
ABSTRACT
Barretts oesophagus represents the most significant risk factor for the development of oesophageal adenocarcinoma (OAC), although the majority of patients will not develop cancer. However, early detection of OAC and its precursors significantly improves outcome and underlines the importance of endoscopic surveillance programmes. Clearly there is a discrepancy between the small number of people who need to undergo surveillance because they are at significant progression risk, and the large number that do. Research is therefore now concentrated on risk stratification. Currently such stratification is currently based on clinical findings, endoscopic diagnosis and histopathological grade. Histopathology can be imperfect and is likely to require molecular confirmation of different grades, thus molecular stratification is becoming more important in this regard and p53 immunohistochemistry is already clinically useful, with other molecular biomarkers likely to prove beneficial in the future. The hope is that non-endoscopic methods, such as the Cytosponge™ may be able to combine molecular biomarkers with histopathology and therefore perhaps benefit a population screening as well as a surveillance programme.
Introduction
Oesophageal adenocarcinoma (OAC) has a high mortality with a median overall survival of 1 year; even when a curative modality is attempted, for cases without metastases to distant organs, 5-year survival remains poor.1 There has been a dramatic increase in this disease in the western world over the past 3 decades and, although more recent data have demonstrated that the incidence of OAC might now be plateauing worldwide, in the UK the incidence is increasing and outcome remains poor.2
One of the most commonly associated risk factors with OAC is the development of Barrett's oesophagus (BO). BO is thought to be the result of a metaplasia from the normal squamous lining of the oesophagus to a columnar, glandular phenotype. Although the cellular origin of BO has not yet been clarified, there is strong evidence from epidemiological and experimental data that the aetiology is related to refluxate. BO is characterised by several cell lineages, including intestinal metaplasia, which is the hallmark and the type that predisposes most to adenocarcinoma. The development of cancer is generally gradual through a metaplasia–dysplasia–cancer sequence, which is a well-established progression sequence for several different, particularly epithelial, cancers. The sequence is often considered to be temporally linear: metaplasia develops into dysplasia, either of low or high grade (LGD or HGD, respectively), which is the precursor lesion to adenocarcinoma. Importantly, if adenocarcinoma is detected when it is confined to the mucosa (so-called ‘intramucosal carcinoma’), the 5-year survival rate is 95%, whereas invasion into the deeper submucosa increases the risk of lymph node metastases considerably (from 5% to 40% depending on degree of submucosal invasion) and increases the 5-year mortality.3,4 This is the premise for the importance of early detection in this disease.
Cancers take years to evolve – understanding precursor lesions and early cancers as targets
Sporadic colon cancer, for example, is known to take 5–15 years to develop and is preceded by adenomas comprising LGD or HGD.5 Prostate, cervical, bladder and breast cancers are all epithelial cancers with precursor lesions that take many years to evolve before invasive cancer occurs (Table 1).
Examples of cancers and their associated precursor lesions.
Therefore, detectable precursor lesions represent an ideal target for the prevention of cancer development. Such strategies are already integral to several cancer prevention programmes. For example, the UK Bowel Cancer Surveillance Programme screens for the detection of cancer and uses a guideline-based follow-up of adenoma detection and eradication.6 Another example is the Japanese model of gastric cancer screening. Since the introduction of the national gastric cancer screening programme in Japan, the detection of early gastric cancer has increased significantly with a consistent decrease in patient mortality.7
Given the importance of early cancer detection and the possibility of treating cancer precursor lesions to prevent cancer development, the question arises concerning how we can best achieve this goal given the low progression rate in BO. At the two ends of the spectrum should we be investigating only patients with upper gastrointestinal (GI) symptoms, those who are considered to be high risk based on clinicopathological features, or should we consider population screening?
The evidence for surveillance
Several studies have demonstrated that the overall risk of developing OAC in patients with non-dysplastic BO is small, with two large population-based cohort studies concluding that the per patient risk of OAC is between 0.12% and 0.16% per year. Patients were at greater risk if goblet cells were present (intestinal metaplasia) and with longer Barrett's segments (>3 cm).8,9
Given the low rate of OAC development and that surveillance programmes exist in most western countries, it is worth considering what the impact of surveillance regimes has been on the development of OAC or its mortality. Although several studies found a positive impact on survival,10,11 the most recent study from Kaiser Permanente in the USA argues against the need for surveillance.12 This case-control study by Corley et al matched 38 OAC deaths by age, year and place of diagnosis, sex and race, with 101 controls (patients with Barrett's but who did not die from oesophageal adenocarcinoma by the end of the study, although patients in this group could still have oesophageal cancer) from a large database kept between 1995 and 2007. The authors concluded that a surveillance gastroscopy within 3 years of the diagnosis of cancer did not decrease the risk of death from OAC. This study highlights some of the challenges related to determining surveillance impact in an area where endoscopic technologies and treatments change and where surveillance might not be standardised. Of the patients in this study who developed cancer, 47.4% had previously been found to have dysplasia before cancer development and, in those who had developed cancer, approximately 50% had cancer diagnosed at an advanced stage, indicating that the quality of the surveillance was poor. Therefore, their study underlines the need for high-quality surveillance according to strict protocol. Furthermore, whereas treatment by oesophagectomy would have been available for HGD in this historical cohort, the more successful endoscopic therapies, such as radiofrequency ablation, which are now preferred for early disease, would have only been available after this cohort was collected. Thus, this interesting study not only highlights the difficulty of assessing historical data and retrospective studies, but also underlines the importance of stratifying patients according to their risk of developing cancer, especially given the ability of current endoscopic therapy to eradicate earlier oesophageal precursor lesions.
