
ABSTRACT
Gout, classically affecting the first metatarsal joints, knees, fingers and ears, is seldom thrown out as a differential when a patient complains of lower back pain. Symptoms presented by patients with spinal gout may be non-specific and varied; at times, the only clue being that the patient has a previous history of gout. Prompt treatment with anti-inflammatory medication once diagnosis is reached helps to alleviate pain and improves the prognosis of the disease. Therefore, it is vital for the treating physician to keep an open mind and consider spinal gout as a diagnosis once other sinister causes such as osteomyelitis have been ruled out. This greatly reduces the morbidity associated with late treatment of spinal gout.
Background
Gout as a diagnosis rarely comes to mind when faced with a patient experiencing lower back pain symptoms. Since the first ever recorded case of spinal gout was diagnosed,1 very little reference has been made to this in literature. A PubMed search showed that in Singapore, only one case has ever been reported previously.2 Recent studies have shown that spinal gout is under- and misdiagnosed due to its presentation mimicking a varied clinical picture.3,4 Our case report exemplifies this difficulty. We hope to encourage physicians to consider spinal gout as a diagnosis when faced with long standing ‘gouty’ patients who present with new onset lower back pain.
History
Our patient is a 35-year-old man diagnosed with polyarticular tophaceous gout in 2007, for which he has been on long term colchicine and allopurinol and occasional prednisolone. Otherwise he is well with no significant comorbidities. In December 2013, the patient complained of acute lower back pain and reduced lumbar extension. This was the second time in six months he had this symptom and this time it had worsened progressively over three weeks.
Examination
Physical examination showed severe spinal stiffness with a reduced range of motion. Tenderness over the right paravertebral areas of L1-L2 was noted. There was no suggestion of any neurological deficit although there was decreased straight leg rising. Other joints, more commonly involved in gout, were quiescent and no significant tophi were noted.
Investigations
His full blood count revealed a hemoglobin level of 12.7 g/dl and a white cell count of 9,260/dl. His erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were 69 mm/h and 46.5 mg/l, respectively. The uric acid level was 473 μmol/l. Radiographs showed no definite tophus in the spine and changes equivocal to both spinal gout and spondylodiscitis were noted. A Magnetic resonance imaging (MRI) showed foci of marrow edema with enhancement involving the lumbar spine. Erosion of the superior endplate of S1 and posterior cortex of L5 vertebral body was noted (Fig 1). The findings were suggestive of gout, but to exclude an infective process such as osteomyelitis or spondylodiscitis the patient was scheduled for a needle biopsy (Fig 2). Histopathology of the specimen revealed a small focus of amorphous material surrounded by histiocytes and foreign body giant cells which were highly suggestive of gout. Unfortunately uric acid crystals could not be demonstrated due to improper specimen fixation in formalin causing the crystals to be ‘washed off’. A high level of suspicion is required for spinal gout to ensure proper staining of the specimen in alcohol prior to histopathological examination.2,4 No acid fast bacilli were identified.
