
ABSTRACT
The National Institute for Health and Care Excellence (NICE) CG95 clinical guideline on chest pain of recent onset was published in 2010. There is debate over whether the proposed strategy improves patient care and its implications on service costs. Following a six-month pilot, 472 consecutive patient records were audited for pre-test probability of significant coronary artery disease, investigations performed and outcomes. Low- and moderate-risk patients had an unexpectedly low rate of coronary disease and revascularisation. Computerised tomography coronary angiography (CTCA) and stress echocardiography performed similarly, though the latter was more resource intensive. High-/very high-risk patients frequently required revascularisation and greater than 10% of each group had prognostically significant disease, going against the recommendation that very high risk patients do not undergo angiography. There were frequent protocol deviations and training clinic staff in the new approach was challenging. In conclusion, implementing NICE CG95 is feasible but presents challenges. Staff require training to follow the protocol consistently. Functional testing had no benefits over anatomical testing with CTCA, which may allow cost savings in some departments.
Background
National Institute for Health and Care Excellence (NICE) clinical guideline CG95 was published in March 20101 to usher in changes to the assessment of new onset stable angina. Rapid access chest pain clinics (RACPCs) were introduced in the early 2000s in response to national standards (the National Service Framework for coronary heart disease, published 20002), which required assessment of patients referred from primary care within two weeks. CPCs are usually nurse led and use a combination of clinical assessment and exercise tolerance testing (ETT) to risk stratify patients in order to guide further testing and management. This strategy has proved efficient in processing the large number of referrals made but there is concern over the lack of specificity and sensitivity of this approach, particularly in certain patient groups. The new clinical guideline replaced ETT with a panel of investigations from computerised tomography (CT) calcium scoring/CT coronary angiography (CTCA), to functional tests (nuclear imaging, stress echocardiography and stress or perfusion magnetic resonance imaging (MRI)) and invasive CA. The investigation chosen is determined by a risk score based on symptoms, age, gender and cardiovascular risk factors, utilising the work of Pryor3 to generate a pre-test probability of significant coronary artery disease (CAD).