The growing emphasis on targeting the right patients for surveillance
Therefore, the standardisation of clinical care for BO is an important part of assessing the true impact of surveillance programmes. The UK guidelines for the diagnosis and treatment of Barrett's have recently been updated.13 Important evidence-based changes have been introduced that start to clarify how patients can be risk stratified according to clinicopathological features (Fig 2).
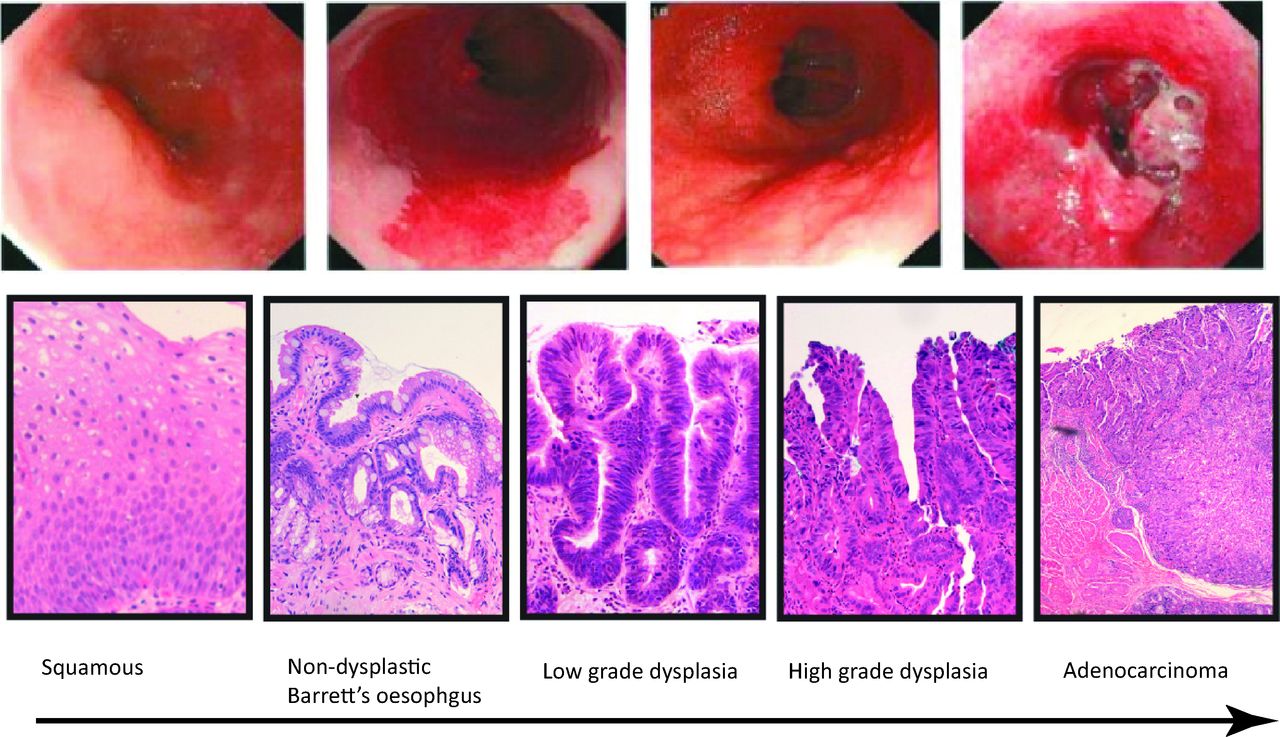
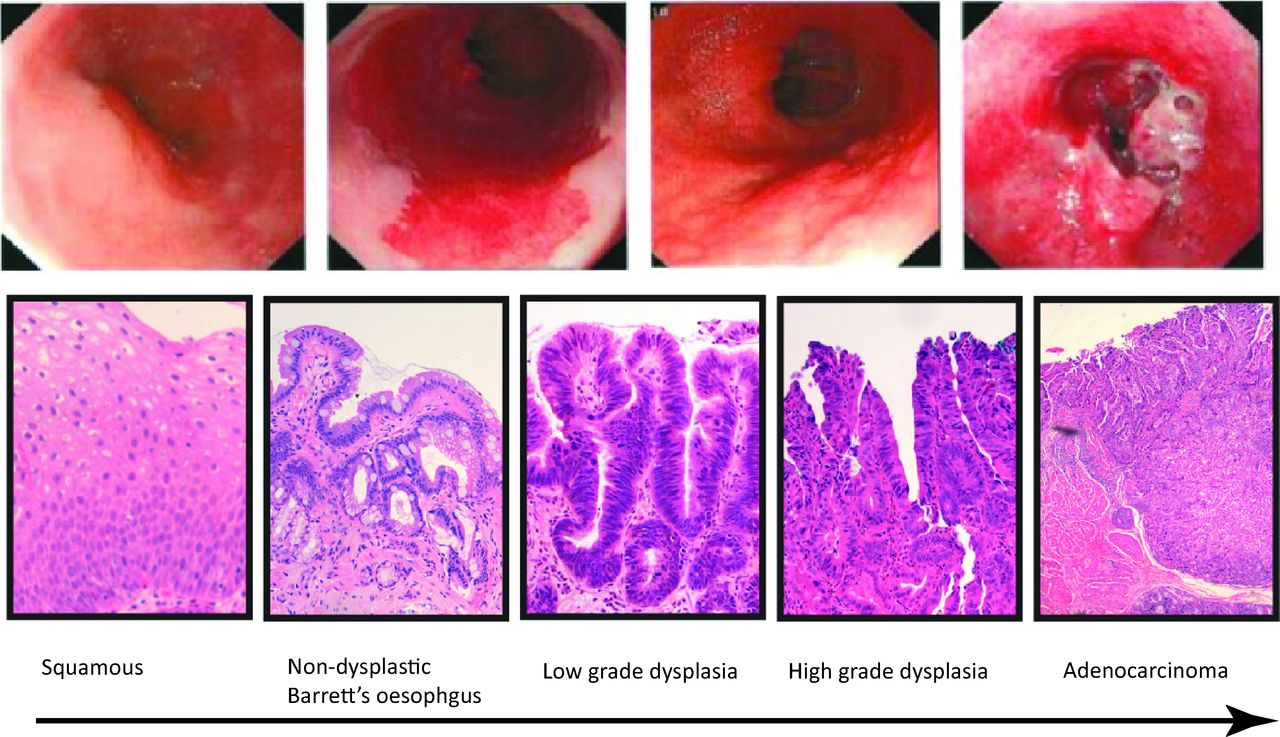
An endoscopic (top panels) and histological (bottom panels) description of the development of oesophageal adenocarcinoma in patients with Barrett's oesophagus. The initial lining of the oesophagus comprises squamous cells. These are then replaced by non-dysplastic columnar cells with or without goblet cells. In a few patients, further molecular and genetic aberrations result in low- and then high-grade dysplasia. The latter is the immediate precursor of, and often coexists with, adenocarcinoma.

Algorithm for the endoscopic evaluation and follow-up for patients with non-dysplastic Barrett's oesophagus. *Interval depends on the degree of clinical confidence about diagnosis (accuracy of endoscopic report and number of biopsies). Reproduced with permission from Gut.13 OGD = oesophago-gastro-duodenoscopy.
Clinical stratification
The Prague classification for endoscopic reporting of Barrett's segments, which reports the circumferential extent (denoted C for circumferential and the length in cm) as well as total extent (taking tongues of Barrett's into account (M)) from the gastrooesophageal junction, is now a standard endoscopic reporting descriptor. This should be combined with the Paris classification, which standardises the description of visible oesophageal lesions. As regards risk stratification, several studies have demonstrated that patients with longer Barrett's sections (>3 cm) at endoscopy are considered to be at higher risk14–16 of OAC progression and, therefore, the intensity of endoscopic surveillance is modified between 2 and 5 years accordingly.