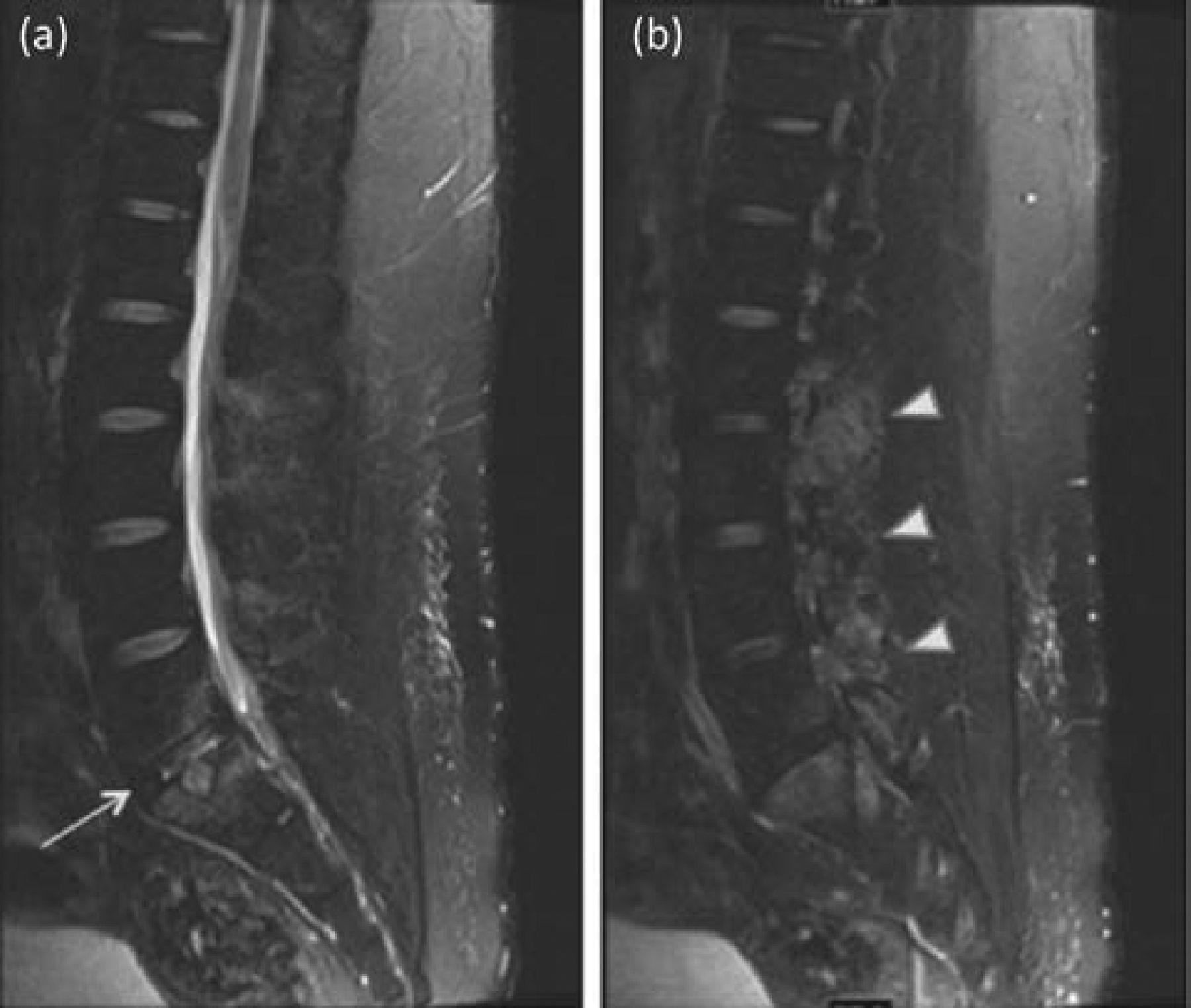
MRI of the lumbar spine. (a) Central and (b) paracentral -sagittal T2 fat saturated images of the lumbar spine show endplate erosions at L5/S1 with surrounding edema (arrow) as well as multilevel facet arthropathy (arrow heads). MRI = magnetic resonance imaging.

