
ABSTRACT
The past century has witnessed accelerated development in imaging modalities. Better anatomical visualisation and improved data analysis have improved survival rates. Through emerging functional, molecular and structural imaging modalities, better anatomical visualisation has been extended to cellular and molecular detail, improving diagnosis and management of diseases. This article reviews the advances made in emerging imaging modalities as well as their potential applications in targeted therapy.
Introduction
Since Wilhelm Röntgen's discovery of X-rays with the first radiograph of his wife's left hand in 1895,1 the development of imaging modalities has been explosive. From the first clinical computed tomography (CT) scan in 1971,2 to the three-dimensional volume rendering of images from volumetric CT scanners in 1989,3 to the first integrated positron emission tomography computed tomography (PET-CT) scan in 1998,4 imaging technologies have allowed better anatomical visualisation of the human body. The demand for imaging examination has also risen exponentially. The number of CT scans performed by NHS trusts has increased from 1.45 million in 2000–2001 to 3.72 million in 2009–2010. In 2010, NHS England owned a total of 426 CT scanners, 376 of which were installed in the last 10 years.5 Today, emerging imaging modalities that incorporate improved data analysis, functional, molecular and structural imaging, and that facilitate image-targeted therapy, are set to further transform the practice of medicine.
Improved data analysis
The use of imaging technology with improved data analysis can reduce the projected rise of cancer deaths, which is predicted to double from 7.6 million deaths in 2008 to 13.2 million deaths in 2030.6 Using a combination of epidemiological data analysis with low dose CT screening, the National Lung Screening Trial has successfully reduced lung cancer mortality.7 In total, 53,454 participants at high risk for lung cancer were randomly assigned to receive annual low-dose helical CT scan or chest radiograph screenings for three years and followed up for an additional 3.5 years. Lung cancer mortality was reduced by 20.3% in the low-dose helical CT group, compared with the chest radiograph group.
Image processing techniques such as maximum-intensity-projection (MIP) have enabled the increased detection of pulmonary nodules on CT scans.8 A study comparing the use of MIP with volume rendering (VR) image processing techniques found VR to be superior to MIP in detecting small pulmonary nodules.9 These image processing techniques have been further developed using machine learning methods to facilitate computer-aided detection of pulmonary nodules.10,11
New diagnostic algorithms have been developed using improved data analysis techniques to improve disease diagnosis and management. By incorporating imaging features, such as size and solidity of the nodules, and clinical and social data such as smoking history, a comprehensive algorithm was developed to stratify patients in the diagnosis and management of solitary pulmonary nodules.12 This has led to a more streamlined diagnostic and management pathway, thus reducing unnecessary investigations.
Functional imaging
Integrated colour perfusion imaging with CT scans has enabled the creation of a quantifiable map of regional tissue perfusion to be displayed according to a colour scale. The rate of enhancement of a region of interest is quantified through a sequence of images rapidly acquired immediately after a bolus of intravenous injection of a contrast medium. First described in 1991, its potential applications have been widespread, as the authors predicted, and has proven to be useful in studies of intrarenal blood flow, regional perfusion in tumours and studies of cerebral perfusion in patients with stroke.13 This has further informed clinical decision making by enabling the prediction of tumour behaviour and stroke recovery, as well as by stratifying benign or malignant renal tumours. For example, a study of the use of perfusion CT in rectal cancer has shown that tumours with short mean transit time (MTT) values tended to respond poorly to chemotherapy and radiation therapy.14
Functional imaging of tumours using dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) has also been used to predict tumour response to treatment. A more comprehensive visualisation of the wash-in and wash-out contrast kinetics within tumours has allowed pharmacokinetic modeling to generate a DCE-MRI biomarker, ΔKtrans. DCE-MRI has been used in early phase trials to determine a minimal effective dose of chemotherapy.15,16 In a study of women with breast cancer, ΔKtrans was shown to be able to discriminate non-responders, partial responders, and good responders to bevacizumab. These findings were corroborated by the authors’ pathological findings.17 DCE-MRI has also been shown to be accurate for detecting residual local disease following chemo-radiotherapy in patients with locally advanced breast cancer.18
MRI using hyperpolarised noble gas is emerging as a new technique to describe regional functional abnormality in the lung. The MR signal originates from hyperpolarised noble gas, which is inhaled into the lungs. The highly diffusible helium gas (3He) has been investigated in normal patients as well as in patients with lung disease such as asthma, cystic fibrosis and chronic obstructive pulmonary disease. It has also been used in patients after radiation therapy. The poor availability of 3He and its cost have led researchers to investigate an alternative noble gas, xenon (129Xe). This is a highly soluble gas which has been used in pulmonary and cerebral imaging.19 Regional ventilation and alveolar size can be quantified using the distribution and diffusion of the gas, respectively. As a small fracture of the inhaled, 129Xe is taken up by the lung parenchyma and blood. Xenon MR can distinguish the resulting signals and may lead to a new way of performing ventilation/perfusion scans by providing a real-time picture of lung function (Fig 1).20

Xe-MRI ventilation images and lung density images showing abnormal heterogenous signal throughout the lungs. Abstracted Xe-MRI ventilation maps (b and d) are mapped onto conventional MRI (a) and volumetric CT data (c) to produce 3D ventilation images (e and f). Xe-MRI = xenon magnetic resonance imaging.
