
Pleural effusions are a common problem in both general and respiratory medicine, with pleural fluid aspiration and chest tube insertion being among the most frequently performed medical procedures. Although guidelines advocate thoracic ultrasound in the diagnostic evaluation of pleural effusion, its use is not yet fully established in everyday clinical practice.1 However, a diagnosis of pleural effusion based on only radiographic and physical examination may be misleading and can result in iatrogenic complications.2,3
A 69-year-old man was referred for evaluation of a left-sided pleural effusion. His symptoms included dyspnoea, which had worsened over 6 months, dysphagia and coughing after eating. His chest X-ray (Fig 1) showed a left-sided pleural effusion, mediastinal shift to the right and loculated air in the left mid-zone, which was suspected to be a hydropneumothorax and pleural infection. However, thoracic ultrasound (Fig 2) identified only bowel contents in the left hemithorax with no evidence of pleural effusion. Subsequent computed tomography (Figs 3 and 4) confirmed these findings with evidence of a large left diaphragmatic hernia, bowel and omentum occupying approximately 70% of the left hemithorax, and partial collapse of the left main bronchus due to extrinsic compression. The patient was referred to thoracic surgery for replacement of the hernia and hemidiaphragmatic reconstruction.

Chest X-ray with suspected left pleural effusion.
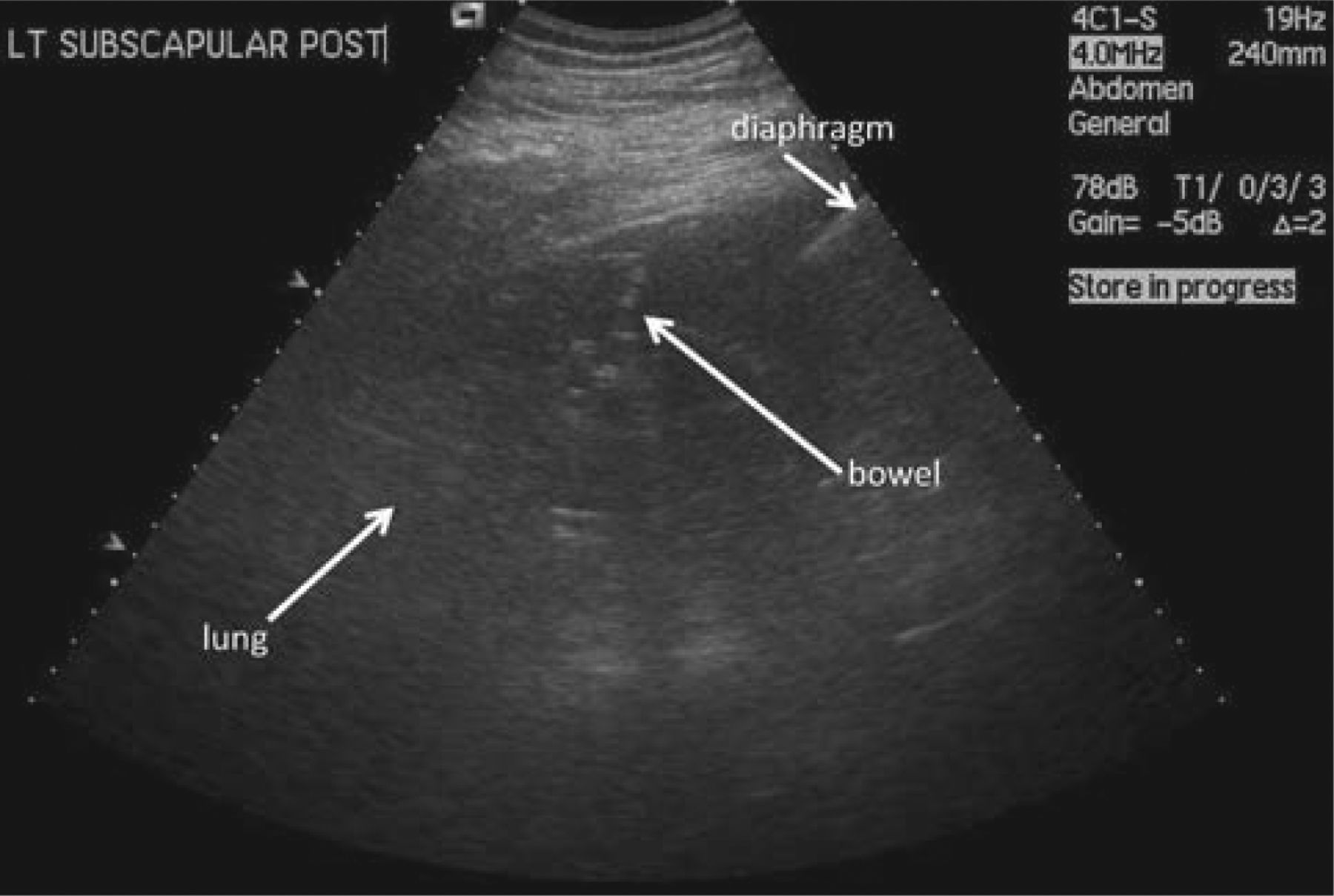
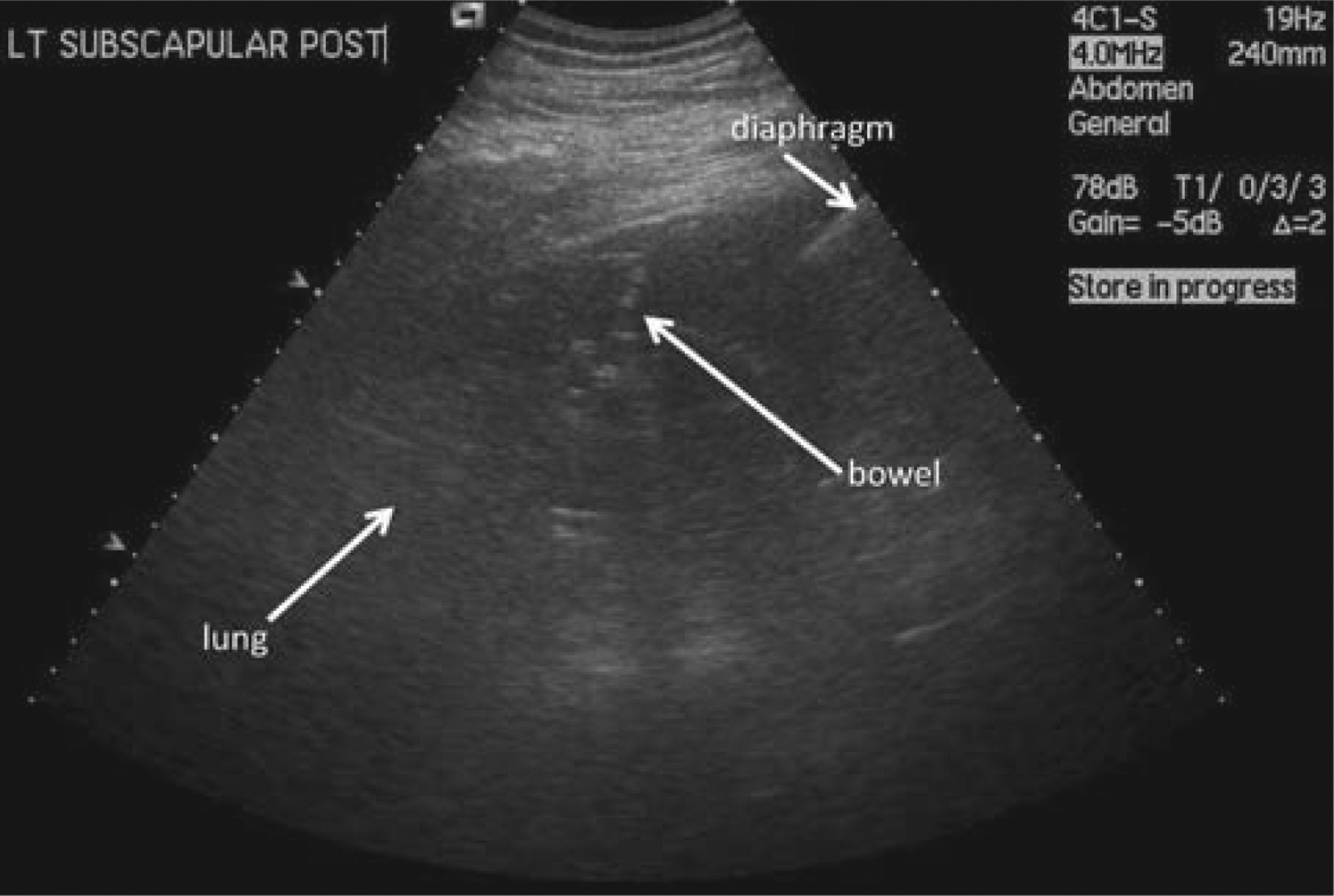
Ultrasound (posterior chest, 4th ICS), showing bowel (mixed echogenicity above diaphragm) with underlying compressed lung. ICS = intercostal space.

