
ABSTRACT
Many patients with heart failure (HF) have a normal left ventricular ejection fraction, and are labelled as having HF with preserved left ventricular ejection fraction (HFPEF). Hypertension, atrial fibrillation and age are important contributors to the development of HFPEF and, therefore, its prevalence is likely to increase in the next few decades. The pathophysiology of HFPEF is heterogeneous but with a final common pathway leading to congestion. HF remains a clinical diagnosis but the plasma concentration of B-type natriuretic peptide (eg BNP/N-terminal prohormone BNP (NT-proBNP)), a marker of congestion, is an essential component. Imaging, usually by echocardiography, is required to determine the cardiac phenotype (ie valve disease, left ventricular ejection fraction) underlying HF. A superficially normal echocardiogram does not exclude a diagnosis of HF. No treatment has been shown conclusively to alter the prognosis of HFPEF. However, treatments directed at congestion and hypertension, such as diuretics, mineralocorticoid receptor antagonists (MRAs) and angiotensin converting-enzyme inhibitors, may improve symptoms and probably do improve outcomes. No treatment has yet been shown to reverse the underlying myocardial pathology of HFPEF, although there is some hope that MRAs might.
Introduction
Breathlessness on exertion is extremely common; it causes substantial disability and has many causes, including heart failure (HF). In England, HF causes or contributes to about 400,000 emergency admissions to hospital each year. About 10–15% of these patients will die in hospital and more than 20% of those surviving admission will die in the following year, many of them subsequent to a further admission.1
Many epidemiological reports suggest that about half of patients who have symptoms or signs of HF have a relatively normal left ventricular ejection fraction (LVEF) and are labelled as having HF with preserved ejection fraction (HFPEF). In the coming decades, as the population ages, the prevalence of diabetes, obesity and hypertension increases and survival after myocardial infarction improves, the substrate for developing HF and its incidence will therefore increase dramatically.2,3
Over the last 25 years, several effective therapies have been identified for patients who have HF with reduced ejection fraction (HFREF) but none have been conclusively shown to be effective for HFPEF. This may reflect problems in either the veracity of the diagnosis of HF or the heterogeneous pathophysiology of HFPEF that renders it unamenable to a single therapeutic approach.
What is HFPEF?
Many attribute HFPEF predominantly to left ventricular diastolic dysfunction (DD). However, many patients with DD have no readily identifiable symptoms. They may become breathless during exercise but this is often attributed to age and low levels of fitness. They are probably more prone to developing clinically overt HFPEF but DD is not an accurate predictor of risk.4 The underlying myocardial pathology appears to be heterogeneous but many patients have left ventricular and cardiac myocyte hypertrophy with impaired relaxation and an increase in myocardial collagen content indicating fibrosis. Opinions differ on which is most important in HFPEF; most likely this varies among patients. In some patients, scars indicating subclinical myocardial infarction can be found. Amyloid may be an under-recognised problem, especially senile or transthyretin cardiac amyloidosis, which run a more benign course than light-chain induced amyloidosis.5
Breathlessness on exercise is the key clinical marker of HFPEF. Patients with HFPEF and controls often have a similar haemodynamic profile at rest. The haemodynamic hallmark of HFPEF is an exaggerated rise in pulmonary capillary wedge pressure and pulmonary artery pressure during exercise.6 This is accompanied by a failure of LV end-diastolic volume to increase during exercise (impaired diastolic reserve) due to impaired left ventricular relaxation and increased left ventricular stiffness,7,8 leading to an attenuated increase in stroke volume and cardiac output. Exercise-induced mitral regurgitation and left ventricular dyssynchrony may also contribute to abnormal haemodynamics and impaired exercise capacity.9 However, skeletal muscle deconditioning and respiratory and joint disease most likely also have an important impact on exercise capacity.
