
ABSTRACT
Dengue is one of the most rapidly emerging viral infections globally, with 2.5 billion people now thought to live in dengue-endemic areas. In addition, reports of travel-related and autochthonous infections are increasing in non-endemic areas. Most patients with dengue experience a self-limiting febrile illness, but a proportion develop potentially life threatening complications around the time of fever clearance, including plasma leakage occasionally leading to shock, bleeding, and organ impairment. As dengue can present with non-specific symptoms of fever, headache and myalgias, the potential for misdiagnosis and inappropriate management by medical staff inexperienced with the disease is a concern. This short review will outline the latest World Health Organisation disease classification, potential complications, clinical assessment and management for clinicians working in non-endemic areas.
Key points
Dengue is emerging as the most abundant vector-borne viral illness in the world.
Travel-related and autochthonous infections are increasing in non-endemic areas.
Dengue can present with non-specific symptoms of fever, headache and myalgias and the potential for misdiagnosis and inappropriate management by medical staff unfamiliar with the disease is a cause for concern.
Most patients with dengue experience a self-limiting febrile illness but a proportion develop potentially life-threatening complications around the time of fever clearance, including plasma leakage occasionally leading to shock, bleeding and organ impairment.
Management currently relies on symptomatic and supportive treatment in the form of meticulous fluid balance for those identified to have significant plasma leakage.
Dengue is the most abundant vector-borne viral disease in the world. In the last 20 years the burden of disease has increased four-fold and 2.5 billion people are now thought to live in dengue-endemic areas. Latest estimates suggest there are around 100 million symptomatic dengue infections annually.1 South-East Asia has a particularly high disease burden, although in the last two decades Latin America and the Caribbean have also seen considerable expansion in case numbers. More recently, outbreaks have been reported from several African countries.2,3
Dengue can be caused by any one of four viral serotypes (dengue virus (DENV) 1–4), and is transmitted by day-biting urban-adapted Aedes mosquito species.4 After an incubation period of 4–14 days, symptomatic patients typically experience a self-limiting febrile illness with one or more of the following symptoms:
high fever of up to 40˚C
headache
retro-orbital pain
nausea/vomiting
myalgia
arthralgia
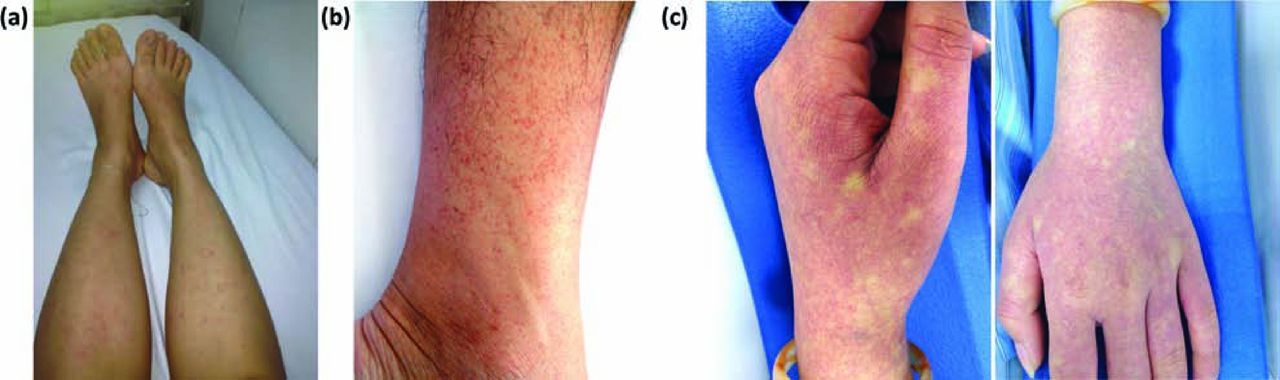
rashes (Fig 1).

Spectrum of dengue associated rashes. (a) Macular-papular rash may be seen during the febrile phase; (b) petechial rash may develop during the febrile/critical phase particularly on arms and legs; (c) erythematous rash with ‘islands of white’ can be widespread and develop during the recovery phase.
This febrile phase lasts for 4–7 days, and once the temperature settles most patients recover without complications.5 Crucially however, a small number of individuals go on to develop potentially serious complications during the 48 hours around defervescence (the critical phase) including plasma leakage, sometimes severe enough to cause hypovolaemic shock; coagulation derangements, sometimes associated with haemorrhage; and organ impairment (usually secondary to severe leakage and/or bleeding).6 With careful management the outcome is generally good and convalescence is typically short and uneventful, although it may be prolonged in adults with profound tiredness, aesthenia and depression persisting for weeks to months after recovery.7
The World Health Organisation (WHO) classification of dengue was updated in 2009,6 replacing the original dengue fever/dengue haemorrhagic fever grading, and now comprises the following entities:
Box 1. Warning signs.

