
ABSTRACT
Mycoplasma pneumoniae primarily causes respiratory tract infections. Extrapulmonary manifestations are seen in 20–25% of cases. Cardiac involvement is rarely reported. We present a unique case of a pericardial mass and cardiac tamponade associated with a Mycoplasma pneumoniae pneumonia. This required emergency pericardial fenestration. The patient improved dramatically postoperatively on antibiotics and there was no recurrence of the pericardial effusion on follow up. This case highlights the often forgotten invasive properties of a common respiratory tract pathogen and emphasises the need to consider this easily treatable entity in the differential diagnosis of idiopathic pericardial effusions.
Lesson
A 40-year-old African–Caribbean woman presented to the emergency department with a 4-day history of worsening shortness of breath and chest pain. These were preceded by a 3-week history of fevers, a non-productive cough, fatigue and generalised aches. Significant medical history included childhood asthma and a 10-pack-year smoking history. She was not prescribed any regular medication.
Initial clinical examination revealed a temperature of 38.5°C, a blood pressure of 107/85 mmHg, a heart rate of 110 beats/min and a respiratory rate of 20 breaths/min, with oxygen saturations of 95% on room air. Heart sounds were normal on auscultation and there was evidence of bronchial breathing on the right lung base with a few bibasal crepitations. Systemic examination did not reveal any other abnormalities. Electrocardiogram (ECG) showed sinus rhythm with a ventricular rate of 102. There was a fixed anterolateral T-wave inversion with good R-wave progression. The P–R interval was 146 ms with a QTc of 427 ms. The axis was normal with no evidence of fascicular block. The chest radiograph revealed an enlarged, globular, cardiac silhouette with right basal consolidation in the lung parenchyma. Laboratory blood tests during the course of her admission are summarised in Table 1. Mycoplasma serology was positive.
Laboratory blood tests.
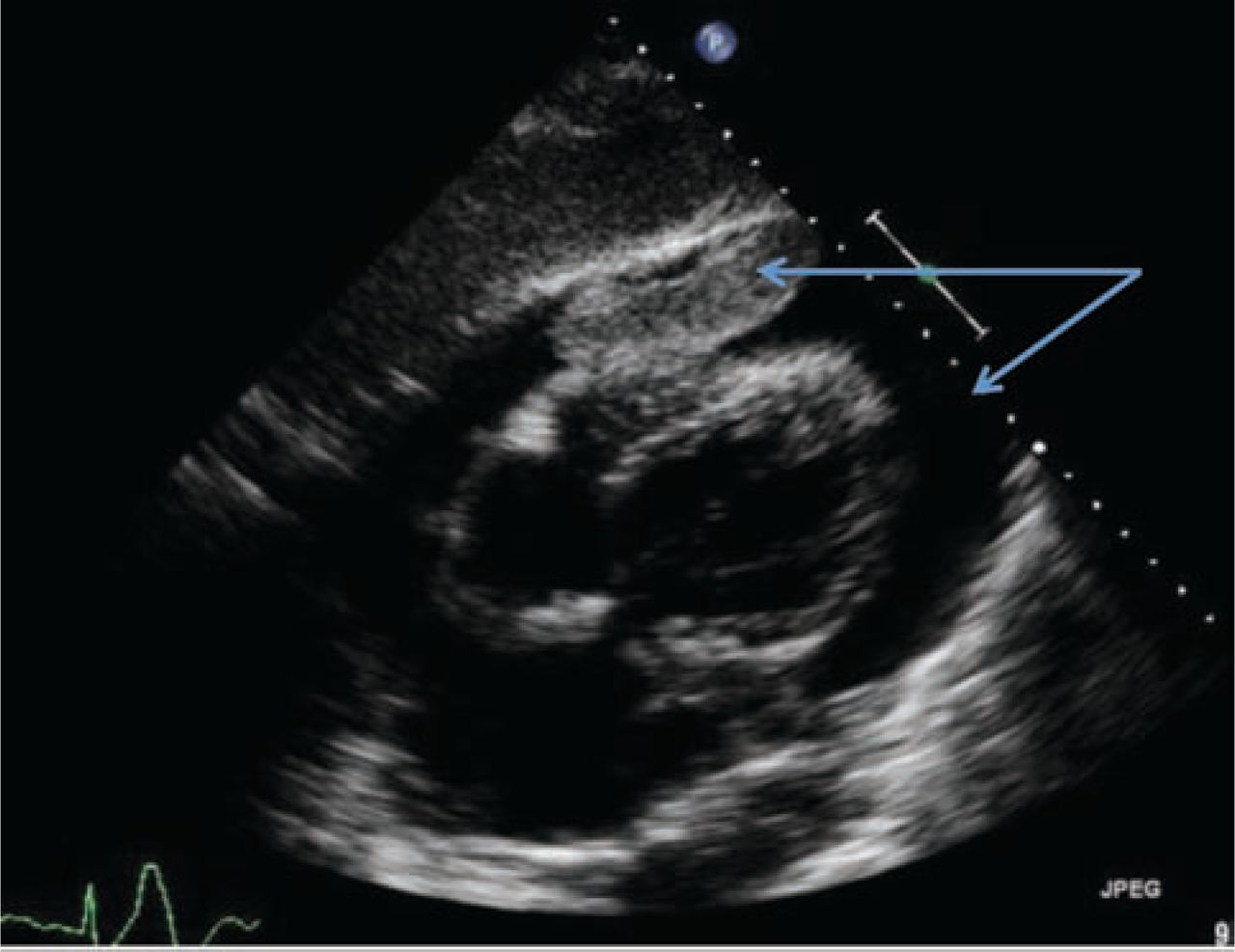
A transthoracic echocardiogram was performed. This showed a moderate pericardial effusion with a mass in the pericardial space compressing the right ventricle. Respiratory variation of Doppler velocities across the mitral and tricuspid valve suggested tamponade. Collapse of the inferior vena cava during inspiration was impaired. Left ventricular size and function were normal (Fig 1).
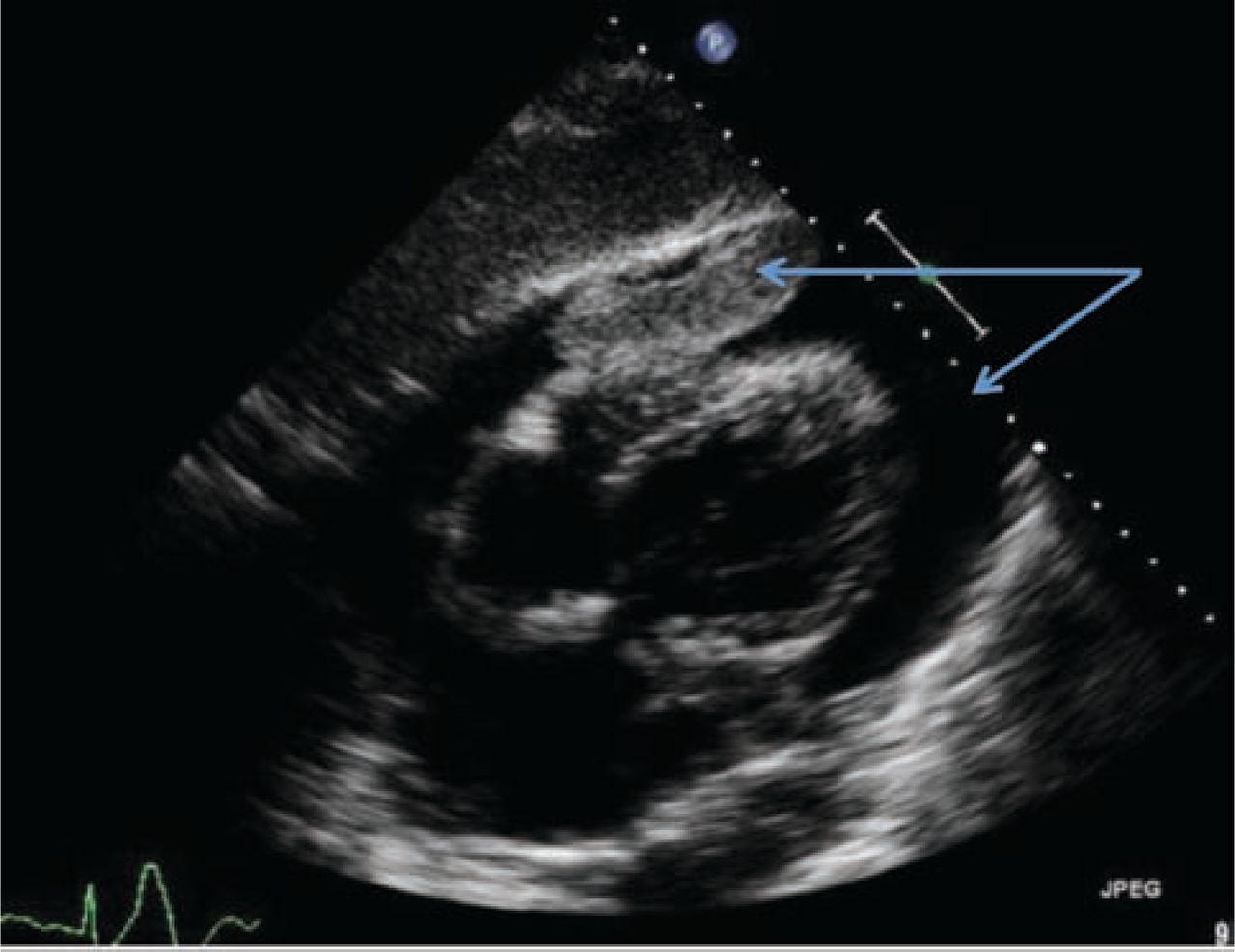
Transthoracic echocardiogram on admission. The pericardial mass with diastolic compression of the right ventricle is seen (shown by arrows). Respiratory variation of Doppler velocities across mitral and tricuspid valves suggests cardiac tamponade.
