
Background and scale
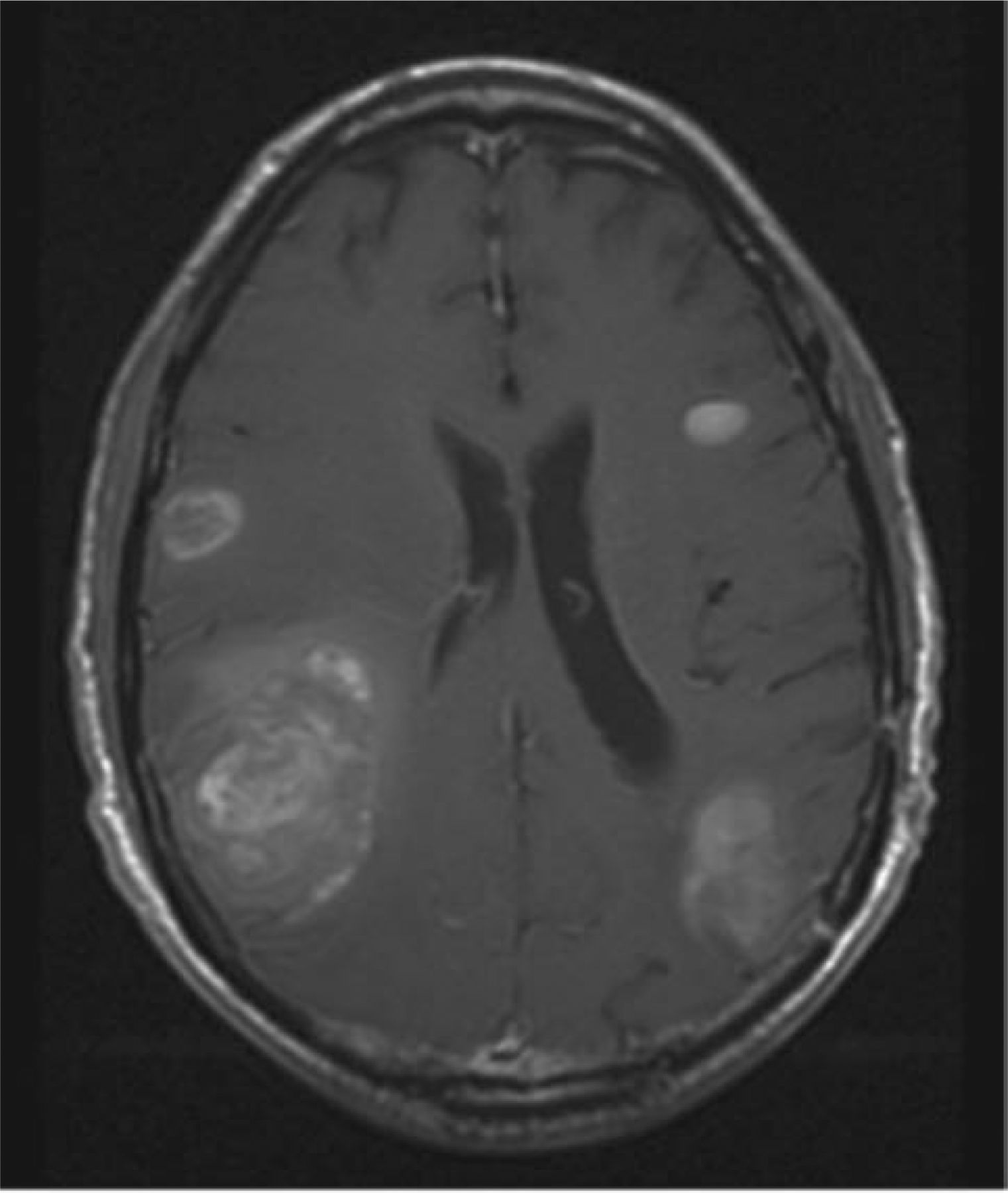
Brain metastases affect up to 40% of patients with cancer during their illness.1 The prognosis is often poor and lesions frequently result in significant morbidity despite treatment. Lung cancer (42%), breast cancer (19%), colorectal cancer (9%), melanoma (7%) and cancer of unknown primary (7%) cancer are the primary diagnoses most frequently associated with brain metastases.2 The incidence of brain metastases appears to be increasing, although much of this is likely to be the result of improvements in, and access to, imaging. Fig 1 shows magnetic resonance imagine (MRI) of the brain demonstrating multiple brain metastases.