HFPEF-associated morphological changes occurring in the heart structure include focal (scar, due to myocardial infarction) or diffuse (due to hypertension or inflammation) fibrosis, leading initially to a decline in long-axis LV systolic and diastolic function.10 Systolic and diastolic segmental impairment of LV function, such as a reduced radial function and apical rotation, or delayed LV untwisting, can also be detected with advanced echocardiographic methods.11
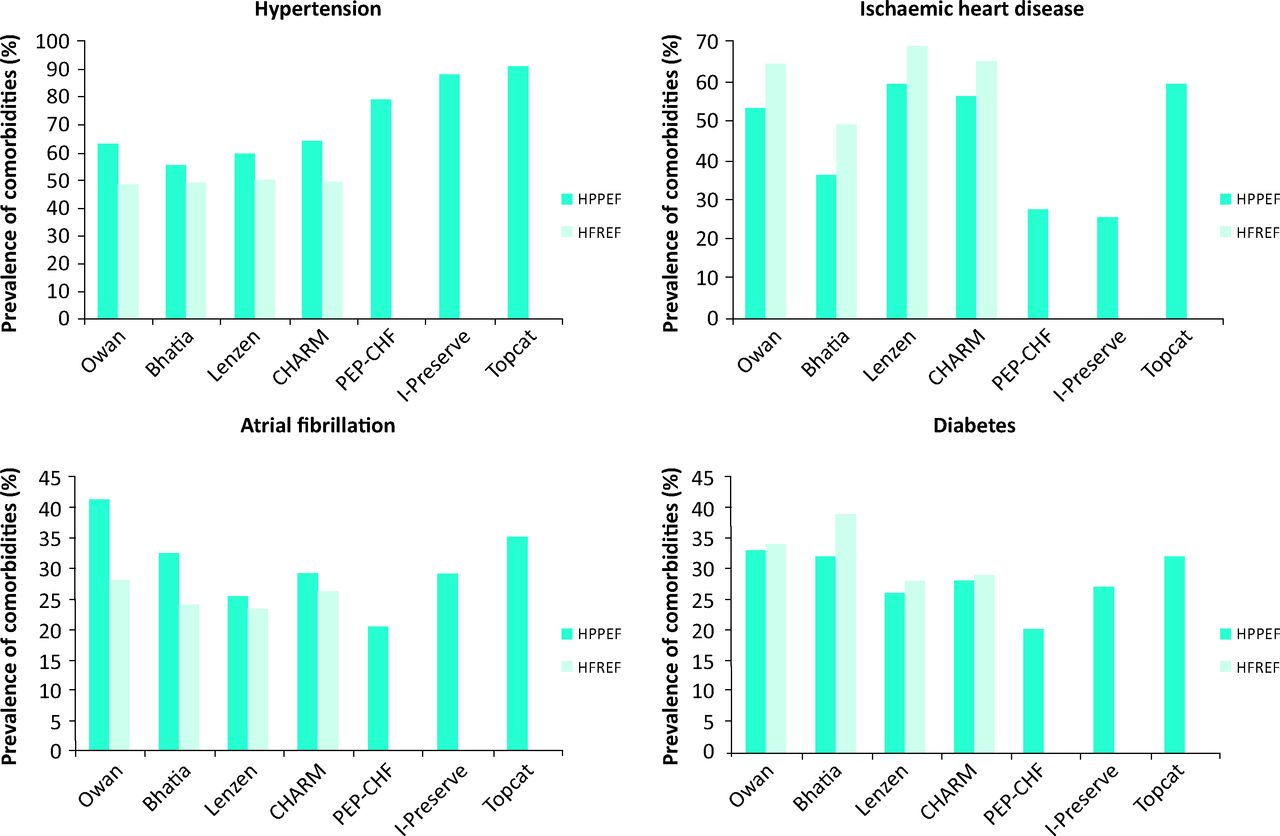
However, HFPEF is a disease of the elderly and it is not surprising that several comorbidities have a higher prevalence among patients with HFPEF than in those with HFREF (Fig 1), including atrial fibrillation, anaemia, chronic obstructive