
Background
Diarrhoea forms part of the symptom burden of many patients with cancer and can manifest from a low-grade but persistent annoyance to a life-threatening toxicity requiring inpatient admission and urgent medical care. Acute and chronic forms of diarrhoea are differentiated by their duration (acute diarrhoea lasting for up to 4 weeks).1 Acute diarrhoea is a common adverse effect of systemic anticancer therapy (SACT) affecting up to 80% of patients treated with some chemotherapy regimens.2 Diarrhoea grading is described in Table 1; however, the patient's perception of the burden of their toxicity might differ from the classical medical description of its severity.3
Common terminology criteria for adverse events (v4.0).
Acute diarrhoea in patients receiving treatment for cancer can arise as a direct consequence of damage to the bowel from chemotherapy or radiotherapy or indirectly (eg from secondary infection or the effects of previous surgery). Distinguishing between these differing aetiologies for diarrhoea in patients receiving cancer treatment is important for determining appropriate management. Previous surgery to the gastrointestinal tract can result in altered gastric emptying or bile salt flow, bacterial overgrowth or hepatic and/or pancreatic insufficiency; all can result in diarrhoea that can be exacerbated by systemic anticancer treatment. Overflow diarrhoea associated with bowel stasis and incomplete obstruction can result directly from the effects of the cancer itself or as a consequence of medications (eg opiates), abdominal surgery or radiotherapy (eg pelvic radiotherapy having effects on loops of small bowel or the sigmoid colon).4–6
Assessment and management
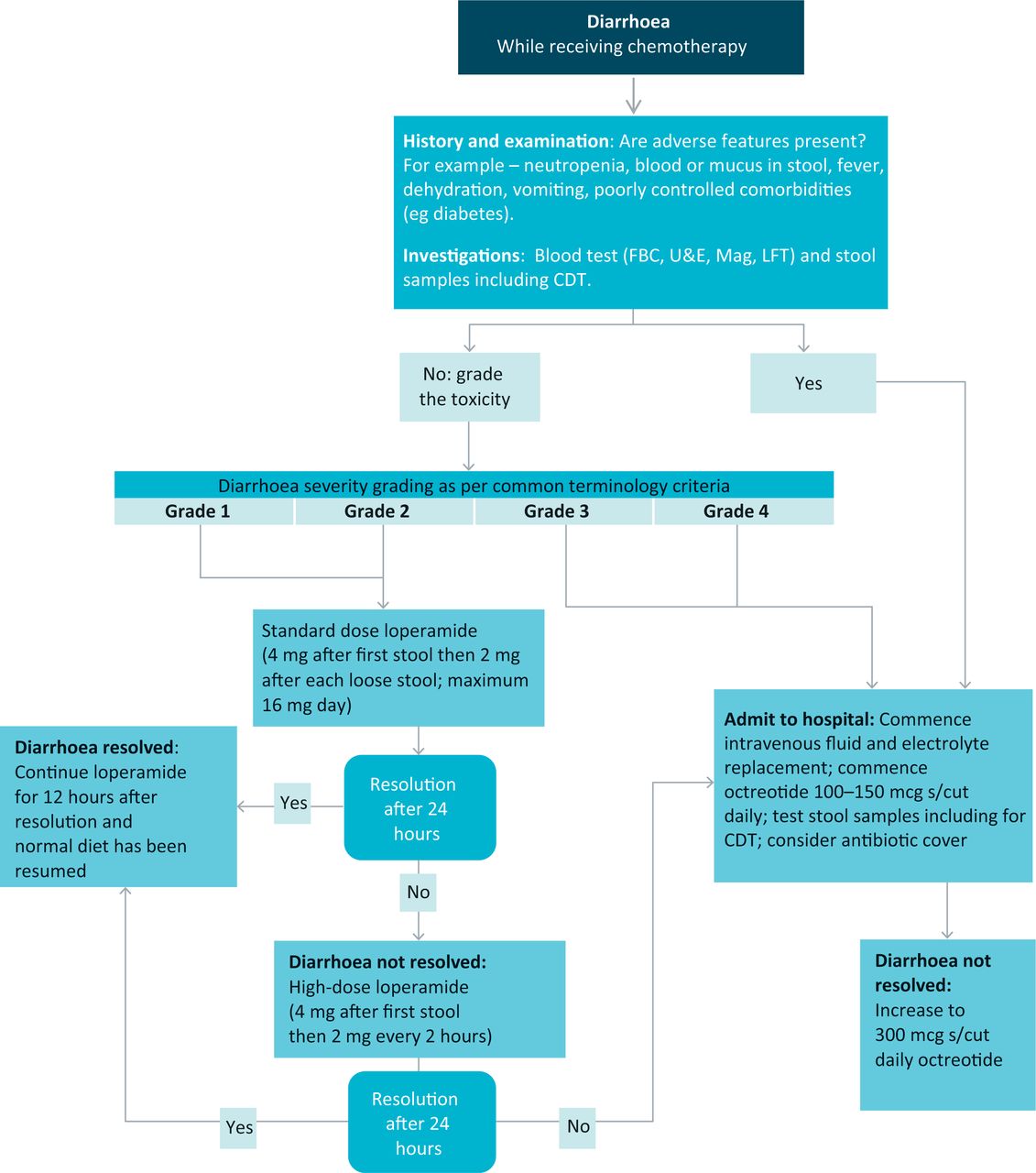
The management of diarrhoea in patients with cancer receiving SACT can be markedly different compared with patients on a general medical ward, because antidiarrhoeals might need to be used early and aggressively, before stool culture results are available. Fig 1 outlines a common assessment and treatment pathway for patients on chemotherapy with diarrhoea. The most important distinction to make when assessing a patient is whether the diarrhoea is secondary to either infection or to treatment. Guides to an infective cause for assessing acute diarrhoea are symptoms such as fever, contact with a person with diarrhoea, exposure to possible infective sources (eg eating out) or recent travel abroad.7
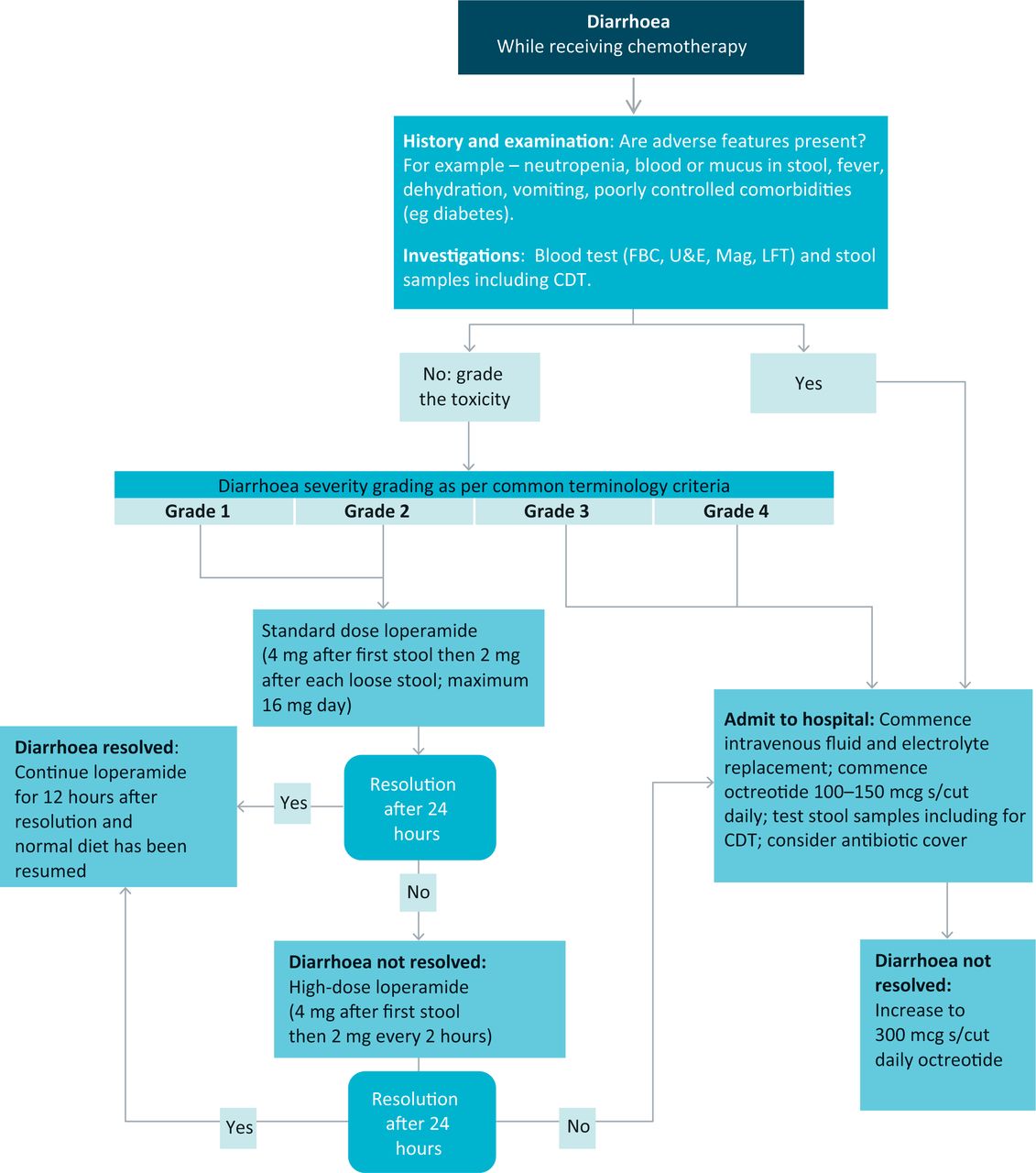
Flow diagram for the management of patients with diarrhoea while receiving chemotherapy. Common terminology criteria grading is given in Table 1. CDT = Clostridium difficile toxin; FBC = full blood count; Mag = magnesium; LFTs = liver function tests; U&E = urea and electrolytes.