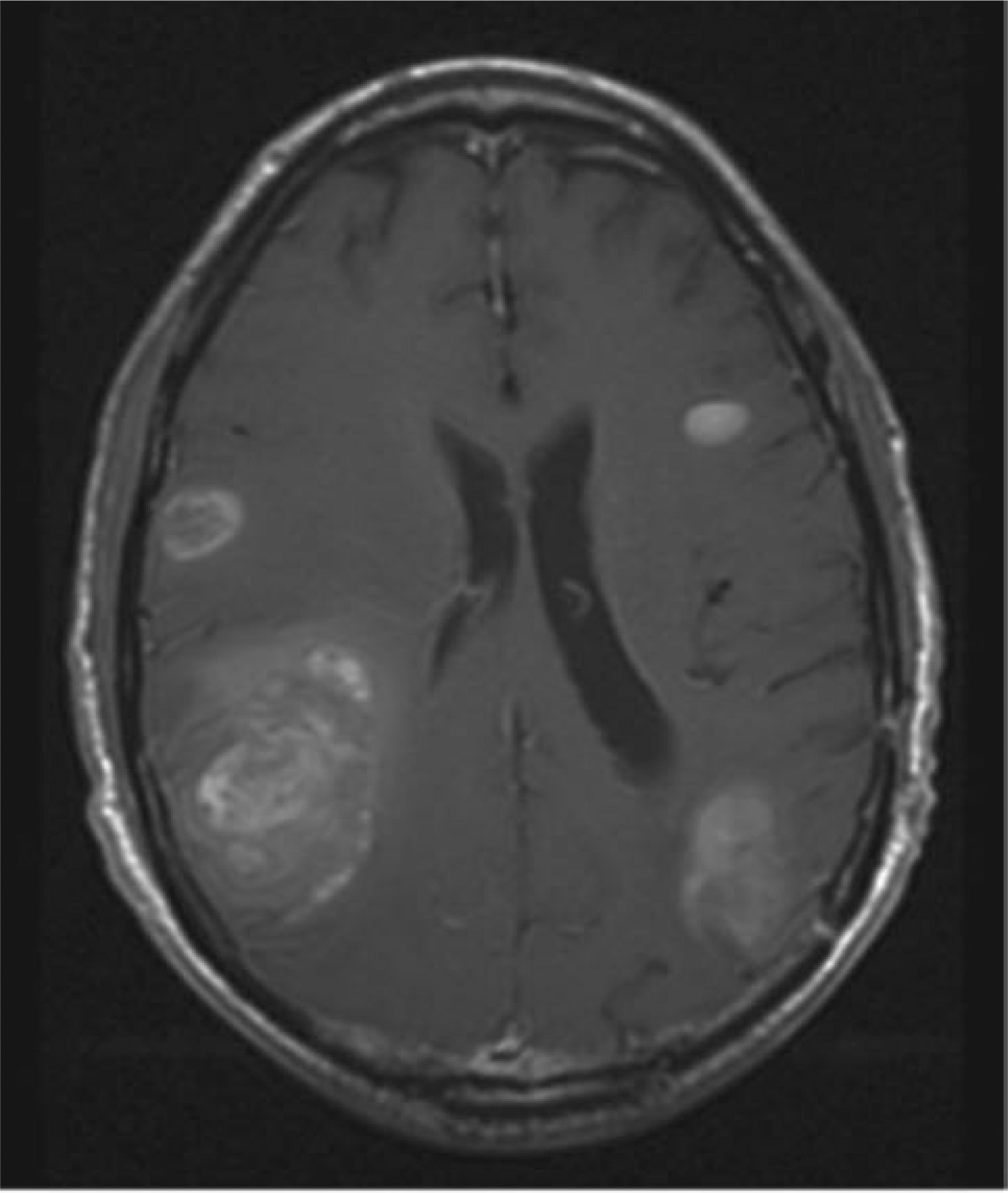
Magnetic resonance imaging, with gadolinium enhancement of the brain, demonstrating multiple enhancing brain metastases with surrounding vasogenic oedema and effacement of the ventricle.