Molecular imaging
The advent of PET-CT scans has enabled more detailed imaging of the body at a molecular and cellular level. PET-CT scans with a radioactive tracer 18-flurodeoxyglucose (18FDG) allow the quantification of metabolically active cells in a colour-encoded map. The use of PET-CT scans in pre-operative assessment of patients with suspected non-small-cell lung cancer has improved the differentiation of benign and malignant pulmonary nodules and the detection of distant metastasis, leading to a 50% reduction in futile thoracotomies in patients.21 The use of PET-CT scans in a randomised controlled trial also improved the overall survival of patients with early lung cancer (hazard ratio, 0.88; confidence interval, 0.61–1.29).22
New PET-CT tracers are also under development. Choline-based 18F-labelled tracers have been shown to be useful in distinguishing malignant and normal cerebral tissue and in detecting local recurrence of prostate cancer.23 PET-CT 18F-Fluoride scan is also the most sensitive and specific for detecting bone metastases in patients with prostate cancer.24
Liver imaging with a novel non-invasive MR method allows the rapid characterisation of liver tissue, including the quantification of hepatic iron and fat content, as well as the identification and staging of inflammation and fibrosis. The high corroboration with pathological findings suggests that this method could potentially replace liver biopsy for many indications.25
The first trial of metabolic imaging using dynamic nuclear polarisation of [1-13C]pyruvate in humans has shown that it is safe and useful in non-invasively characterising changes in tumour metabolism in patients with prostate cancer. Regions of biopsy-proven cancer were found to have elevated levels of the hyperpolarised tracer.26
Combined functional and molecular imaging
Trials investigating the combined use of functional and molecular imaging to better visualise regions of active angiogenesis are underway. PET-CT scans with 18F-FDG uptake and tumour perfusion parameters from perfusion CT scans such as blood flow, blood volume and Ktrans have both been shown to correlate with tumour biomarkers such as Ki67 and microvessel density, respectively.27 As such, the combined use of functional and molecular imaging can provide complementary data to improve tumour profiling.
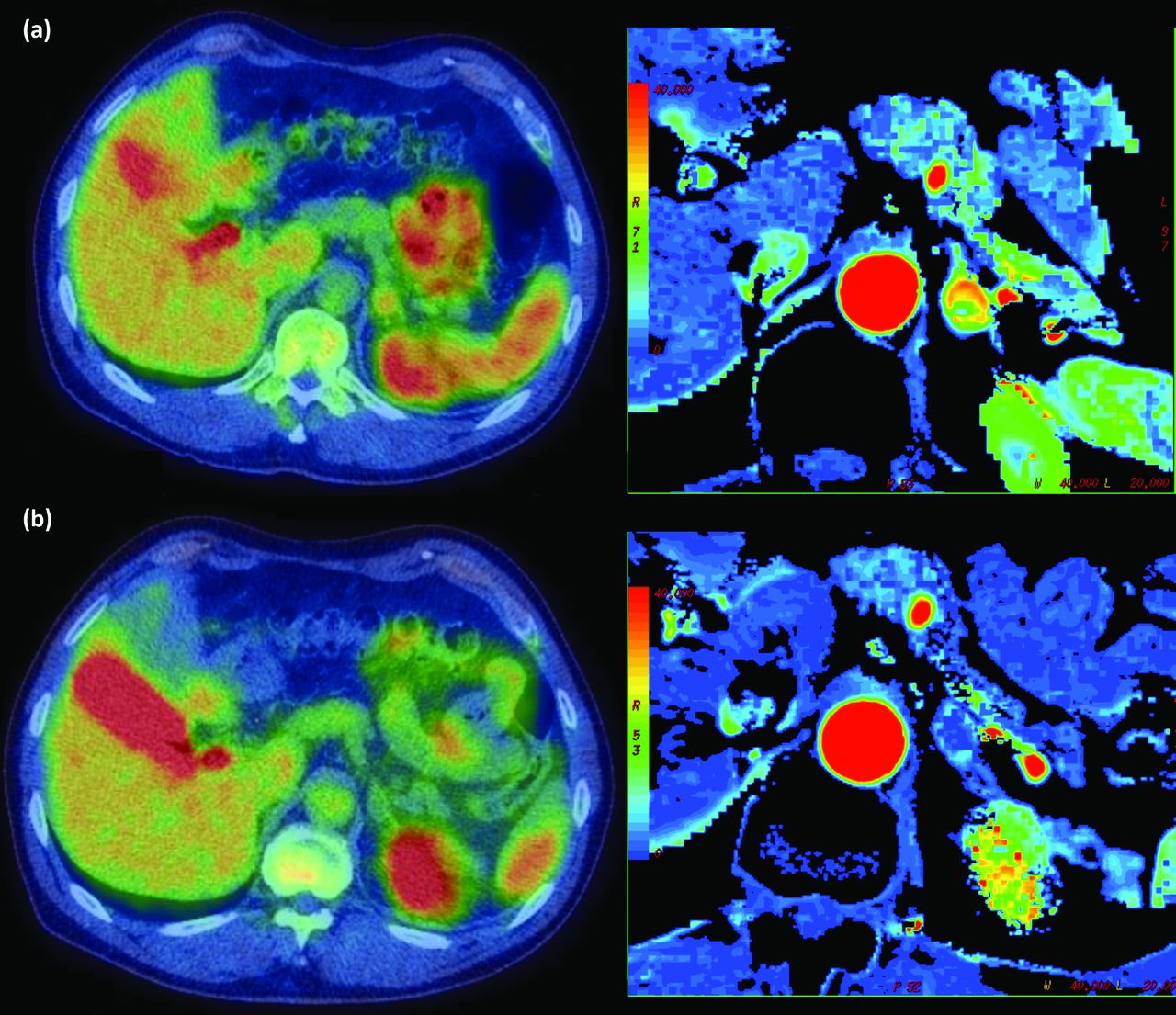
A new PET tracer, fluciclatide, is a small peptide containing the Arg-Gly-Asp (RGD) tripeptide that has been shown to have high affinity for integrin αvβ3 receptors, which are upregulated in metastatic tumour cells and in angiogenesis. It is being investigated in combination with perfusion CT scans to quantify tumour response to anti-angiogenic agent sunitinib in patients with metastatic renal cell cancer in Oxford (NCT01492192; Fig 2).

Axial slices showing PET-CT (left) and perfusion CT (right) images of an adrenal metastasis before (above) and after (after) treatment with an anti-angiogenic agent. PET-CT = positron emission tomography-computed tomography.
Structural imaging
