
ABSTRACT
This paper describes a new tool called ‘Day-of-Care Survey’, developed to assess inpatient delays in acute hospitals. Using literature review, iterative testing and feedback from professional groups, a national multidisciplinary team developed the survey criteria and methodology. Review teams working in pairs visited wards and used case records and bedside charts to assess the patient's status against severity of illness and service intensity criteria. Patients who did not meet the survey criteria for acute care were identified and delays were categorised. From March 2012 to December 2013, nine acute hospitals across Scotland, Australia and England were surveyed. A total of 3,846 adult general inpatient beds (excluding intensive care and maternity) were reviewed. There were 145 empty beds at the time of surveys across the nine sites, with 270 definite discharges planned on the day of the survey. The total number of patients not meeting criteria for acute care was 798/3,431 (23%, range 18−28%). Six factors accounted for 61% (490/798) of the reasons why patients not meeting acute care criteria remained in hospital. This survey gives important insights into the challenges of managing inpatient flow using system level information as a method to target interventions designed to address delay.
Introduction
Ensuring emergency access to acute health services is a challenge for many countries. Emergency access efficiency is commonly measured through emergency department overcrowding statistics. International evidence suggests that lack of timely access to inpatient beds is one of the main reasons for emergency department overcrowding: this problem has been termed ‘access block’.
Timely emergency access is commonly considered a managerial rather than a clinical issue, but retrospective analysis of emergency department attendance and admissions in recent years has shown that overcrowding is associated with increased risk of readmission and mortality.1,2 While causal relationships have yet to be established, reducing access block is clearly not only an imperative for managers but also for clinicians.
Addressing access block requires improvements in systems and processes across the continuum of care to ensure patients receive timely clinical treatment from appropriate teams in the correct location. Improving inpatient flow is part of this continuum and dependent upon action at many levels within acute, community and social care sectors.
Objective data to inform hospital operational teams dealing with patient flow is an important part of this process. The aim was to develop an easy, reliable and consistent method to assess acute hospital inpatients that would identify those no longer likely to benefit from acute hospital care, and to determine the reasons why patients remain in hospital after the purpose of the acute admission has been achieved.
Literature review
On review of the literature, the appropriateness evaluation protocol (AEP) developed by Gertman and Restuccia in 1981 was identified as a ‘technique for assessing unnecessary days of hospital care’.3 This provides objective criteria-based assessment of the clinical appropriateness of admissions to hospital and subsequent days of care.
In the literature, the AEP criteria have been applied at a single point in time, such as a single day, or used multiple times on sequential days with the same patients.4–6 The criteria have also been shown to reliably identify acuity of medical illness and, in one study, the presence of positive AEP criteria reflected increased morbidity and mortality.5
Since 1981, the AEP criteria have been used, or modified for local use, in Italy,6 France,7 Belgium,8 Holland,9 Spain,10,11 Germany,12 Denmark5 and Turkey.13,14 Assessments in the UK include the 1997 national study of acute medical admissions conducted by the Royal College of Physicians of London,4 which reviewed 4,885 days of hospital care against the AEP criteria. In this study, 45% were judged ‘inappropriate’, most commonly because of patients remaining in hospital after the medical purpose of hospitalisation had been accomplished.
Methodology
To deepen understanding of delays in unscheduled inpatient emergency access, a national multidisciplinary working group was established. This group reviewed the relevant literature and developed criteria and methodology for use (initially) in NHS Scotland. The working group reviewed the AEP and found it to be useful but needed updating to reflect contemporary inpatient care. A variety of methods was used to update the criteria, including collecting expert opinion and testing and receiving feedback from a range of professional groups, including doctors, nurses, allied health professionals, managers and social care colleagues. This resulted in the development of a set of criteria with 12 ‘severity of illness’ variables, covering derangements in physiological parameters, and 16 ‘service intensity’ variables, reflecting levels of clinical interventions, prescribed treatments and clinical characteristics according to history (see supplementary material online for list of criteria).