Presentation
Presentation with brain metastases can be in the context of known extensive systemic disease or, less frequently, as a de novo presentation of metastases. Presenting symptoms tend to have a subacute onset over days to weeks, with the most frequently occurring symptoms at presentation being headache (49%), focal weakness (30%), gait ataxia (21%) and seizures (18%).1 Less-frequent presentations include nausea, speech disturbance, visual disturbance and sensory disturbance. As would be anticipated from the frequency of these presenting symptoms, most metastases are located within the cerebral hemispheres, the cerebellum less frequently (10–15%) and rarely the brain stem (1–3%).1
Prognosis
Without treatment, the prognosis following a diagnosis of brain metastases is poor, with a median survival of 1–2 months. Depending on the patients’ general health, radiotherapy may lead to improved survival (up to approximately 4 months) in selected cases.3–5 However, any treatment must be carefully tailored to avoid unnecessary treatment burden and toxicity during the last few weeks of life.
To try to identify those patients who are likely to benefit from a more aggressive approach, several prognostic indices have been developed. The most frequently used of these was developed using a pooled analysis of all patients with brain metastases who were randomised into three major North American radiotherapy trials.6 This study aimed to use recursive partitioning analysis to define the features predictive of outcome in patients with brain metastases. Performance status, extracranial and primary tumour disease status and age were identified as significant predictors (Table 1). This study also identified those patients with solitary brain metastases as having a better prognosis compared with those with multiple lesions. Patients with breast cancer also had a better prognosis compared with all other diagnostic groups combined.
Recursive partitioning analysis classification with characteristics and median survival.
Investigations
Given the significant variation in prognosis associated with the factors discussed above (see Table 1), there is a need to individually tailor investigations. Performance status (PS) of the patient is a key driver of investigations because the former also dictates management and outcome of the patient.7 Where doubt exists about the appropriateness of investigation, specialist advice should be sought to avoid the distress and discomfort of investigations that are unlikely to alter management. Where patients are felt to be well enough for intervention beyond steroids, extracranial disease must be assessed by computerised tomography (CT). In patients with known malignancy, this establishes the status of disease as either progressive or stable. In those with their first presentation of malignancy, investigations are those of a suspected malignancy of unknown origin.
The differential diagnosis of a solitary intracranial lesion includes benign lesions beyond the scope of this article (eg infection) and several malignant processes, including: solitary metastasis from an extracranial primary tumour; primary brain tumour; and primary central nervous system lymphoma. Imaging and clinical history may help to distinguish between these differentials with biopsy used to confirm the diagnosis when appropriate.
For lesions identified as solitary on contrast-enhanced CT, magnetic resonance imaging (MRI) with gadolinium is indicated to assess the extent of intracranial disease and resectability. Where there is a high degree of clinical suspicion in the presence of a normal CT, MRI might be indicated to assess for possible leptomeningeal disease.
The acute oncology team can facilitate multidisciplinary involvement of neurosurgeons, radiologists, oncologists and pathologists to ensure the prompt and appropriate diagnosis and management of patients with brain metastases.
Immediate management
High-dose dexamethasone reduces cerebral oedema, providing symptomatic relief and potentially improving function and quality of life. A typical regimen is dexamethasone 16 mg daily for 48 h (a single dose in the morning giving less risk of insomnia than divided dosing) followed by gradual reduction to a maintenance dose of 2–4 mg daily. Blood glucose levels should be monitored regularly while taking high-dose corticosteroids, and prophylactic gastric protection should be considered using proton pump inhibitors. Unnecessary continuation of high doses of corticosteroids has potentially debilitating neuromuscular, psychological, cosmetic, gastrointestinal and metabolic adverse effects.
Patients presenting with seizure activity should be given anticonvulsant therapy according to local policy and are likely to require long-term anticonvulsants. For those with complex symptom control problems, early involvement of specialist palliative care is beneficial.
Treatment options, aims and toxicity
Patients with a limited number of lesions (≤4) who are of recursive partitioning analysis (RPA) classification I or II (either before or after steroids) can be considered for more aggressive treatment in the form of either neurosurgery or stereotactic radiotherapy. Discussion with the local neurosurgical team, ideally in the context of an appropriate multidisciplinary team, enables appropriate decision making for this group. Other patients who might benefit from neurosurgical intervention are those for whom palliation through reduced intracranial pressure (ICP) might be achieved by surgery (eg those with hydrocephalus or large metastases [>5 cm] suitable for debulking). Posterior fossa lesions in particular might benefit from neurosurgical intervention. For those who have no confirmed diagnosis, and in whom no other more accessible lesion can be identified, neurosurgical biopsy might be sought if the patient is likely to be a candidate for further oncological treatment. Review by the treating oncologist or the local acute oncology team should be sought where there is doubt about the appropriateness of referral to neurosurgery.