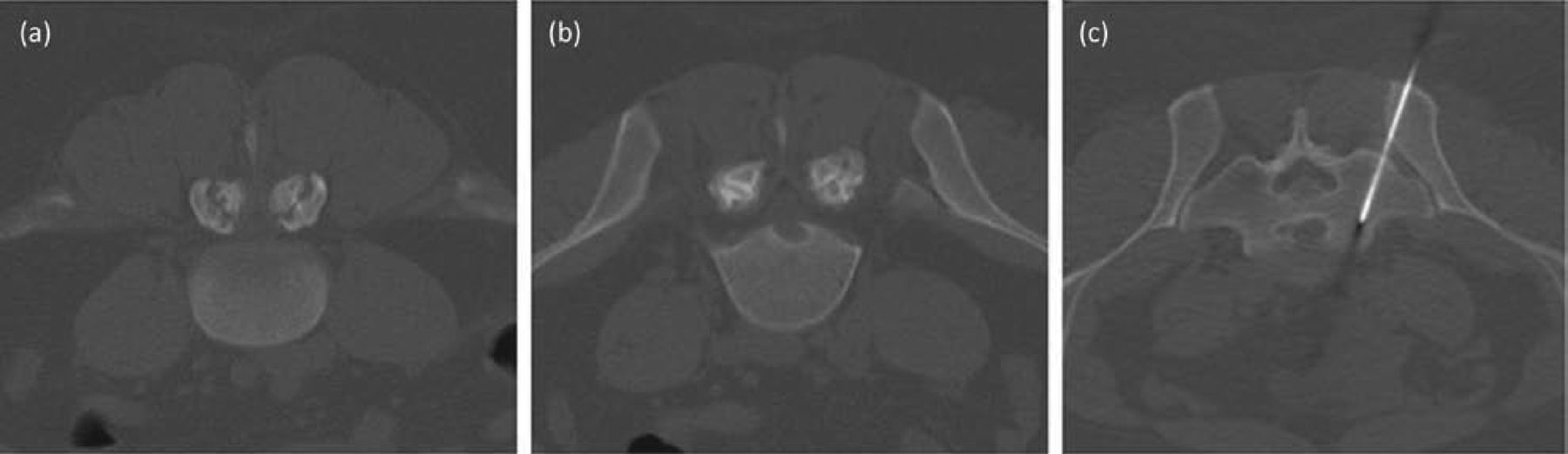
CT images of vertebral bodies. Axial CT images of (a) L4 and (b) L5 vertebral bodies demonstrate subchondral erosions at the facet joints as well as a punched out erosion with sclerotic margins at the posterior cortex. (c) CT guided biopsy at L5/S1 level. CT = computed tomography.
Management
The patient's symptoms improved greatly with bedrest, painkillers and anti-inflammatory medication. He was subsequently discharged with a short course of prednisolone and his regular medication of colchicine and allopurinol were continued. He has also been scheduled regular appointments at the rheumatology outpatient clinic for follow up.
Discussion
Gout is a crystal arthropathy characterized by the deposition of uric acid in the joints. Common joints involved include the first metatarsal, elbows, knees, fingers and ears. Spinal involvement is relatively uncommon, although the frequency of axial involvement has been suggested to be as high as 14–35%.5–7,9 The majority of these patients develop gout in the lumbar region,6,7 and it can affect any part of the vertebral body, including the epidural space, ligamentum flavum, pedicle or facet joint.8 Some patients are asymptomatic; otherwise, presenting symptoms range from simple back pain to myelopathy and radiculopathy, which is the most common symptom, occurring up to 34.5% of cases (including this one).7 Elevated temperature, total white counts, ESR and CRP are also seen in some patients.7 The hypermetabolic nature of presentation of spinal gout mimics infective, inflammatory and neoplastic etiologies such as osteomyelitis, spondylodiscitis, Pott's disease, abscesses and metastasis, making the accurate diagnosis difficult to reach.4,10 Even in this case, the non-specific presentation had lead to an infective cause being considered for the back pain. Studies have shown that spinal gout is more common in men aged 35–75 years of age with a previous history of chronic polyarticular tophaceous gout that is not optimally controlled.6,8,10 There has also been a positive correlation between the onset of symptoms and serum uric acid level.8 Although MRI and computed tomography (CT) findings have been useful in preliminary diagnosis of spinal gout, the gold standard remains histopathological examination where urate crystals can be demonstrated under polarized light.8–10 Proper specimen collection avoiding formalin also needs highlighting in order not to miss the microscopic evidence of gout, as in our case. Once the diagnosis is reached, spinal gout can be controlled medically with the use of nonsteroidal anti-inflammatory drugs (NSAIDs), allopurinol and colchicine, which have been shown to be effective in controlling symptoms as an alternative to definite surgical treatment.7–9 In summary, spinal gout can result in a varied clinical presentation and it should be considered in all patients with a known history of gout and presenting with new onset back pain or neurological compromise.5,7,8,10
- © 2014 Royal College of Physicians








{kind=link}
{kind=link}