The criteria and methodology were developed though iterative testing in four hospitals. This included feedback sessions at the sites surveyed followed by review by the national group. The criteria were further assessed by reviewing 89 consecutive patients admitted to an acute hospital and measuring them against the criteria on a daily basis until discharge. The adaptations to the criteria were tested prospectively.
In addition to the acute care criteria we developed a list of ‘reasons not discharged’ for patients not meeting the revised criteria. This was aligned to Scotland's national delayed-discharge codes, providing 19 reasons reflecting acute and community/social care services. Examples include ‘awaiting social work assessment’, ‘awaiting community hospital bed’ and ‘awaiting consultant decision/review’.
We identified research in Spain11 which had demonstrated that location of patients outside of the relevant specialty unit (usually known as ‘outliers’ or ‘boarders’) had a significant association with a higher incidence of inappropriate stay. Testing of the criteria in Scotland revealed a similar pattern, with outlying/boarding patients often not meeting the criteria for acute care. This element was therefore added to the data collection method.
Only one criterion for acute care needs to be satisfied for the day of care to be deemed ‘appropriate’: patients who do not meet a single criterion are deemed ‘inappropriate’. Survey teams have the option of overriding the protocol in either direction if the objective criteria appear to give a result that is clinically counterintuitive.
Having developed and tested the criteria and methodology for completing the survey, we provided guidance, documentation, on-site support and data analysis for the local teams who conducted individual hospital surveys.
Results
The Day-of-Care Survey (DoCS) was used between March 2012 and December 2013 to survey 3,846 acute hospital beds in nine hospitals internationally (these included district general hospitals and tertiary hospitals in the UK and Australia). All adult general inpatients at each site (excluding intensive care, obstetric and mental health units) were reviewed using the DoCS criteria set. Patients were defined as inpatients if they had been accepted for admission and waiting in the emergency department for more than four hours. Unfunded/surge capacity beds were included in the numerator, but not the denominator. Each hospital review took 1−2 hours to complete and data were made available the same day.
The total number of patients across the nine hospitals was 3,701, with bed occupancy at the individual hospitals ranging from 85–104% at the time of survey. Each survey commenced at 8 am and was completed within a two-hour period. Patients identified for definite discharge on the day of the survey totalled 270 across the nine hospitals and were excluded from further analysis. A total of 798 patients out of the total of 3,431 (23%, range 18–28%) did not meet acute care criteria (Table 1).
Hospitals surveyed, date of surveys, total patients surveyed and those not meeting Day-of-Care Survey criteria (numbers and percentage).
For patients not meeting DoCS criteria, the reviewer selected the primary reason the patient had not yet been discharged from the list provided. This usually required discussion with the ward manager or medical team. A breakdown of ‘reasons not discharged’, split by in-hospital/out-of-hospital for all patients not meeting the criteria, is shown in Table 2.
Top three reasons patients were not discharged split by in-hospital/out-of-hospital, for all patients not meeting the Day-of-Care Survey criteria.
The top three in-hospital reasons for not being discharged accounted for 32% of total delays, and the top three out-of-hospital reasons accounted for 28% of delays. All other specified reasons accounted for the 22% of the total with 18% not categorised, but individual reasons were identified in the narrative.