pulmonary disease (COPD), renal dysfunction and, most notably, hypertension. Many of these will actively contribute to the development of HFPEF and are not merely ‘bystanders’. Arterial stiffening is another age-related process that is both a cause and consequence of hypertension that may increase LV afterload at rest, and which may be exaggerated during exercise.18
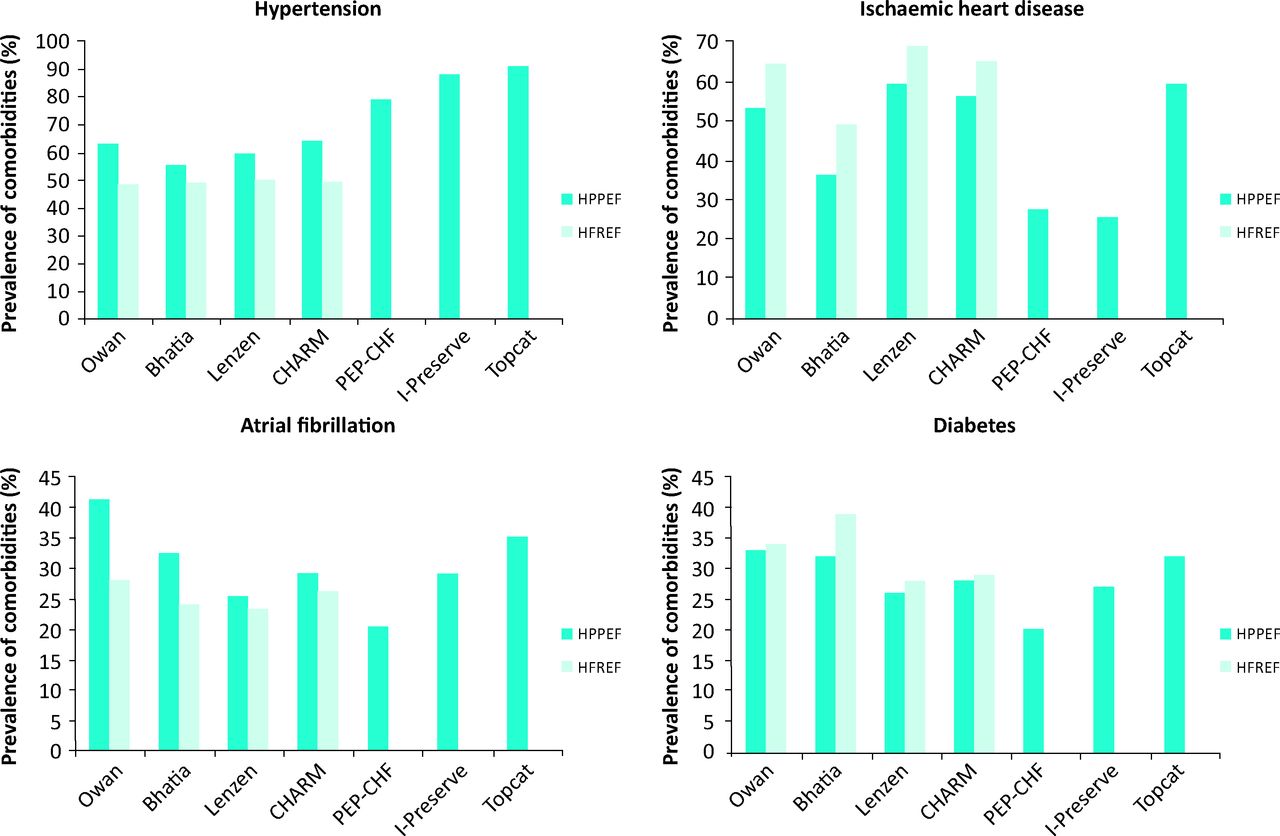
Prevalence of important comorbidities (atrial fibrillation, hypertension, ischaemic heart disease and diabetes) among patients with -HFPEF compared with those with HFREF in observational studies and relevant clinical trials.12–17 HFPEF = heart failure with preserved left -ventricular ejection fraction; HFREF = HF with reduced ejection fraction.