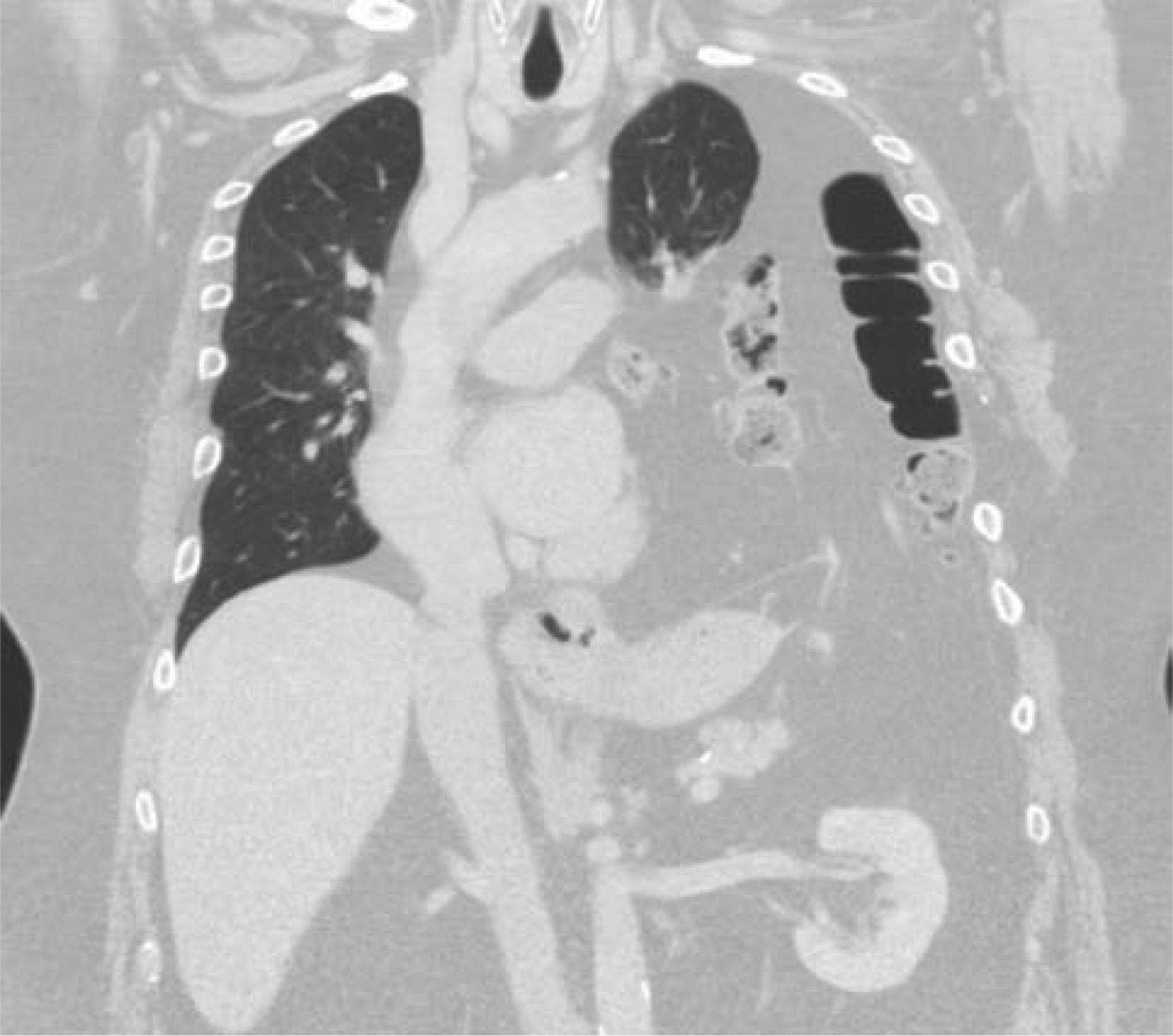
Coronal computed tomography showing abdominal contents extending into left hemithorax.

