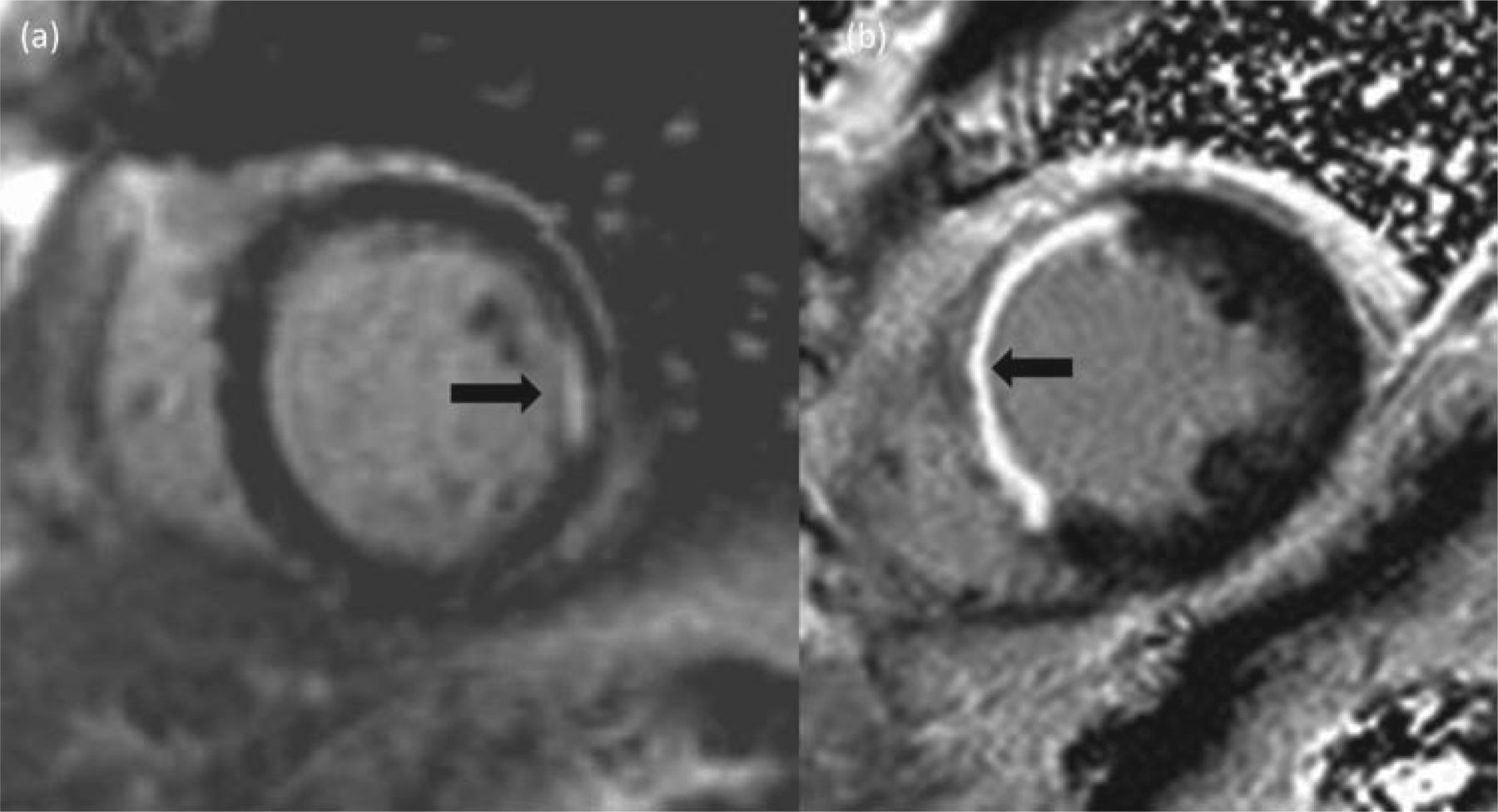
Gadolinium is an extracellular paramagnetic contrast agent that diffuses rapidly though the capillary basement membrane into the interstitial space. It does not cross intact cell membranes. The normal myocardium has very little extracellular space, although after a myocardial infarction the normal structure of the heart is replaced by collagen-rich scarring, in which the gadolinium accumulates. 10 minutes after a bolus of gadolinium, a series of T1-weighted inversion recovery scans are performed. As there is more gadolinium present in the scar tissue compared with normal myocardium, the area of scar can be identified. Due to the high spatial resolution of cardiac MRI, small subendocardial infarcts are visible, which are missed by other techniques.35 The extent of the myocardial scar can predict the chance of functional recovery after revascularisation in akinetic segments. Akinetic segments