The need for high-quality, high-resolution endoscopy
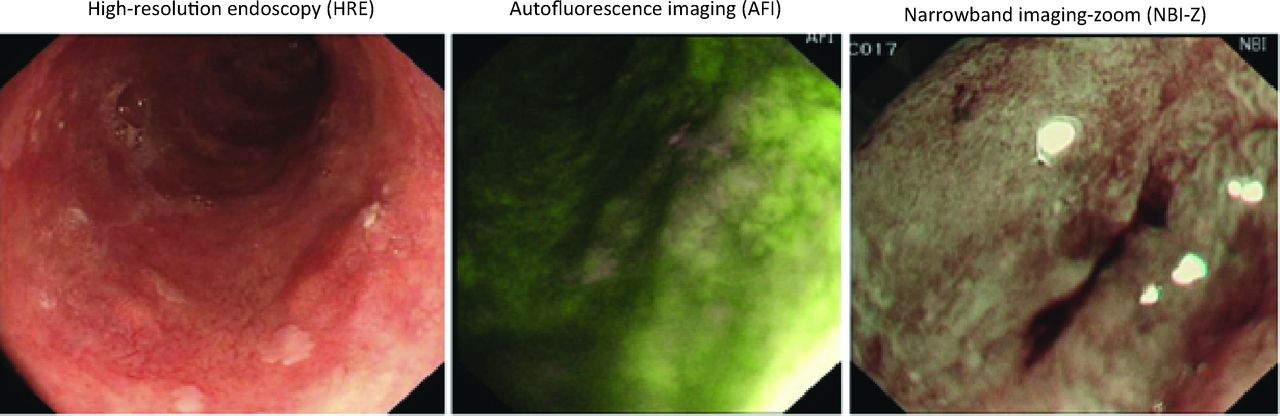
The need for accurate and high-quality endoscopy has also increased in importance as treatment for early OAC becomes more accurate and targeted. Much progress has been made with endoscopic modalities for early OAC and HGD treatment, but these treatments rely on the recognition of lesions, which can be subtle. The endoscopist's tool-kit contains several modalities to enhance lesion recognition, including autofluorescence, narrowband imaging, confocal microscopy and chromoendoscopy (Fig 3). Although still experimental, the ability to target suspicious areas at endoscopy reduces unnecessary sampling and can increase the yield of potentially treatable areas.17 Given that modalities such as radiofrequency ablation with or without endoscopic or submucosal mucosal resection are now curative in most cases, including early OAC, such targeting is of paramount importance.
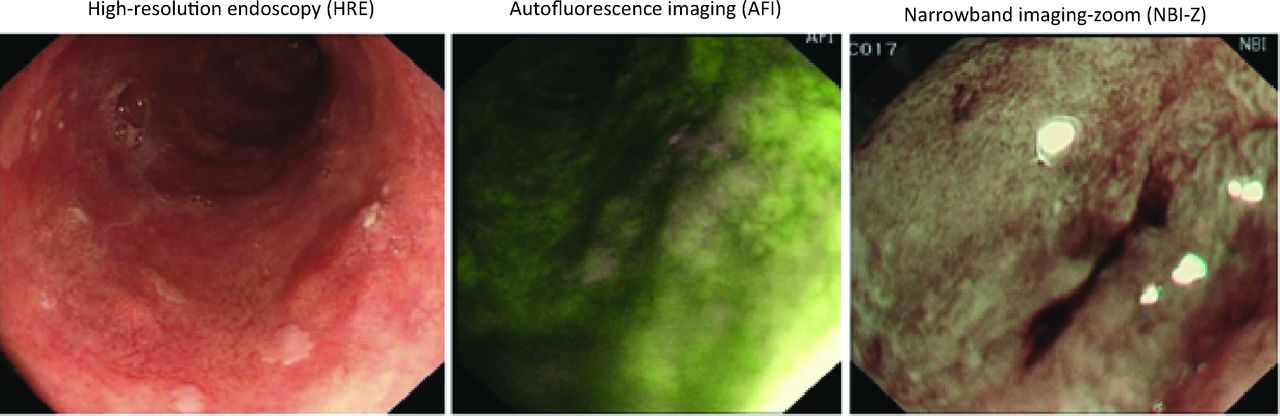
Different endoscopic modalities for the examination of a Barrett's segment. AFI = autofluorescence imaging; HRE = high-resolution endoscopy; NBI-Z = narrowband imaging-zoom.