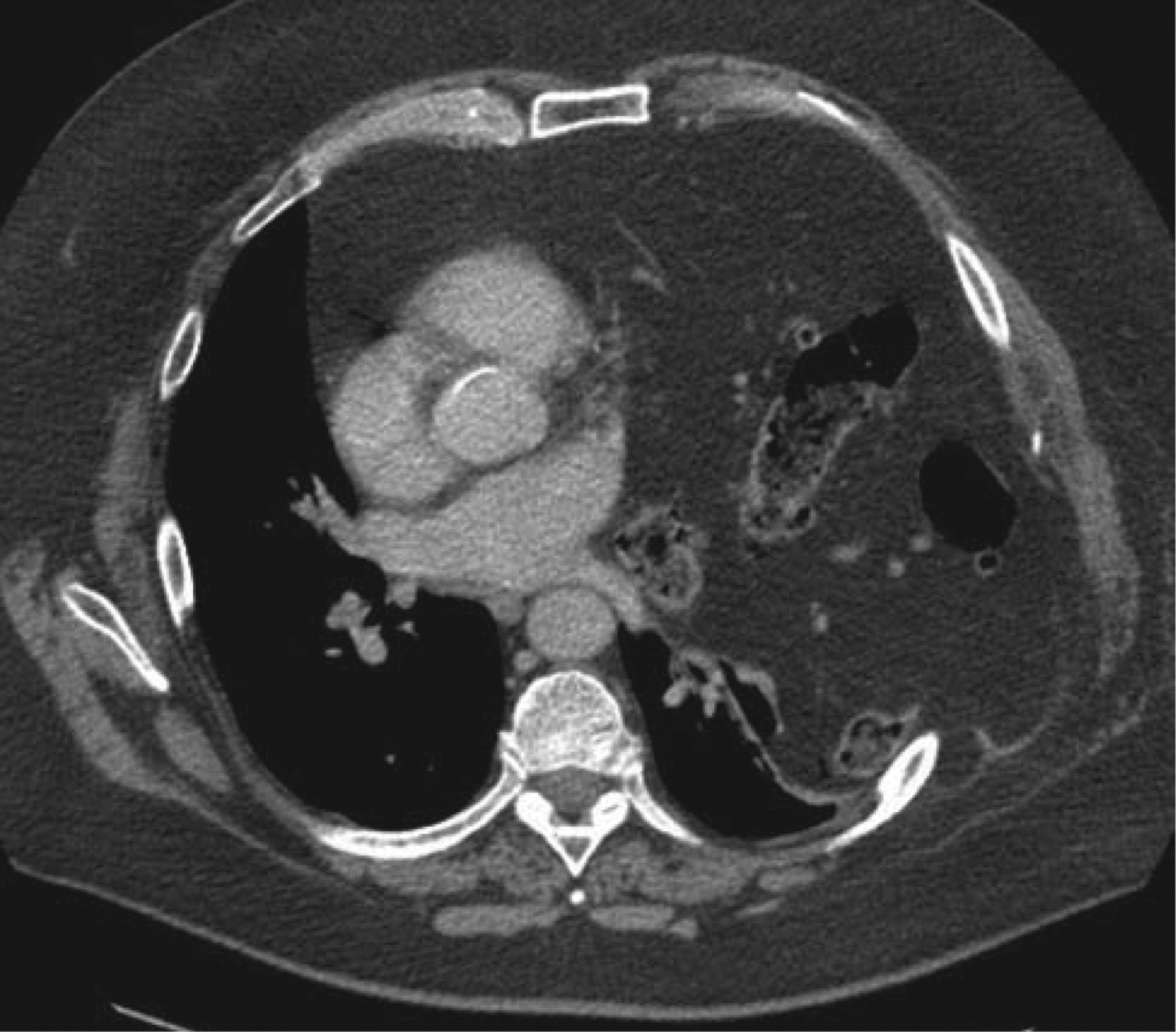
Axial computed tomography showing mediastinal shift and left-sided rib splaying caused by herniation of abdominal contents.
This case reinforces the importance of thoracic ultrasound in the evaluation of suspected pleural effusion as a straightforward, non-invasive and non-irradiating diagnostic technique. Current evidence recommend that ultrasound guided pleural aspirations are associated with lower complications, particularly pneumothoraces and inadvertent organ punctures.4 Current training of respiratory physicians should include the minimum standard requirements from the Royal College of Radiologists to achieve level 1 competency in ultrasound imaging. The increased use of this technique after appropriate training will gradually maximise the potential benefits for patients in the scope of diagnosis and management of pleural diseases.
Acknowledgement
Dr Ioannis Psallidas is the recipient of a European Respiratory Society Fellowship (LTRF 2013–1824).
- © 2014 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.