of myocardium with <50% transmural gadolinium enhancement have an improved chance of functional recovery compared to those with >50% transmural enhancement (Fig 4).29
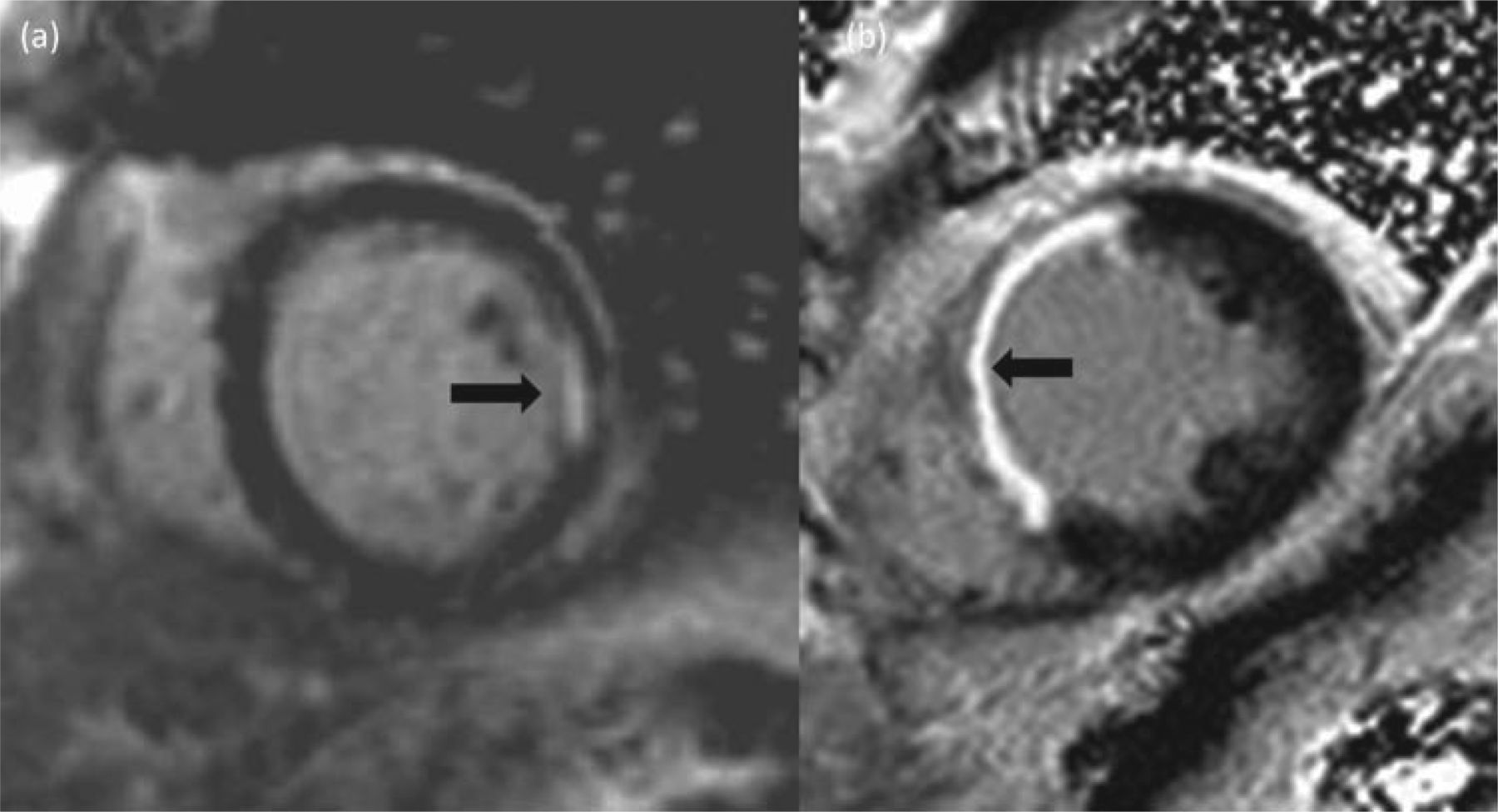
A small lateral subendocardial infarct (a) has a greater chance of -functional recovery when compared with a full-thickness transmural septal infarct (b).
Future prospects
With the advent of stronger magnetic field strengths (3-tesla scanners) whole heart perfusion imaging will be possible. This will enable complete coverage of the myocardium and may improve the diagnostic accuracy of stress CMR.36 Stress CMR assessment at present is a qualitative visual assessment of myocardial blood flow. Quantitative assessment is possible but is a timely and complex calculation; contemporary software and new scanning techniques may increase the applicability of quantitative measurements, leading to its adoption in clinical practice.