Histological stratification
Histologically, although the presence of intestinal metaplasia is not a prerequisite for the diagnosis of BO, as it is in North America, its presence might also indicate a higher risk of OAC development9,18,19 and, therefore, endoscopic follow-up of these patients is also stratified accordingly. A key emphasis is placed on the fact that, if the patient has gastric metaplasia without goblet cells, and the Barrett's segment is less than 3 cm, then discharge from surveillance should be considered because the risk of endoscopy might outweigh the benefit of surveillance. Given the importance of a histological diagnosis, the guidelines also stress the need for histopathological quality control, particularly in relation to dysplasia grade, because this can trigger a therapeutic intervention with endoscopic therapy. The detection of LGD carries a hazard ratio of 5.67 for the development of HGD and OAC combined.9 Historically there have also been different treatment pathways based on the detection of LGD and HGD; thus, the lack of consensus in diagnosing dysplasia subtypes between histopathologists has been of concern. Patients with HGD will all need to be discussed at the local multidisciplinary team meeting after consensus review and, depending on endoscopic and histopathological features, might undergo radiofrequency ablation, endoscopic mucosal resection, surgery or a combination thereof. However, patients with LGD were advised to undergo a gastroscopy every 6 months until two consecutive endoscopies demonstrated non-dysplastic Barrett's or the patient developed HGD. Several studies have demonstrated kappa values for interobserver agreement in the diagnosis of LGD as low as 0.18.20 In fact, although LGD without consensus is reported to have an incidence rate of later OAC development of 0.49%, at least one study has demonstrated that, with consensus between at least two histopathologists, the incidence rate increases to 13.4%.21 A recent randomised controlled trial has demonstrated that with consensus between expert GI pathologists, patients who undergo ablation for LGD are significantly less likely to develop adenocarcinoma and therefore the ablation of Barrett's containing confirmed LGD is now recommended.22
Can molecular biology help histopathological diagnosis? Molecular stratification
Based on the above discussion, strategies to increase the consensus around a diagnosis of LGD would be helpful. The protein product, p53 of the tumour suppressor gene TP53, which is often mutated in the progression to OAC, is now validated as an adjunct to help clarify the diagnosis of LGD. An abnormal pattern is associated with an increased risk of OAC progression in patients with BO (Fig 4). It is also a better predictor of neoplastic progression compared with the histological diagnosis of LGD and has the benefit of good interobserver agreement.23,24
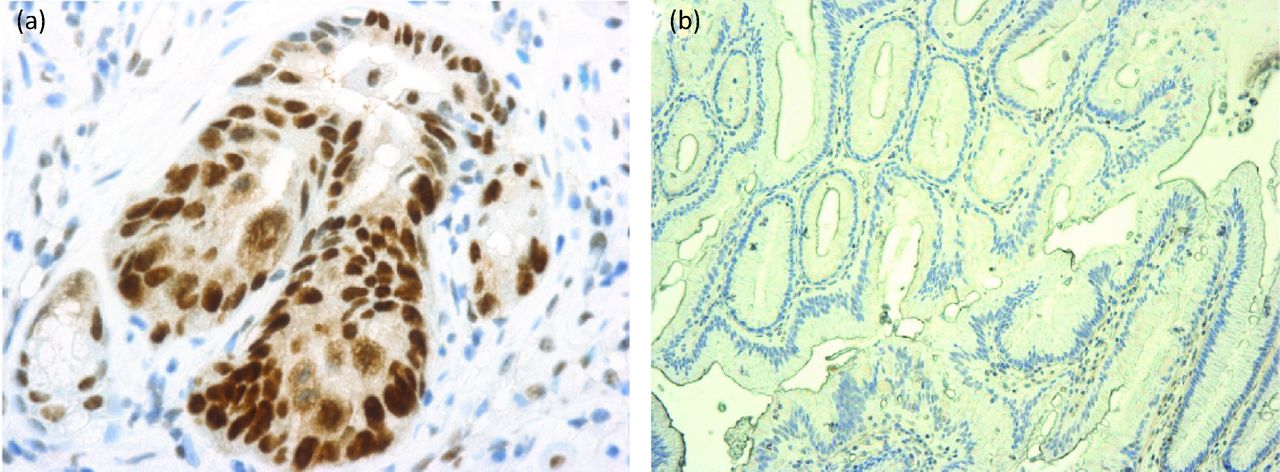
Immunohistochemistry for p53. (a) Overexpression of p53. (b) Absent p53 pattern. Both are pathological.
The future – considering population screening
Cytosponge™ for population screening
Most of the work in BO has been undertaken in patients who have already been found to have the condition and, usually, they have presented with upper GI symptoms of reflux. However, given that the population prevalence of BO is estimated to be around 2% of the total population in the western world, over 80% of patients with BO will remain undiagnosed.25,26 To reduce the incidence of OAC, it follows that we should also concentrate on diagnosing the population at risk through screening as well as risk stratifying those with diagnosed BO.