The patient's computed tomography (CT) scan of the chest/abdomen/pelvis confirmed a small, right-sided, pleural effusion with right basal consolidation. A large pericardial effusion was noted and there was an anterior mediastinal soft-tissue mass by the right lower lobe and pulmonary artery.
The patient was transferred to a tertiary centre for further investigations and drainage of the pericardial fluid. Subsequent cardiac magnetic resonance imaging (MRI) showed a large pericardial effusion with a mass in the pericardial space. There was also a mass posterior to the left atrium, which suggested a benign bronchial cyst.
The patient underwent a right-sided, video-assisted, thoracoscopic pericardial window using pericardial fenestration. A volume of 800 ml pericardial fluid was drained and the pericardial mass was biopsied. Samples were sent for microbiology and histology.
The pericardial fluid was negative for acid-fast bacilli and fungal cultures. The pericardial biopsy demonstrated chronically inflamed pericardial tissue. Biopsy of the pericardial mass revealed an organising thrombus.
The patient was treated with amoxicillin and clavulanate (Augmentin), and clarithromycin. She made an excellent clinical recovery and her inflammatory markers returned to normal.
Subsequent follow-up echocardiography showed no residual pericardial effusion, normal left ventricular function and no evidence of valvular abnormalities (Fig 2).

Normal follow-up transthoracic echocardiogram with a structurally normal heart. LA = left atrium; LV = left ventricle; RA = right atrium; RV = right ventricle.
Repeat cardiac MRI, 4 months post-pericardial drainage and biopsy, demonstrated complete resolution of the pericardial disease. The benign looking posterior mediastinal cyst remained unchanged from the previous scan. The left and right ventricular cavity sizes and function were normal. Myocardial tissue characterisation was also normal.
Key points
Mycoplasma pneumoniae is a common respiratory pathogen that can cause significant cardiac complications, including pericardial mass and cardiac tamponade
This easily treatable entity should be considered in the differential diagnosis of idiopathic pericardial effusions
Discussion
Mycoplasma pneumoniae is a common cause of atypical pneumonia in young adults. Extrapulmonary manifestations are seen in 20–25% of cases and may appear before or after, or coexist with, the pulmonary disease.1 Although extrapulmonary manifestations of M pneumoniae are well described, cardiac tamponade and pericardial masses associated with M pneumonia are rarely reported.
Cardiac complications associated with M pneumoniae are relatively uncommon. The incidence of cardiac involvement is estimated at 4.5% in people with serological evidence of infection. It is more common in adults and has been reported in isolated cases, manifesting largely as myopericarditis.2,3 Proposed hypotheses for M pneumonia-associated carditis include direct invasion of the myocardium by the organism (via the lymphatics, circulation or contamination from the lower respiratory tract), autoimmune mechanisms or increased tendency for intravascular coagulation.4
The present case is a unique example of a plausible association between M pneumoniae and a pericardial mass and effusion, causing cardiac tamponade. It highlights the often forgotten invasive properties of a common respiratory tract pathogen, and emphasises the need to consider this easily treatable entity in the differential diagnosis of idiopathic pericardial effusions.
- © 2014 Royal College of Physicians








{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.