Thus, from a narrow cardiology perspective, HFPEF can be considered a clinical condition characterised by both systolic and diastolic left ventricular dysfunction. However, from a broader clinical perspective, HFPEF might be considered an age-related syndrome with LV dysfunction as only one component of a multi-system disorder that contributes to symptoms (breathlessness) and signs (peripheral oedema).19
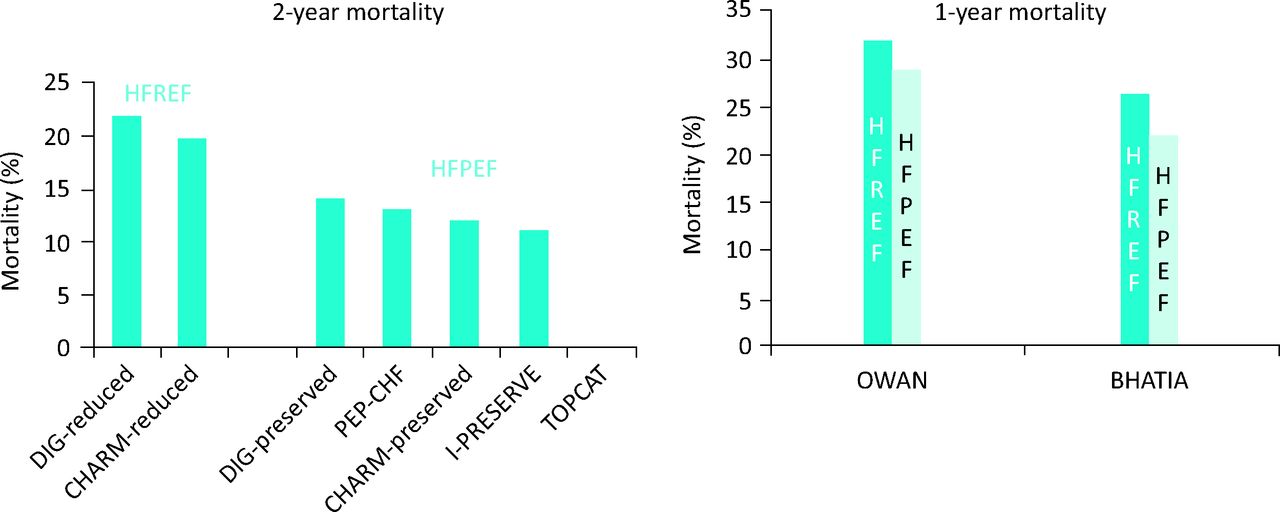
Reports from registries suggest that the outcome of patients with HFPEF and HFREF might be similar,12 but clinical trials (that usually exclude patients with comorbidities that cause diagnostic confusion) have not confirmed this (Fig 2). The poor prognosis of HFPEF may reflect the concomitant effects of greater age and the number of other serious comorbidities, rather than the severity of cardiac dysfunction.
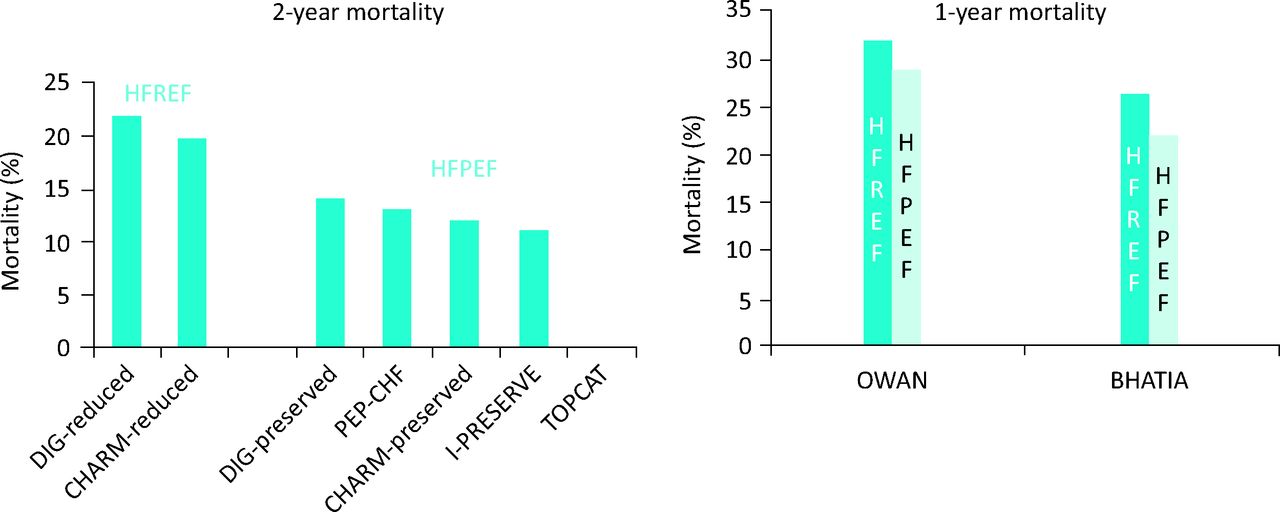
Mortality in trials (left) and observational studies (right) in HFPEF and HRFEF.3,12 HFPEF = heart failure with preserved left ventricular ejection fraction; HFREF = heart failure with reduced ejection fraction.