The three main indications for surgery are: resection of a solitary or few (usually three or less) accessible metastasis; palliation of hydrocephalus and/or debulking of large metastasis; and biopsy for histological diagnosis.
Stereotactic radiosurgery
Stereotactic radiosurgery (SRS) delivers highly conformal, ablative doses of radiotherapy to intracranial lesions with millimetre accuracy, largely sparing the surrounding normal tissue. Strict criteria are necessary to ensure appropriate patient selection. Common selection criteria include four or fewer metastases ≤4 cm, in patients with controlled or only slowly progressing distal disease that do not require surgery for mass effect, cerebrospinal fluid pathway control or diagnosis.
The question of whether SRS is equivalent to surgery remains, with studies producing conflicting results, and no good randomised controlled trials. The data so far suggest that SRS is almost as good as surgery for tumour control, but with less risk. The choice of SRS over surgery is often based on surgical accessibility, size of the lesion, functional status of the patient and the local availability of SRS.8,9
Role of whole-brain radiotherapy
For patients with more than four lesions and RPA classification I or II, whole-brain radiotherapy (WBRT) can be considered. This has been the accepted standard treatment for palliation of brain metastases for the past 3 decades.10 However, the resulting toxicity is significant and no randomised evidence of either symptomatic or survival benefit exists in the CT era.1 Common toxicities of WBRT include fatigue, alopecia, scalp erythema and impaired higher cognitive function. Somnolence syndrome and severe headaches are less frequently seen adverse effects. As such, SRS and surgery are increasingly preferred for appropriate patient groups. The QUARTZ trial (a Medical Research Council-funded randomised trial) is evaluating WBRT versus steroids and best supportive care in the management of brain metastases in patients with non-small cell lung cancer.11 For those who are not suitable for further intervention, steroids are the mainstay of treatment alongside good-quality palliative care.
WBRT has been shown to reduce local and distal cerebral recurrence rates when delivered adjuvantly following either surgery or stereotactic radiotherapy. However, there is no demonstrable improvement in overall survival.12
Patients with tumours with high intrinsic chemosensitivity, for example lymphoma or germ cell tumours, should be treated primarily with chemotherapy. The role of systemic chemotherapy in other patients is assessed on an individual basis.
Relapse
Despite treatment, approximately 50% of patients with brain metastases will die of intracranial progression, with relapse often being rapidly fatal. For a few patients with oligometastases, resection or SRS might offer disease control and better prognosis. However, symptomatic treatment with corticosteroids is often the only intervention for patients who maintain good performance status despite relapse; systemic cytotoxic therapy and emerging biological targeted therapies remain an option in selected cases. Investigation and imaging of patients in the post-treatment period should be discussed with the treating oncology team, given the significant crossover between disease- and treatment-related symptomatology.
Conclusion
Brain metastases herald a poor prognosis for most patients with cancer. Given the systemic nature of metastatic disease, outcomes are often dependent upon not only local treatment, but also the patient's overall response to systemic therapy. Despite treatment, over half of all patients with brain metastases will die from intracranial progression.1 Although steroids remain the mainstay of treatment, additional treatment with surgery, SR or WBRT can be considered. A full assessment of the patient and their disease status enables a degree of prognostication and, hence, appropriate clinical decision making.
Key points
High-dose steroids are the mainstay of treatment (accompanied by gastric protection and monitoring of blood glucose levels)
Where doubt exists over the appropriateness of investigations and treatment, prompt discussion with the acute oncology team is recommended
Computed tomography (CT) imaging of the head to confirm the diagnosis and chest/abdomen/pelvis to assess extracranial disease is required
Treatment options include neurosurgery, stereotactic radiosurgery (SRS) and whole-brain radiotherapy (WBRT). Post-treatment imaging should be discussed with the treating oncology team
Prognosis is poor and early palliative care input should be considered
- © 2014 Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.