On introduction of the guideline, there was concern over the markedly decreased role for exercise stress testing, and also over the assumption of equivalence in cost and efficacy of multiple functional tests. Further controversial recommendations include: 1) all patients with a high risk of CAD need invasive testing, as some may have angina which will be well controlled by medication; 2) those with a very high predicted risk of CAD can be safely treated as if they have confirmed CAD without the need for angiography, potentially missing patients with severe patterns of CAD in whom revascularisation would offer a mortality benefit (‘prognostically significant disease’). The guidelines have been implemented to a variable extent in UK hospitals, and full compliance with the schema is rare. Factors that were identified as preventing implementation in a 2010 survey of 96 RACPCs in 22 networks include lack of equipment and trained staff.4 It is generally predicted that there would be a significant increase in costs; this has been variously predicted at 24%5 and 42–43%6 in two separate London trusts. One study predicted no increase in overall short-term costs as patients underwent fewer investigations.7 To our knowledge, no real-world experience of implementing the guideline has yet been published.
Methods
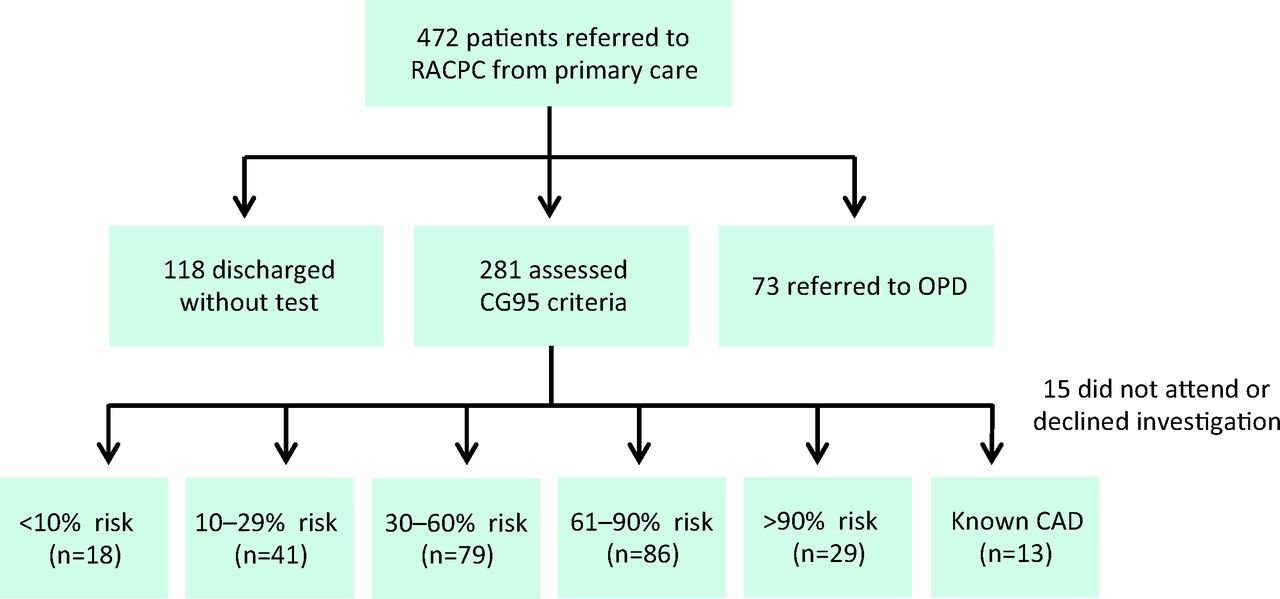
The audit was a retrospective review of 472 consecutive case records from 9 November 2012 to 26 March 2013 (168 days). The audit was registered with Great Western Hospital NHS Foundation Trust. Consecutive patients were referred to the RACPC by primary care over a six-month period (Fig 1). These patients were assessed by senior specialist nurses according to the NICE clinical guideline CG95 and, where indicated, referred for further testing (Table 1). As defined in the guideline, significant CAD found during invasive CA is ≥70% diameter stenosis of at least one major epicardial artery segment or ≥50% diameter stenosis in the left main coronary artery.1
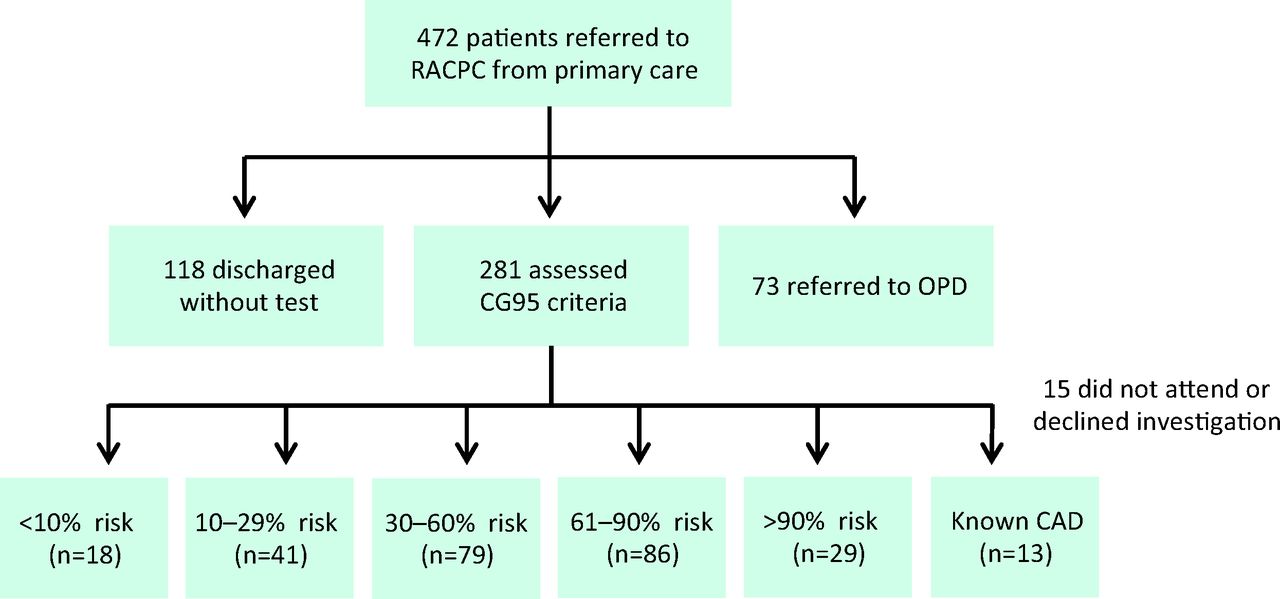
Summary of patient outcomes in the six-month pilot. CAD = coronary artery disease; OPD = outpatient department; RACPC = rapid access chest pain clinic.
Referral for each diagnostic test, stratified by predicted risk group.
All patients referred for CTCA underwent full studies, rather than calcium scoring. This was because it has been shown that significant CAD can occur in those with a low or absent calcium score,8 especially in young patients with soft plaque.
The guideline recommends discharging those patients judged to be at very low (<10%) risk of significant disease without testing. It was planned that as part of this pilot they would be tested in a similar way to the low-risk (10–29%) group. Additionally, the guideline recommends assuming significant disease in those judged to be at very high risk (>90%), and not routinely offering angiography to these patients. However, in this pilot it was decided to assess this group in a similar manner to the high-risk (61–90%) group, in order to assess the consequences of this recommendation. Thirteen patients with known CAD underwent ETT and were not included in further analysis.
Statistical analysis
All patients were prospectively included in an audit of the six-month pilot. Outcomes were assessed six months after the end date of the pilot. Statistical testing was by two-tailed Student's t test unless otherwise specified.