How is HFPEF diagnosed?
The diagnosis of HFPEF is probably often overlooked. Only about one-third of patients treated with loop diuretics are labelled as HF, but when investigated many are found to have cardiac dysfunction. The diagnosis of HFPEF may also often be made in error.9 However it is also likely that HFPEF is a paroxysmal disease. Although LVDD may be consistently present, the evidence for HF may only appear when the heart is stressed by, for example, uncontrolled hypertension, atrial fibrillation, anaemia or infection.19 This explains why many patients admitted with florid features of HF have little or no evidence of the disease at subsequent outpatient follow-up. In a breathless patient, a diagnosis of HF can be made with some confidence when the LVEF is reduced, even when comorbid respiratory disease exists. When LVEF is normal, there are two approaches to the diagnosis of HFPEF: either exclusion of alternative reasons for symptoms and signs and the use of clinical judgment or a diagnosis based on evidence of cardiac dysfunction other than a reduced LVEF. Unfortunately, as noted above, many older patients have abnormal DD but no symptoms.
The 2007 European Society of Cardiology consensus statement required echocardiographic (E/E’ >15) or invasive (raised left atrial or left ventricular filling pressure) evidence of diastolic dysfunction to confirm a diagnosis of HFPEF when LVEF >50%.20 It is worth mentioning that these authors were the first to introduce the use of natriuretic peptides for diagnostic purposes, but only when supported by echocardiographic measurements (E/E’ >8). However, the guidance on natriuretic peptides was flawed for many reasons. Suggested diagnostic thresholds for B-type natriuretic peptide (BNP) (>200 pg/ml) and N-terminal prohormone BNP (NT-pro BNP); >220 pg/ml/l) were inconsistent and no account was taken of heart rhythm or renal function, both of which have a profound effect on the interpretation of results. The recent European Society of Heart Failure (ESC) HF guidelines lowered the cut-off for NTproBNP plasma levels (<125 ng/l) to exclude serious cardiac structural alterations or dysfunction, but the diagnosis of HFPEF still requires identification of diastolic dysfunction by echocardiography.21 Importantly, this set of guidelines suggested that a single echocardiographic variable should not be used to establish a diagnosis, but a more comprehensive assessment of LV structure (volumes and mass), left atrial size and Doppler variables is required. The American Heart Association and the American College of Cardiology (ACC/AHA) guidelines for the management of HF have introduced an important distinction between those patients who have HF and relatively preserved LVEF (>40%), with three groups of patients being identified: ‘possible’ HFPEF (LVEF >50%), ‘borderline’ HFPEF (40<LVEF<49), and ‘improved’ HFPEF (LVEF >40%), for patients who had HFREF whose LVEF had risen but in whom the features of HF had not resolved.22
Although there is still debate about whether HFPEF and HFREF are a continuum of the same disease or two separate clinical entities,23,24 differences exist in pathophysiology, the importance of hypertension and ischaemic heart disease to causation and in treatment.25 Therefore, it is important to identify cardiac phenotypes that are hidden behind the same acronym and a single echocardiographic measurement.