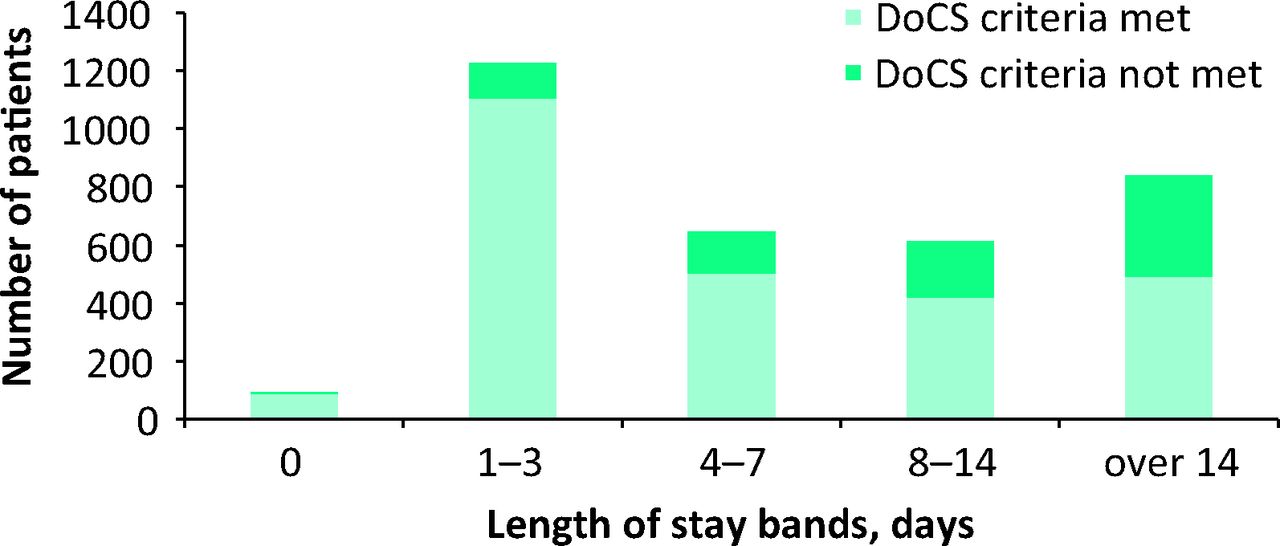
Over half the patients included in the surveys were over 70 years of age. As Fig 1 shows, the proportion of patients not meeting the criteria rose with age. There was also a consistent finding across all sites and countries surveyed that the proportion of patients who did not meet the DoCS criteria increased with length of stay (Fig 2).
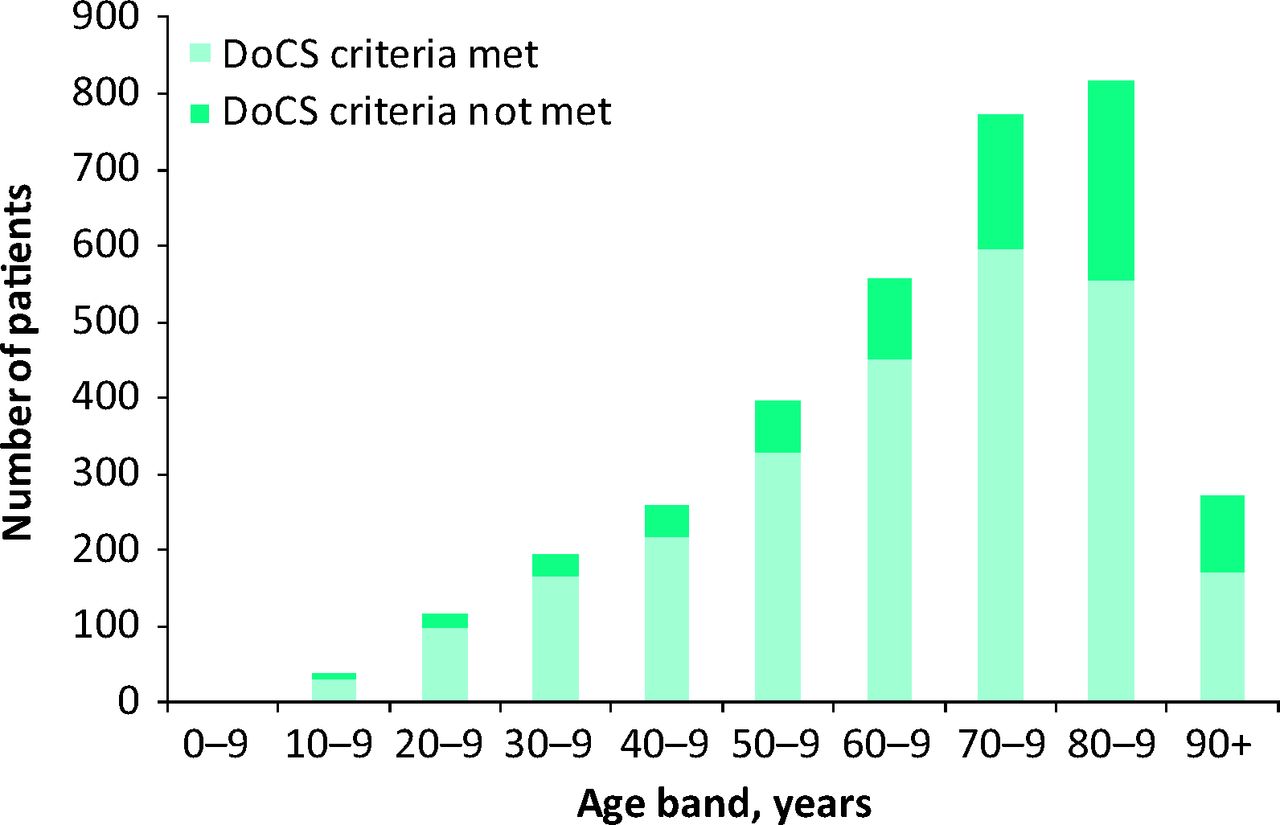
Age profile of patients who met and did not meet the DoCS criteria, excluding patients discharged on the survey day. DoCS = Day-of-Care Survey.