Box 2. Criteria for severe dengue.
Development of severe dengue is strongly associated with secondary heterotypic DENV infections rather than primary infections.8 Age also has a strong influence on the clinical phenotype, with severe plasma leakage more likely to occur in children, while major bleeding is usually seen in adults.9
Dengue in non-endemic areas
Changing mosquito ecology, globalisation of trade and a remarkable increase in the volume of air travel have all influenced dengue epidemiology. Reports of travellers acquiring dengue are increasing, as are reports of autochthonous cases presenting in non-endemic areas where the mosquito vectors have become newly established.10 Surveillance data indicate that dengue is now the most common cause for fever in travellers returning from all geographical regions except sub-Saharan Africa and Central America, where malaria remains the most common cause.11,12 Travellers returning to Europe usually acquire dengue from South-East Asia, particularly Thailand,13 while in the USA the highest rates followed travel to Dominican Republic and Mexico.14 Autochthonous spread has been reported from the south of France and Croatia, and in 2012 the first European dengue outbreak since the 1920's occurred in Madeira, resulting in over 2,000 cases and 120 hospitalisations.15
Although most patients with travel-associated dengue have primary infections and thus are unlikely to develop severe disease, one study from Europe showed 11% of the 219 dengue infections reported between 2003–5 had complications, including internal haemorrhage, plasma leakage and shock.16 Recent reports of fatalities in Germany and Norway have highlighted the potential for misdiagnosis and inappropriate management by staff unfamiliar with the disease.17,18
Clinical assessment and laboratory diagnosis
In the early febrile phase dengue presents with clinical features similar to malaria and a wide variety of bacterial and viral infections.6 A detailed travel history is important, focused on timing and duration of stay in endemic areas, dengue seasonality and epidemic activity in the places visited, and predominant urban or rural stay.19 Simple laboratory investigations may help distinguish dengue from other infections, but are not definitive. Thrombocytopenia occurs almost universally, with a nadir around defervescence, and can help differentiate dengue from infections like influenza, measles and rubella. Leucopenia and a mild transaminitis are also seen, but other laboratory parameters are generally unaffected unless complications develop. Table 1 briefly summarises the clinical features and investigations to consider during each disease phase.
Assessment of suspected dengue patients during each disease phase.
In the first week of illness, laboratory confirmation relies on identification of viral RNA using reverse transcription polymerase chain reaction (RT-PCR), or detection of dengue non-structural protein 1 (NS1) using enzyme-linked immunosorbent assay (ELISA).22,23 However, the viraemia is short so serodiagnostic tests (typically IgM Capture ELISA) are used from the end of the first week onwards, ideally with demonstration of seroconversion on paired samples. Rapid tests, often combining NS1 detection with an antibody test, are also available and have a reasonable window of detection.24
Management
A number of warning signs (Box 1) may occur during the transition into the critical phase. Of note, abdominal pain can be severe, and there are reports of surgery being performed for suspected acute abdomen before dengue was diagnosed.17,25 Symptomatic relief and regular outpatient review are usually sufficient in the absence of warning signs. Other high-risk groups include children and the elderly, pregnant women, and individuals with comorbidities (eg diabetes, hypertension or obesity).26,27 These patients should be seen at least once daily or admitted for close observation.
No specific antivirals or adjunctive therapies have shown benefit, so management relies on symptomatic and supportive treatment.28,29 This involves meticulous fluid balance and cautious intravenous fluid replacement for patients unable to tolerate oral fluids and those identified to have significant plasma leakage. The minimum volume of parenteral fluid should be given to achieve adequate organ perfusion while avoiding the well-recognised complication of fluid overload. Oral paracetamol can be given but NSAIDs should be avoided due to the risk of gastrointestinal bleeding. Specific management for patients who develop severe dengue is out of the scope of this article and the WHO guidelines should be consulted.6
Conclusion
Dengue is one of the most rapidly emerging viral infections in the world, and as it continues to spread across the globe, travel-related infections are likely to increase. As climate change and globalisation facilitate the establishment of competent vectors in non-endemic areas, local transmission could also become more frequent. Awareness of dengue, the potential complications, and the essential principles of management is important for frontline healthcare personnel everywhere to avoid unnecessary morbidity and mortality.
- © 2015 Royal College of Physicians








{kind=link}