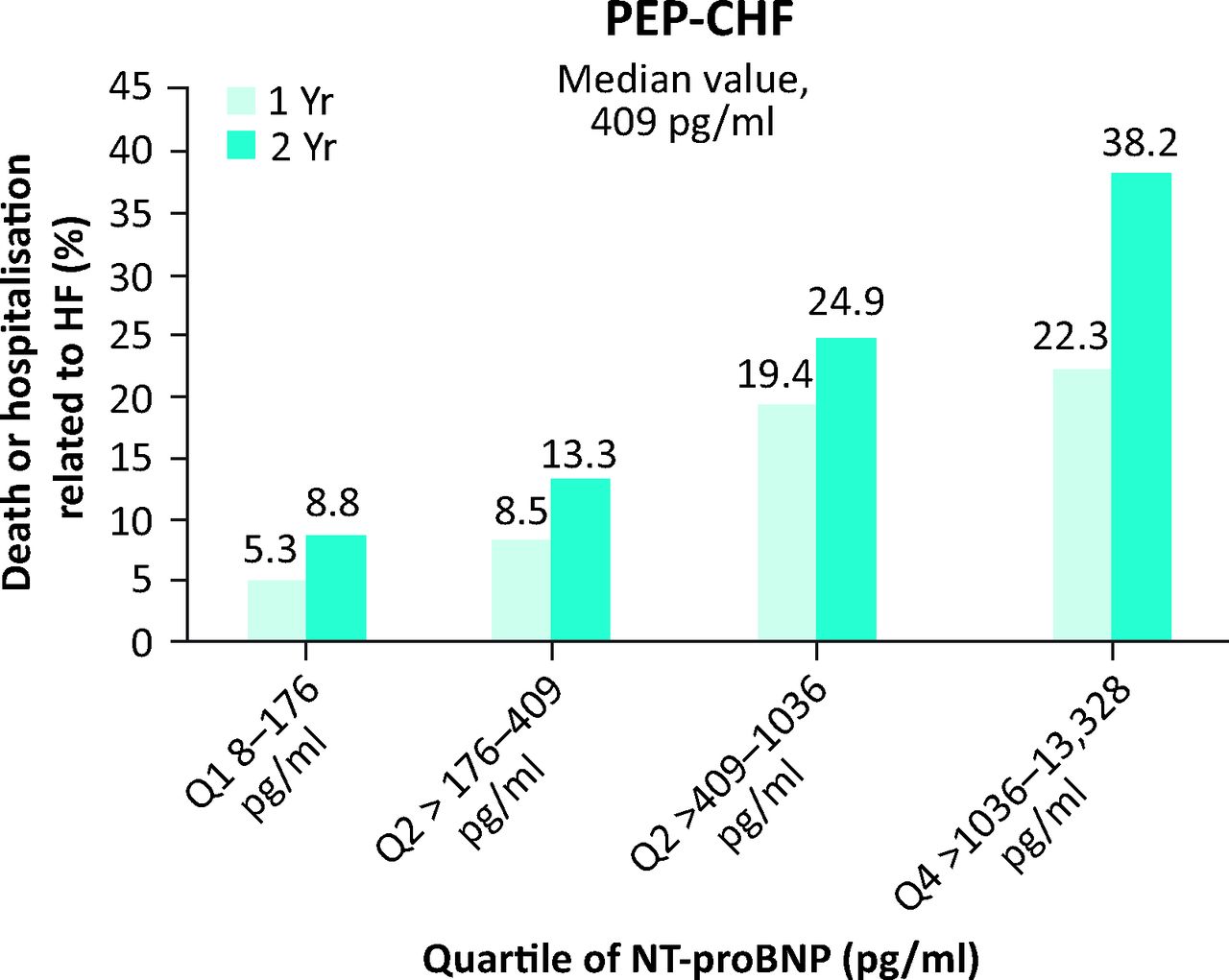
Natriuretic peptides are produced by the heart as a defence against fluid congestion. They are an essential tool to identify both patients with HF and their risk of clinical events (Fig 3).15,26 However, natriuretic peptides are almost completely agnostic as to the cause of congestion, including cardiac or renal causes. The rare exception is constrictive pericarditis, where severe congestion may develop with only a modest increase in natriuretic peptides, the plasma concentration of which reflects transmural wall stress rather than intra-cardiac pressure.27 When natriuretic peptide levels are low, clinicians can generally reassure themselves and their patients that breathlessness or oedema are not cardiac in origin and that prognosis is good.28 Increased plasma concentrations of natriuretic peptides suggest that the heart is stressed and congestion is developing. Plasma concentrations do rise with age, renal dysfunction, the severity of coronary disease, anaemia and heart rhythm disturbances, such as atrial fibrillation, because each of these places a strain on the heart. Each also brings the patient closer to death.29 Only those interested in rationing care to older people should adjust interpretation of plasma concentrations of natriuretic peptides for age.30

Outcome according to quartiles of the plasma concentration of NT-proBNP in patients with HFPEF enrolled in the PEP-CHF study. Reproduced with permission from Cleland et al.15 HF = heart failure; HFPEF = heart failure with preserved left ventricular ejection fraction; NT-proBNP = N-terminal prohormone B-type natriuretic peptide.