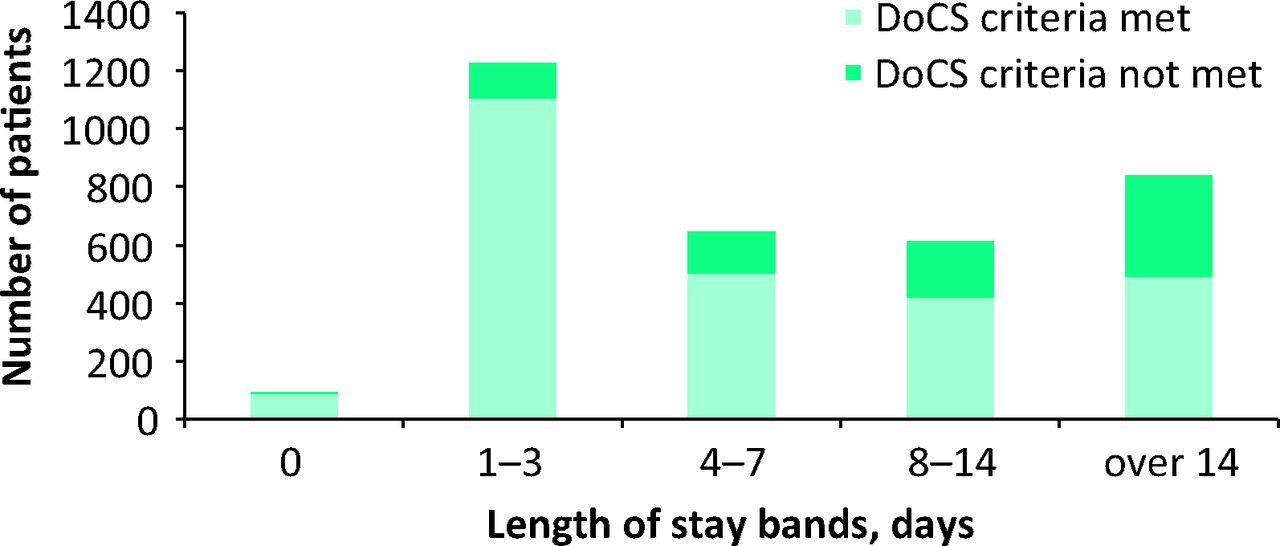
Length of stay for all patients who met and did not meet the DoCS criteria, excluding patients discharged on the survey day. DoCS = Day-of-Care Survey.
Surveying using the DoCS criteria is a simple, reproducible process that can be conducted by a combination of clinicians and personnel who are not necessarily directly involved in frontline acute care (non-health care professionals such as social workers and managers). Preparation of staff involved in the survey is crucial, but a 15-minute briefing on the afternoon prior to the survey is sufficient. The survey process itself is not lengthy, taking up to one hour per ward of 30 beds.