Gut infection
Cytotoxic chemotherapy agents directly affect the gastrointestinal mucosa and cause inflammation, oedema, ulceration and atrophy, leading to increased permeability of the bowel mucosa and increased susceptibility to the spread of organisms from the intestine across the bowel wall into the blood stream. This can result in septicaemia and shock, especially if it coincides with chemotherapy-induced neutropenia.4,8,9 The gastrointestinal symptoms caused through infection can respond quickly to antibiotics. The work up of such patients should be timely because appropriate early intervention can decrease morbidity and mortality.
Although coliforms, such as Escherichia coli, are the most common pathogens causing sepsis in patients with chemotherapy-induced diarrhoea (CID), other organisms, such as Clostridium difficile, fungal infections and viruses, can be responsible for severe symptoms. Clostridium difficile might not be associated with previous antibiotic use in patients on chemotherapy and can present without typical features; for example, 10% of cases are toxin negative and, in neuropenic patients, the typical pseudomembranes seen on endoscopy might not be obvious. Treatment includes oral metronidazole or vancomycin, depending on local protocol and severity. In patients with severe or prolonged treatment-induced immunosuppression, infection with viral pathogens, such as cytomegalovirus (CMV), should be considered. Empirical treatment should be considered when there is a high index of suspicion because positive detection of CMV (by culture or polymerase chain reaction) can take several weeks.4
Acute diarrhoea secondary to anticancer treatment
Chemotherapy-induced diarrhoea (CID) can occur in up to 80% of patients, depending on the regimen. Combinations of agents can have additive or synergistic effects with greater frequency and severity of diarrhoea (Table 2). Agents involved in treating cancers of the gastrointestinal tract are those most commonly associated with severe diarrhoea.
Chemotherapy regimens and rates of severe diarrhoea.11
There are several specific factors that can influence the likelihood of CID with individual chemotherapy agents.
Oral anticancer treatments
With orally administered chemotherapy, patients are ultimately responsible for taking the medication. Some patients, in the hope of increasing treatment effectiveness, will continue to take their tablets despite the onset of severe and increasing toxicity. Good patient selection and education are vital and can reduce the morbidity associated with this treatment route.10
Fluorouracil and dihydropyrimidine dehydrogenase
Up to 5% of patients have genetic polymorphisms resulting in reduced activity of dihydropyrimidine dehydrogenase (DPD), an enzyme central to fluorouracil catabolism. Administration of a standard dose of 5 fluorouracil (5FU) in such patients results in significantly prolonged exposure to higher concentrations of the drug, resulting in early onset and increased severity of diarrhoea and other toxicities. Patients should be managed aggressively as above and further 5FU use would not be recommended.12
Irinotecan
Irinotecan is associated with two distinct forms of diarrhoea. Early-onset diarrhoea (within 24 h) is associated with an acute cholinergic reaction and often with rhinitis and salivation. This should be treated with atropine and usually resolves quickly. Late-onset diarrhoea is particularly difficult; it is associated with the production of irinotecan metabolites within the gastrointestinal tract and can produce profuse diarrhoea. It tends to occur around 7–10 days post treatment, corresponding with the most likely time for neutropenia. Ciprofloxacin is often given to patients if moderate diarrhoea develops at home, to cover for Gram-negative sepsis.9
Polymorphisms in the UGT1A1 gene (whose protein product is involved in irinotecan degradation) have been associated with an increased risk of severe diarrhoea with moderate or high doses of irinotecan.
Biological treatment
Diarrhoea is a common adverse effect of the newer targeted anticancer therapies and occurs in up to 60% of patients. Drug interactions (between different targeted therapies or in combination with classical cytotoxics) can increase the risk and severity of diarrhoea. Particularly important or common drugs are listed in Table 3.