Taking the above to its logical but provocative conclusion, the diagnosis of HF should be based on clinical assessment made in the light of the plasma concentration of BNP/NT-proBNP31 and not be based on echocardiography. However, imaging plays an essential role in identifying the cardiac phenotype and probable cause of HF by assessing LV contractile function, left atrial volume and valve function. A broader echocardiographic perspective that focuses on the up-stream consequences of a stiffer left ventricle might be the best method to phenotype this complex disease further and to identify different therapeutic targets.32 Other data suggest that assessing RV function or even the vena cava may be a better guide to prognosis than measures of left heart function, but these may be late findings that are of less value for diagnosis.33
How should HFPEF be managed?
Current ESC guidelines21 highlight that there is, so far, no robust evidence that any treatment can reduce morbidity and mortality in patients with HFPEF (Fig 4).

Primary outcomes of large, contemporary randomised controlled trials of HFPEF.14–17 Primary outcome definitions: CHARM-Preserved: cardiovascular death or admission to hospital for chronic HF; PEP-CHF: composite of all-cause mortality and unplanned HF related hospitalisation; I-PRESERVE: death from any cause or hospitalisation for a cardiovascular cause (HF, myocardial infarction, unstable angina, arrhythmia or stroke); TOPCAT: death due to cardiovascular causes, aborted cardiac arrest, or hospitalisation for the management of HF. CI = confidence interval; HF = heart failure; HFPEF = heart failure with preserved left ventricular ejection fraction; HR = hazard ratio. Images reproduced with permission.14–17
Diuretics (either loop diuretics or thiazides) offer an effective treatment for congestion and the rapid relief of symptoms that may also improve quality of life.34 There are fears that conventional diuretics may accelerate the progression of cardiovascular dysfunction by activating the renin–angiotensin–aldosterone system. There is a powerful body of evidence that thiazide diuretics reduce morbidity and mortality among older patients with hypertension,35,36 many of whom probably had or would soon develop HFPEF. There is no such evidence for loop diuretics.
Calcium-channel blockers (CCB), a class of drug contraindicated in patients with HFREF, improved exercise tolerance and LV diastolic function in small studies of highly selected patients with HFPEF, as shown by two small crossover studies conducted in the 1990s that used verapamil.37,38 Calcium channel blockers might also be used for ventricular rate control for patients in atrial fibrillation, although the optimal target heart rate is unknown.39 A recent trial compared two CCB (verapamil and diltiazem) to two beta blockers (BB) (metoprolol and carvedilol) in a randomised cross-over study that enrolled 60 patients with permanent atrial fibrillation and grossly elevated plasma concentrations of NT-proBNP (mean 1039 [SD 636] ng/l) that could not be attributed solely to atrial fibrillation, although none of the patients had overt HF. The rate of adverse events leading to discontinuation of medication was relatively high (25%), mainly related to the use of BB (10 patients reported fatigue and dyspnoea while taking BB, versus only two on CCB). Treatment with CCB, but not with BB, preserved exercise capacity and was associated with a decline in NT-proBNP compared with baseline.40
It is likely, although the evidence is not conclusive, that patients with HFPEF benefit from treatment with angiotensin-converting-enzyme (ACE) inhibitors. Hypertension commonly causes or contributes to the development of HFPEF and lowering blood pressure might be expected to delay the onset or progression of HF.