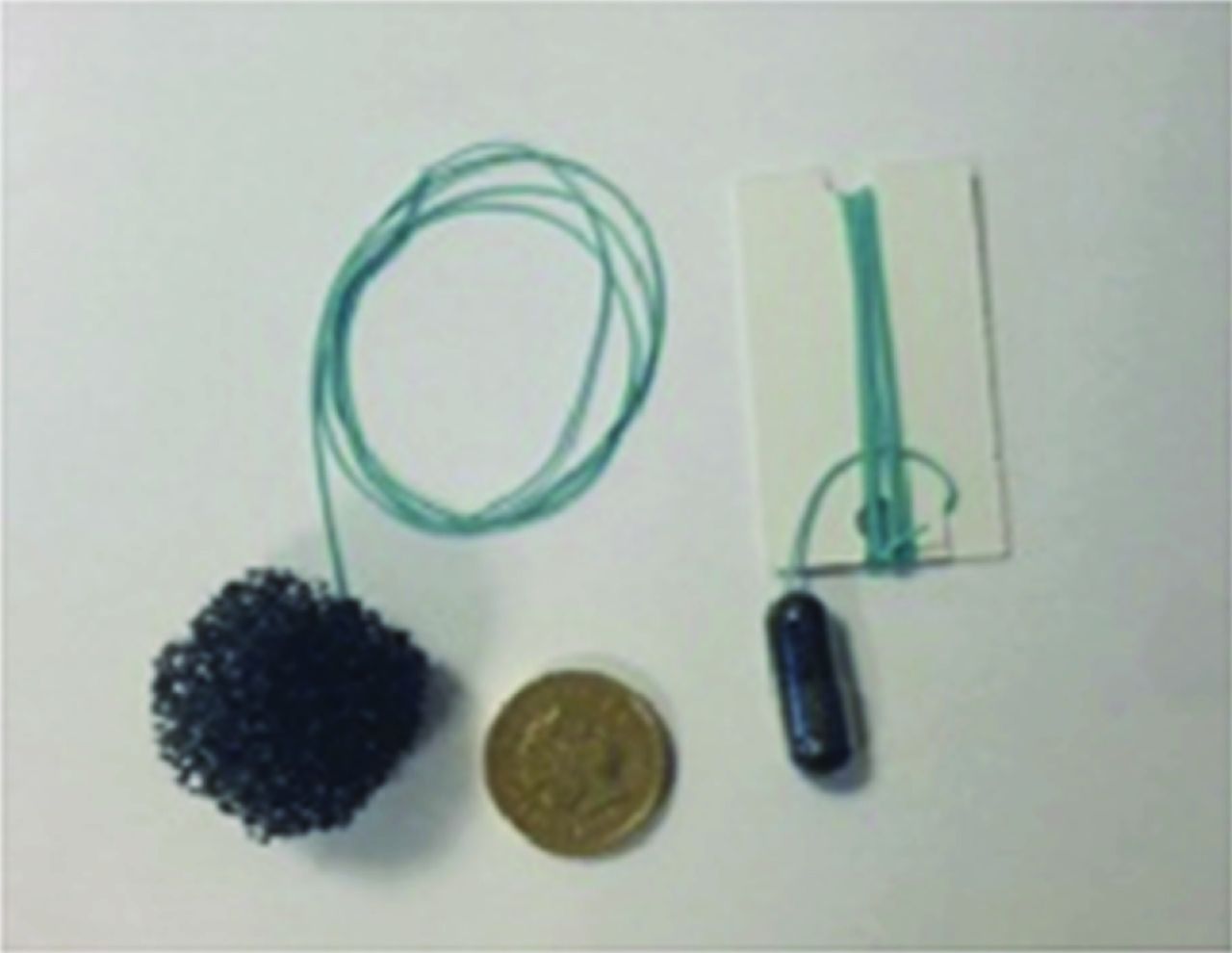
Endoscopic population screening would be unfeasible and, therefore, recent trials have assessed novel technologies for this purpose, including ultrathin transnasal endoscopy and non-endoscopic technologies, such as the Cytosponge™. The Cytosponge™ is a capsule on a string, which the patient swallows. Once in the stomach, the capsule dissolves to release a spherical sponge mesh that can then be retrieved using the string; during its retrieval, approximately 500,000 oesophageal cells accumulate within the mesh. The administration and retrieval of the Cytopsongeô takes 5 minutes and can be performed in the GP surgery. These cells can then be prepared for histological and molecular analyses with immunohistochemical analysis of a Barrett's marker, trifoil factor 3 (TFF3), proving crucial for the success of this test.
The Cytosponge™ test combined with TFF3 detection was compared with endoscopy and biopsy in a primary care cohort study of just over 500 patients.27 The sensitivity and specificity of Cytosponge™ and TFF3 detection for the detection of BO was 73.3% and 93.8%, respectively for short-segment BO (<1 cm circumferential length) and increased to 90% and 93.5%, respectively for longer segments >3 cm. This compares well with tests used in other national cancer screening programmes. A second study of over 1,000 patients is now being completed to evaluate this approach further and the results are awaited (in a Cancer Research UK-funded and National Institute of Health Research portfolio study called ‘BEST2’).
The Cytosponge™ raises the possibility of population screening for BO while uncoupling endoscopy units from the burden of carrying out what would necessarily be a large screening programme. An obvious next step is to ask whether the Cytosponge™ test could be taken further so that, once the BO has been detected, further analyses might enable patients with BO to be stratified as high or low risk for progression to OAC. This possibility will be evaluated in the recently completed BEST2 study.