MRI diffusion-weighted imaging allows the visualisation and quantification of the diffusivity of water molecules within tissue, which may be altered by restricting barriers owing to pathologic processes. This imaging technology therefore allows the histopathological appearances of the tissue to be visualised non-invasively. A study comparing the appearances of colorectal hepatic metastases on diffusion-weighted MRI with histopathology revealed that colorectal liver metastases with high signal rim intensity on imaging correlate with central necrosis on tissue sections.28
A trial comparing PET, conventional contrast-enhanced CT, perfusion CT and diffusion-weighted imaging (DWI) MRI with outcome, histological markers of angiogenesis and genomic analysis in colorectal hepatic metastasis, is due to recruit in Oxford (Fig 3).

Axial images of (clockwise from top left) PET-CT, perfusion CT, DWI MRI and conventional contrast–enhanced CT images of a patient with a hepatic metastasis from colorectal cancer. DWI MRI = diffusion-weighted imaging magnetic resonance imaging; PET-CT = positron emission tomography-computed tomography.
Image post-processing of ultrasound images has also enabled better structural imaging. For example, the intensity of the reflected B-mode ultrasound signal is correlated with lipid content of carotid artery plaques, which may be associated with intraplaque haemorrhage.29 Nakagami parametric imaging, which is based on the distribution of back-scattered radiofrequency echoes, has been used to measure the degree of change in tissue caused by ultrasound-induced thermal exposures.30 In addition, the use of power Doppler and contrast-enhanced ultrasound can allow the visualisation of the vascularity and perfusion characteristics of a lesion in vivo, respectively. Acoustic radiation force impulse (ARFI) elastography has been shown to be a reliable method in assessing tissue stiffness and therefore liver fibrosis.31
Therapies using modern imaging technologies
In addition to image-guided ablative techniques, such as radiofrequency or microwave ablation, high intensity focused ultrasound (HIFU) is a promising new local image-guided treatment. HIFU can generate mild hyperthermia at intensities lower than those required for ablation, resulting in less adverse events from hyperthermia compared with the current ablative treatments. Celsion and the University of Oxford will shortly begin recruiting for the first human trial of the targeted delivery of chemotherapy. In this study, doxorubicin will be delivered intravenously, covered in a liposomal heat sensitive shell that will allow drug release when heated using HIFU. This would enable targeted delivery of the chemotherapy within the lesion of interest as well as reduced systemic administration of chemotherapy and its adverse effects.32
Conclusion
The exponential development and demand for imaging examinations has led to the development of emerging imaging modalities. These imaging modalities have the potential to add to our structural, molecular and functional understanding of pathological processes in addition to providing novel ways to deliver targeted therapy. The results of ongoing and future trials in these emerging modalities will transform our current clinical pathways and are keenly awaited.
- © 2014 Royal College of Physicians
References








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.