Rates of diarrhoea in commonly used biological anticancer agents.
Ipilimumab, used in patients with malignant melanoma, acts differently compared with other commonly used biological therapies by affecting the immune response of the body to cancer cells through modulating T cell immunity. Ipilimumab-associated diarrhoea (up to 40% of treated patients) is an immune-related adverse effect. In approximately 7% of patients, the diarrhoea is Grade 3 or more and can occasionally be life threatening.13 Concern is raised if diarrhoea is associated with other gastrointestinal toxicities, such as nausea, vomiting or cramping abdominal pain, or the presence of blood in the diarrhoea. Low-grade persistent diarrhoea beyond 7 days is also a concern. These patients should be treated in close liaison with the oncology team to discuss possible endoscopy, corticosteroid or infliximab therapy.14
Chemoradiotherapy
Patients receiving concurrent chemotherapy and radiotherapy (chemoradiotherapy) can be more susceptible to diarrhoea, particular if receiving radiotherapy treatment to the pelvis.5 Peak incidence for acute diarrhoea is 1–2 weeks after radiotherapy, when the toxicity to the gastrointestinal mucosa is at its highest. This needs to be proactively treated to reduce the burden of toxicity in patients, as described by Wang-Gillam for the treatment of patients with pancreatic cancer with chemoradiotherapy.15
There is increasing recognition of the long-term gastrointestinal toxicity as a result of radiotherapy. Specialist services and support are available for those with long-term toxicity and its sequelae (eg malabsorption and rectal bleeding).
Neutropenia and typhlitis
Typhlitis is bowel inflammation usually involving the caecum in a patient with chemotherapy-induced neutropenia. It is associated with a triad of right lower quadrant pain, fever and bloody diarrhoea. As any part of the bowel can become involved with some chemotherapies, particularly with taxane use or drug combinations used in haematological malignancies, the term ‘neutropenic enterocolitis’ (NEC) has gained popularity.16
In either case, the patient should receive treatment similarly to any other neutropenic patient alongside aggressive antidiarrhoea management, including aggressive fluid resuscitation and broad-spectrum antibiotics, antifungals can also be indicated. NEC is associated with a gastrointestinal tract thickness of >4 mm on imaging.
There is a high mortality associated with this rare condition. Complications include bacteraemia, haemorrhage and bowel wall perforation or abscess formation. If the bleeding is severe, surgical intervention might be necessary if appropriate.16–18
Adjuvants to treatment
Supportive medications, such as antibiotics, antiemetics, laxatives and some herbal remedies, alongside systemic treatment can also lead to diarrhoea. These should be considered together with a general medical and medicines review.
Future developments in managing chemotherapy-induced diarrhoea
Identification of individual patients at greater risk of CID would enable treatment modifications in advance. It is known that gene polymorphisms for enzymes involved in the metabolism of cytotoxic chemotherapy agents can result in increased drug exposure causing greater likelihood and severity of CID. Assays to detect possible enzyme deficiency states are available (some commercially) or under development; for example, DPD assays for 5FU toxicity and UGT1A1 assays for irinotecan toxicity. However, evidence supporting the predictive benefits of such assays remains contradictory.
Prophylactic measures to reduce the incidence or severity of CID have been researched, with multiple trials trying to identify the optimum prophylactic measure for CID. Probiotics have produced mixed results in diarrhoea of all causes, but use in patients receiving chemotherapy needs further study. Long-acting octreotide has been used, without clinical trial, for patients with rectal cancer at high risk of CID and in those with severe diarrhoea but whom dose reduction is undesirable.2 Slow-release steroids (eg budesonide), which become active within the small and large intestine, are used in inflammatory bowel disease and have been trialled in CID.9
Conclusion
Diarrhoea is a common and important toxicity. Its management differs from that within other medical specialties and early and aggressive use of antidiarrhoeals is paramount. Good patient education and support, together with prompt medical treatment, can reduce both morbidity and mortality.
Key points
Diarrhoea is a common and important symptom in patients receiving chemotherapy
The aetiology of diarrhoea can relate to the cancer treatment (chemotherapy, radiotherapy or surgery) or be infective in nature
Antidiarrhoeals might be indicated much earlier than usual, especially if the diarrhoea is secondary to treatment rather than infection
Some patients might be more prone to toxicity, including diarrhoea, experiencing diarrhoea earlier and with greater severity than usually expected, for example in dihydropyrimidine dehydrogenase deficiency
New biological agents, such as ipilimumab, can result in diarrhoea through different mechanisms of action and require specialist oncology advice and management from early on
- © 2014 Royal College of Physicians
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.