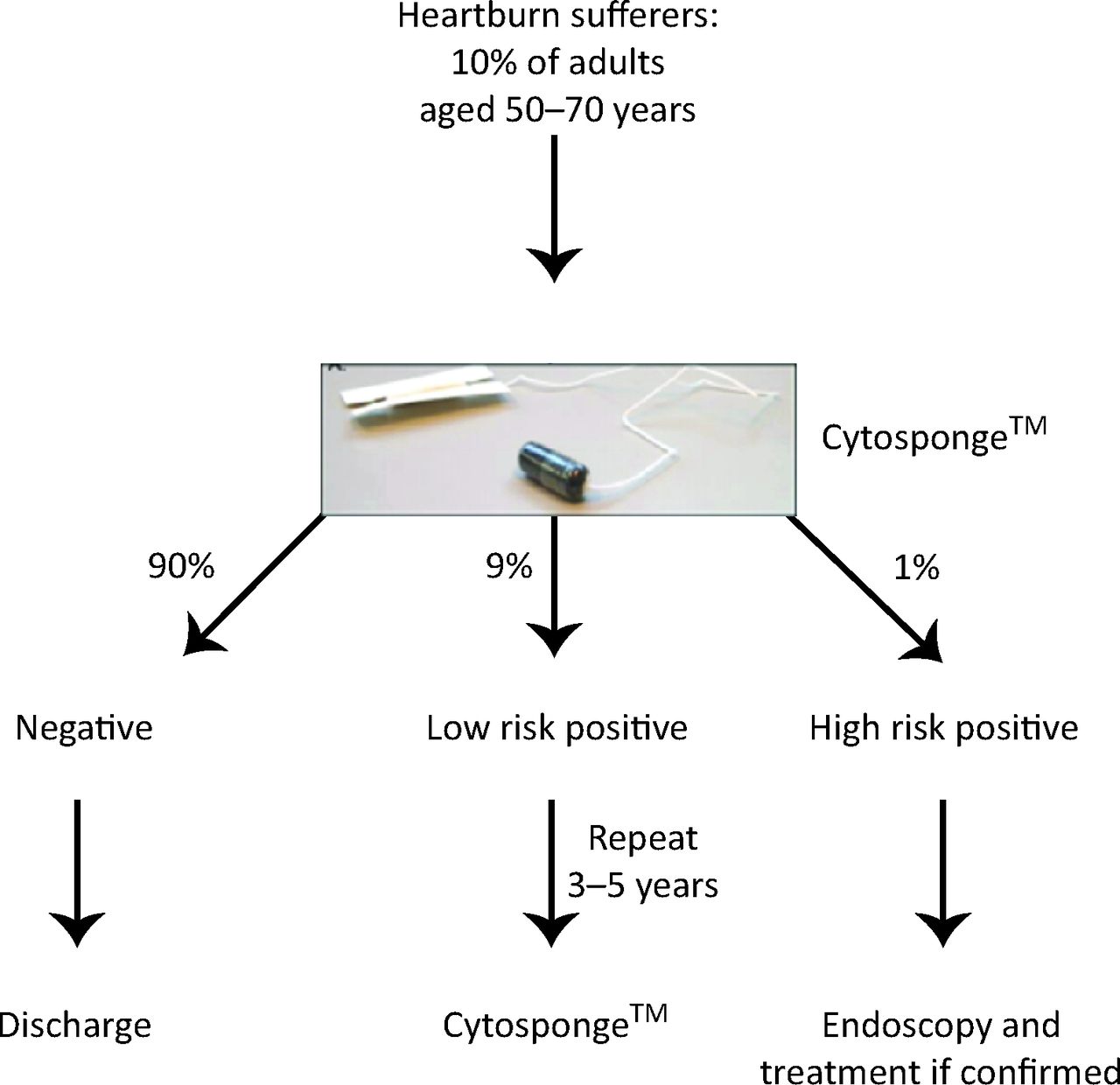
Using non-endoscopic means, such as the Cytosponge™, to both diagnose and risk stratify those with BO might not only reduce the burden on patients having to undergo endoscopic surveillance for BO, but also reduce the healthcare cost burden by reducing the overall number of endoscopies needed.28 A future paradigm is demonstrated in Fig 6, whereby symptomatic patients with heartburn would undergo Cytosponge™ assessment and, if found to contain Barrett's cells as determined by histology and TFF3, they would undergo further histological and molecular analyses to determine the risk of progression to OAC. On the basis of this stratification, patients might then be offered a further Cytosponge™ at a later date if they are low risk, or an endoscopy if there is evidence of dysplasia, to treat with the appropriate endoscopic modality.

The Cytosponge™. The Cytosponge™ is swallowed as a capsule. The soft mesh expands once in the stomach and, on withdrawal, the mesh traps a sample of oesophageal cells, which can then be analysed.