In the HYVET study,36 3,845 elderly patients (mean age of 84 years, 60% female) were randomised to indapamide (with or without perindopril) or placebo: a significant reduction in the development of HF and in mortality was observed after a follow-up period of 1.8 years. In the PEP-CHF trial, perindopril improved symptoms and exercise capacity at one year and this was associated with a reduction in the rate of composite all-cause mortality and HF hospitalisations (the primary endpoint) that were similar in magnitude to that observed with enalapril in patients with HFREF.15,41 The evidence of benefit for angiotensin II receptor blockers is weaker,14,16 just as it is for HFREF, although, curiously, a subgroup analysis of the I-PRESERVE trial suggests that patients with lower plasma concentrations of natriuretic peptides might derive some outcome benefits.29
Several smaller and two substantial studies of mineralocorticoid receptor antagonists (MRA) have suggested equivocal benefits for patients with HFPEF.17,28,42 The population enrolled in ALDO-DHF had rather mild diastolic dysfunction with little evidence of HF and a good prognosis. In TOPCAT, patients with an elevated plasma concentration of natriuretic peptides, indicating congestion and confirming that they had HFPEF, had a reduction in morbidity and mortality with the addition of spironolactone compared with placebo (Table 1). The magnitude of benefit was similar to that observed in HFREF. Patients who were enrolled based on clinical features alone had few events and did not benefit from spironolactone.
Primary outcome in TOPCAT for patients enrolled because they had a previous HF-related admission in the previous 12 months or an elevated plasma concentration of BNP (>100 pg/ml) or NT-proBNP (>360 pg/ml).
No randomised controlled trial (RCT) has been designed to evaluate specifically the role of BB in HFPEF. SENIORS enrolled more than 2,000 patients with HF, and one-third had LVEF >35%. In a pre-specified sub-analysis, nebivolol exerted a similar 20% reduction in the primary end point (all-cause mortality or cardiovascular hospitalisations) among patients with either HFREF or HFPEF, although the trial was not powered to show a statistically significant effect of nebivolol in different LVEF subgroups.43 Although higher heart rate is associated with an adverse outcome in both HFREF and HFPEF, there is very limited evidence that ivabradine is effective in improving either function or outcome. A moderately large study is underway.
Digoxin is an old drug that should receive more attention. In a randomised trial of 988 patients with clinical HFPEF in sinus rhythm, digoxin reduced the primary composite endpoint of hospitalisation or death due to HF at two years but, disappointingly, the effect was no longer apparent by the end of the study at 37 months.44
New treatments being developed for various forms of cardiac amyloidosis will require greater diagnostic efforts to identify appropriate patients.
Devices
Left ventricular dyssynchrony might contribute to the onset of symptoms in HFPEF, particularly when the QRS interval is prolonged. Although isolated case reports and retrospective analysis of previous studies suggest that some patients with LVEF >40% might benefit from cardiac resynchronisation therapy, no RCT have been reported.45,46 There is no evidence that patients with HFPEF benefit from defibrillators. Implanted monitoring devices might help guide treatment and could be a major advance in management, but their outcome impact is still unknown.47 Similarly, inter-atrial shunt devices, designed to off-load left atrial pressure into the systemic venous circulation in a controlled fashion to prevent the exaggerated rise in left atrial pressure during exercise, could be a novel way to manage patients recalcitrant to conventional management of symptoms.48
Conclusions
HFPEF predominantly affects older patients and is characterised by increased left atrial pressure, especially during exercise, in the absence of LV dilatation or markedly depressed LVEF. Natriuretic peptides are the key means of detecting increases in atrial pressure due to congestion. Education and experience is required to interpret plasma concentrations effectively. Imaging reveals diverse and heterogeneous cardiac phenotypes underlying HFPEF that, in turn, may reflect diverse myocardial pathologies including hypertrophy, delayed cardiac myocyte relaxation, myocardial fibrosis and senile amyloidosis. Treatments directed at congestion (and/or hypertension), such as diuretics MRA and ACE inhibitors, may be similarly effective in HFPEF and HFREF. Treatments directed at myocardial pathology have so far failed to change the natural history of HFPEF as they have done for HFREF.
- © 2014 Royal College of Physicians
References








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.