Although most patients can receive gadolinium contrast agents, it is generally not routinely used in those with a glomerular filtration rate of <30 ml/min or in those who undergo dialysis. Newer techniques using T1 mapping sequences can offer tissue characterisation without the need for contrast agents.37
Dobutamine stress echocardiography
Dobutamine stress echocardiography (DSE) has been in mainstream clinical use for more than 15 years. It offers an affordable, quick and accessible test for the assessment of myocardial ischaemia. Patients are scanned in the left decubitus position and the protocol typically lasts <15 min. Incremental doses of dobutamine are infused to reach an age- and sex-defined target heart rate, similar to exercise ECG stress testing. Atropine boluses are sometimes needed to augment the heart rate. Baseline images are compared with those taken at a low-dose (10 μg/kg per min) intermediate level (70% of maximum heart rate) and peak stress (85% of age-predicted maximum heart rate).
The sensitivity, specificity and accuracy of the test in a meta-analysis are 80%, 84% and 80%, respectively. Sensitivity increases to 92% in the presence of three-vessel disease, compared with 74% in single-vessel disease.38
The rationale for the diagnosis of myocardial ischaemia is a relative reduction in myocardial blood flow sufficient to cause a detectable decrease in myocardial contraction (an inducible wall motion abnormality). The diagnostic accuracy of the test therefore hinges on the clarity of the images produced. Images are improved by the simultaneous infusion of transpulmonary ultrasound contrast such as Sonovue; this can enable scanning of patients with poor echocardiographic windows.39
The sensitivity is reduced in the circumflex artery (55%) due to difficulty in imaging the myocardium of the lateral wall (this is typically obscured by ultrasound dropout). The dependency of the examination on clearly defining the myocardium makes it unsuitable for patients with poor echocardiography windows – typically seen in obese patients or those with significant respiratory disease. Therefore the examination is not suitable for all.
A scan negative for inducible wall motion abnormalities and showing a reduction in LV volumes at peak stress heralds a good prognosis: fewer than one cardiac death per annum.40
In patients with pre-existing coronary disease, DSE can be used to assess for viable myocardium. An akinetic area of myocardium that is viable and ischaemic will demonstrate a biphasic response to dobutamine. At low-to-intermediate dose the myocardium contractility improves, followed by a depression in movement at peak stress.41
Myocardial perfusion scintigraphy
An alternative functional imaging modality to CMR and DSE is myocardial perfusion scintigraphy or SPECT. During stress with a vasodilator, such as adenosine or dipyridamole, a radioisotope is injected intravenously. During stress, myocardial blood flow typically increases by three- to fivefold; in the presence of a coronary stenosis there will be reduced uptake of the isotope in the myocardial territory subtended by the diseased vessel.
SPECT is readily available in many hospitals, and has a large historic evidence base in terms of diagnostic accuracy and prognostic information. The sensitivity of SPECT in a meta-analysis is 88% and specificity 61% (compared with 89% and 76% respectively for CMR).42 The prognosis for a negative scan is good, with a 1-year cardiac event rate in this cohort of <1.43
Compared with CMR and DSE, SPECT has several limitations: it exposes the patient to the stochastic effects of ionising radiation, there is image attenuation from breast tissue, the diaphragm can significantly affect the diagnostic accuracy, and prognostically important disease can be overlooked due to the ‘balanced ischaemia’ effect seen in left main stem disease or three-vessel disease.44
Cost implications of the NICE 2010 guidelines
The guidelines suggest that ETT should no longer be used for the assessment of patients with suspected coronary disease. Instead a diagnostic pathway based on the patient's pre-test likelihood of coronary disease is recommended. Implementation of these guidelines will have an impact on local health economies. The estimated cost of CT coronary angiography, stress CMR, DSE and SPECT are significantly more than an ETT (£173, £313, £236, £293 and £75 respectively). However, there is no significant difference between the costs of the functional imaging modalities recommended based on the NICE tariff, compared with £1,052 for an invasive angiogram.45
Conclusion
As ischaemic heart disease is one of the most common conditions presenting to secondary care, improved diagnostic tests that are accurate and reduce the downstream investigations and cost are imperative for a sustainable healthcare system. An integrated diagnostic pathway directing the right patient to the right investigation using DSE, CT and MRI will help to achieve these goals. Cardiac CT is of particular use in low- to intermediate-risk patients to rule out CAD. Cardiac MRI can accurately assess ischaemia in patients with an index presentation of chest pain, but can also provide additional information about LV function, regional wall motion abnormalities, scar burden and viability in patients with established ischaemic heart disease.
Acknowledgements
Dr Gosling would like to acknowledge the support of the Gawthorn Trust Royal Devon and Exeter Foundation NHS Trust.
Competing interests
Dr Morgan-Hughes has received lecture fees from GE healthcare and Dr Gosling has received lecture fees from Pfizer.
- © 2014 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}
{kind=link}