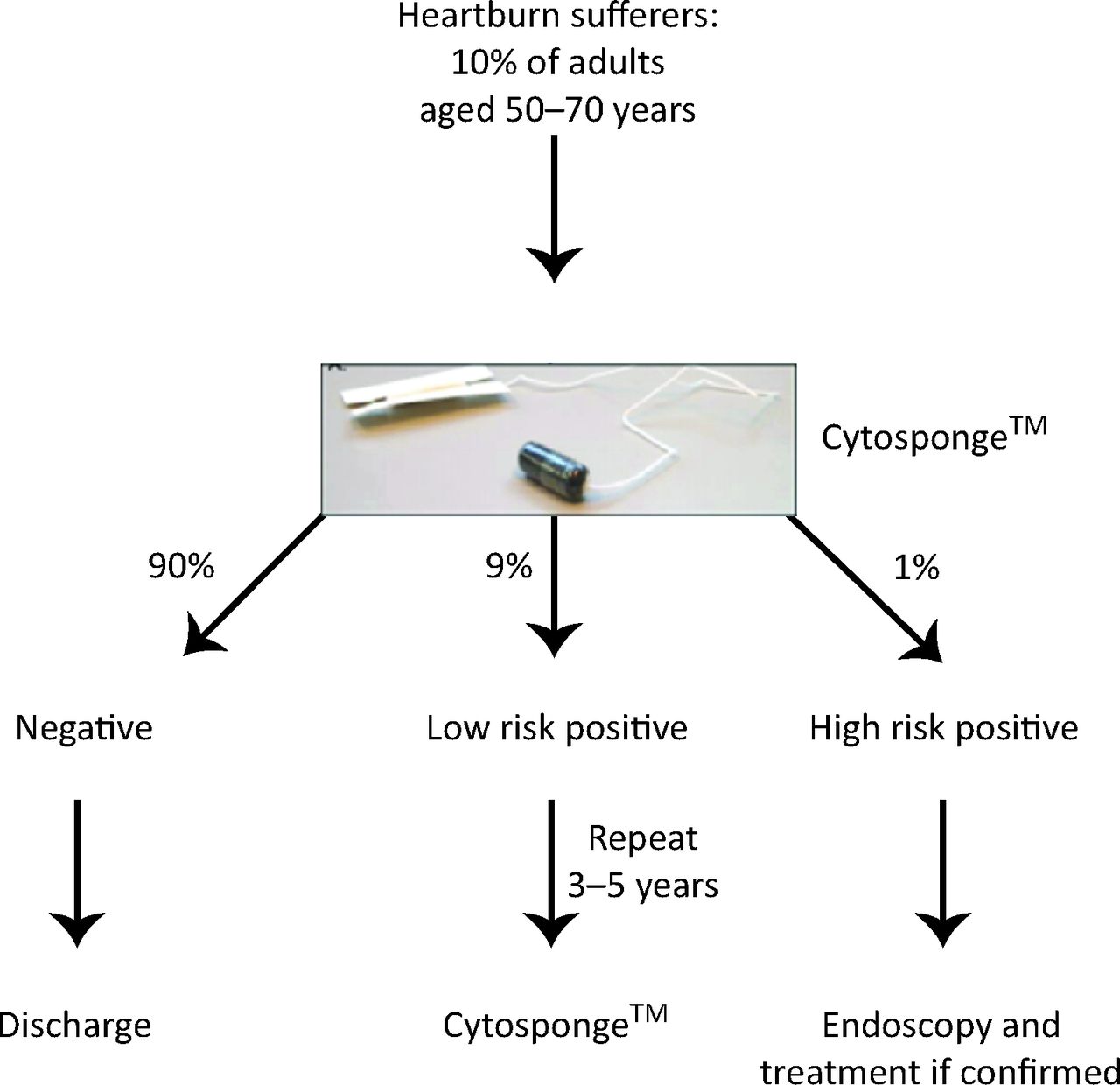
A possible future algorithm for the stratification of patients with Barrett's oesophagus using the Cytosponge™.
Although work has started to stratify patients according to clinical, histological and molecular risk, there is more work to be done. Factors, such as a patient's age or sex, body mass index or waist:hip ratio and drug intake, have all been implicated in Barrett's progression and, pending further studies, might have a part in deciding the need for surveillance. Similarly, advanced imaging techniques might enable targeted biopsy in patients who otherwise would undergo standardised sampling. Finally, genetic and molecular markers are likely to have an increasingly important role in predicting those who will progress to OAC and also in diagnosing different degrees of dysplasia.
- © 2014 Royal College of Physicians
References








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- Introduction
- Cancers take years to evolve – understanding precursor lesions and early cancers as targets
- The evidence for surveillance
- The growing emphasis on targeting the right patients for surveillance
- Clinical stratification
- The need for high-quality, high-resolution endoscopy
- Histological stratification
- Can molecular biology help histopathological diagnosis? Molecular stratification
- The future – considering population screening
- References
- Figures & Data
- Info & Metrics