The overall proportion of patients not meeting the criteria (23%, n = 798) is less than the 36% reported in Australia by Dempsey,15 but not as low as the 7% found in a study of 2,180 hospital days in France,7 although the latter excluded patients who stayed less than one day.
Many published studies using the AEP document reasons for patients remaining in hospital despite not meeting survey criteria. These vary, possibly reflecting the different international models of health and social care. For example in a study from Belgium,8 the most frequent reasons were ‘waiting for an examination (investigation)’ (22%) and ‘lack of extra-hospital structures’ (31%). A French study7 stated non-availability of ‘outside’ care or resources accounted for 61% of the reasons for inappropriate stays in medical units and 83% of surgical stays (68% overall).
Our survey found six of the top-10 reasons for non-discharge were influenced by factors outside the acute hospital (lack of community hospital bed, for instance), but four were hospital-related (awaiting allied health professional assessment or consultant decision and review, for example). This reinforces the understanding that delays to discharge are not exclusively related to factors external to the hospital (as is often assumed), but indicate delays within hospital systems that need to be addressed.
The AEP was found to be useful in older patients, with high reliability and moderate validity.16 Our DoCS showed that the older patients were, the less likely they were to meet the criteria for acute care. When inpatients were grouped in 10-year age bands, it was found consistently that advancing age was associated with an increasing proportion not meeting the criteria (Fig 1). This possibly reflects not only the complex health and community needs of older people, but also their increased vulnerability to hospital admission due to comorbidities. A study in Italy17 showed that while comorbidity increased the likelihood of an appropriate admission in young patients, the converse was true for older people.
Length of stay was also found to be an important factor, with the proportion of patients not meeting a criterion increasing with length of stay (Fig 2). Many patients with stays in hospital of greater than 14 days were outliers/boarders or in unfunded capacity (such as that used to accommodate increased admissions over the winter); as in the study of Soria-Aledo et al,11 which found that outlying/boarding was significantly associated with inappropriate stay (29.7% for outliers/boarders vs 21.8% for non-outliers/boarders), these patients were less likely to meet the criteria. Patients being cared for outside their specialty area and those in hospital due to a surge-capacity response require a focused, multidisciplinary, proactive case management approach to ensure their needs for acute hospital care are met appropriately.
Discussion
The DoCS provides a snapshot of hospitals’ inpatient status at a particular point in time that enables organisations to identify the sources of delay in inpatient flows and take appropriate action. Experience to date has shown that the DoCS method:
offers a simple, easily understandable approach that involves little preparation for staff and can be carried out over short time periods with minimum disruption to clinical services
provides immediate access to core data, such as age spread of the hospital population and length of stay
creates useful insights, such as recognition that patients who have been in hospital for 14 days have a higher chance of not meeting the DoCS criteria, and that criteria are less likely to be met with increasing patient age
presents opportunities to improve patient flows by identifying sites of delays and supporting the development of solutions
creates local ownership of data and, subsequently, solutions.
DoCS have now been undertaken in acute hospitals of differing size and character in Scotland, England and Australia. Expertise to support future iterations is developing at hospital level and understanding of the reasons for delays to inpatient flows is increasing locally and nationally. The hospitals are now planning to embark on an iterative process of regular surveys to inform patient-flow management and care co-ordination.
Acknowledgements
The authors would like to thank the members of the Short Life Working Group: Karen Anderson, Gordon Birnie, Jillian Galloway, Anne Hendry, Jim Hutton, Michael Kelly, Gillian McCready, Johanne Simpson and Clare Smith, who each made significant contributions to the survey criteria and methodology; and the hospitals who participated in the survey. Dr Restuccia offered helpful comments during the development phase. TW is supported by an Improvement Science Fellowship with the Health Foundation and the National Institute for Health Research (NIHR) under the Collaborations for Leadership in Applied Health Research and Care programme for north-west London. The views expressed in this publication are those of the author(s) and not necessarily those of the Health Foundation, the NHS, the NIHR or the Department of Health.
- © 2015 Royal College of Physicians








{kind=link}
{kind=link}