Results
A large group of patients were discharged without testing or being referred on to cardiology outpatients
In total, 118 patients (25%) were discharged from the RACPC without a test, having been assessed as having either no chest pain or chest pain that was clearly non-cardiac in origin. This group had a similar gender balance (44% female in both) but was significantly younger (mean 53.7±1.3 years vs 59.8±0.7 years, median 51 vs 61 years, p<0.0001) than the group referred for testing or to clinic. Seventy-two patients (15%) were referred directly to cardiology outpatients. These patients were judged to be suffering from problems other than angina, such as arrhythmia or heart failure.
Patients with a moderate predicted risk of CAD had a low observed incidence of CAD
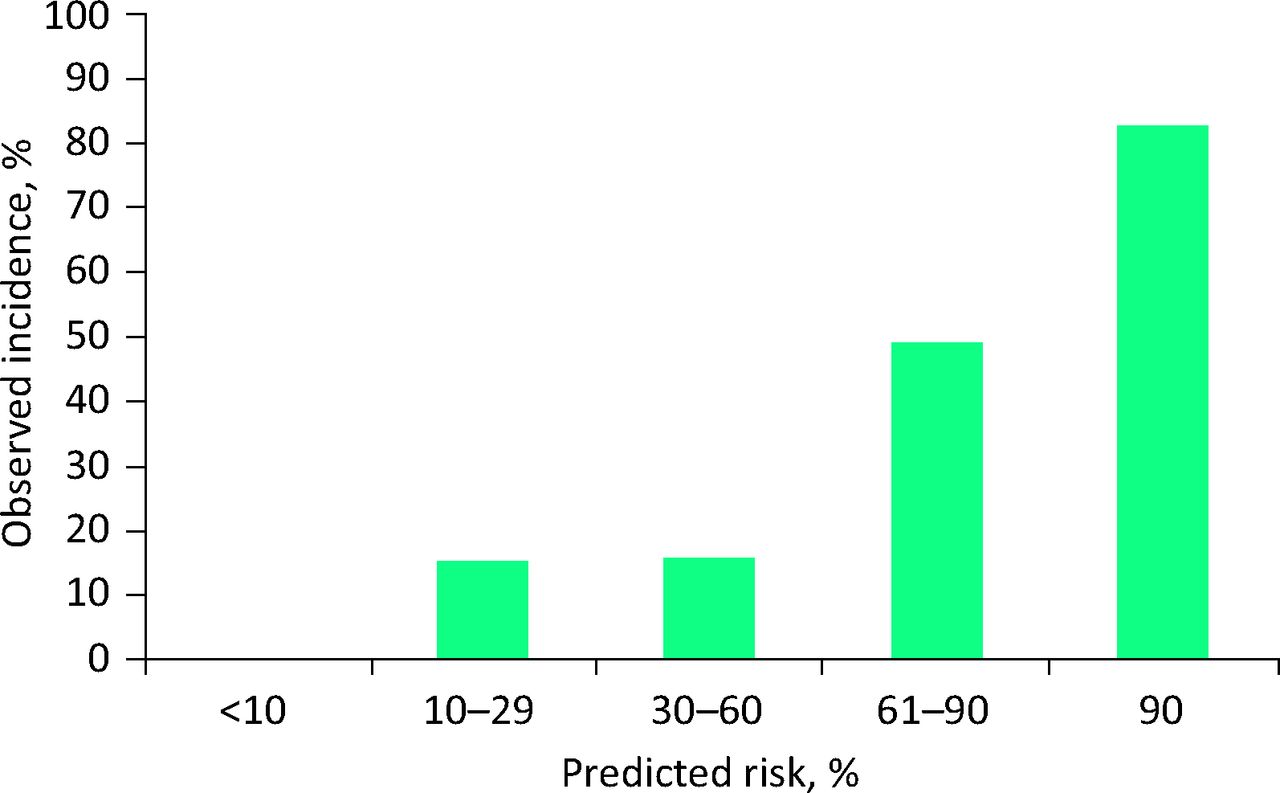
Patients in the moderate-risk group (30–60%) had a low observed incidence of CAD (15.2%) (Fig 2). This was similar to the incidence in the low-risk (10–29%) group (14.6%). The age of the low-risk group was similar to the moderate-risk group (mean 55.3±1.3 years and median 54 vs 55.5±1.2 years and median 57 years, p value not significant). Four moderate-risk patients (5%) underwent revascularisation in the follow-up period (two percutaneous coronary intervention (PCI), two coronary artery bypass surgery (CABS)), while no low-risk patient did (0%) (Fig 3). One patient (1.25%) in the moderate-risk group underwent functional testing after invasive angiography, and a further patient in the moderate-risk group had functional testing after a CTCA.

Incidence of significant coronary disease in each risk group.
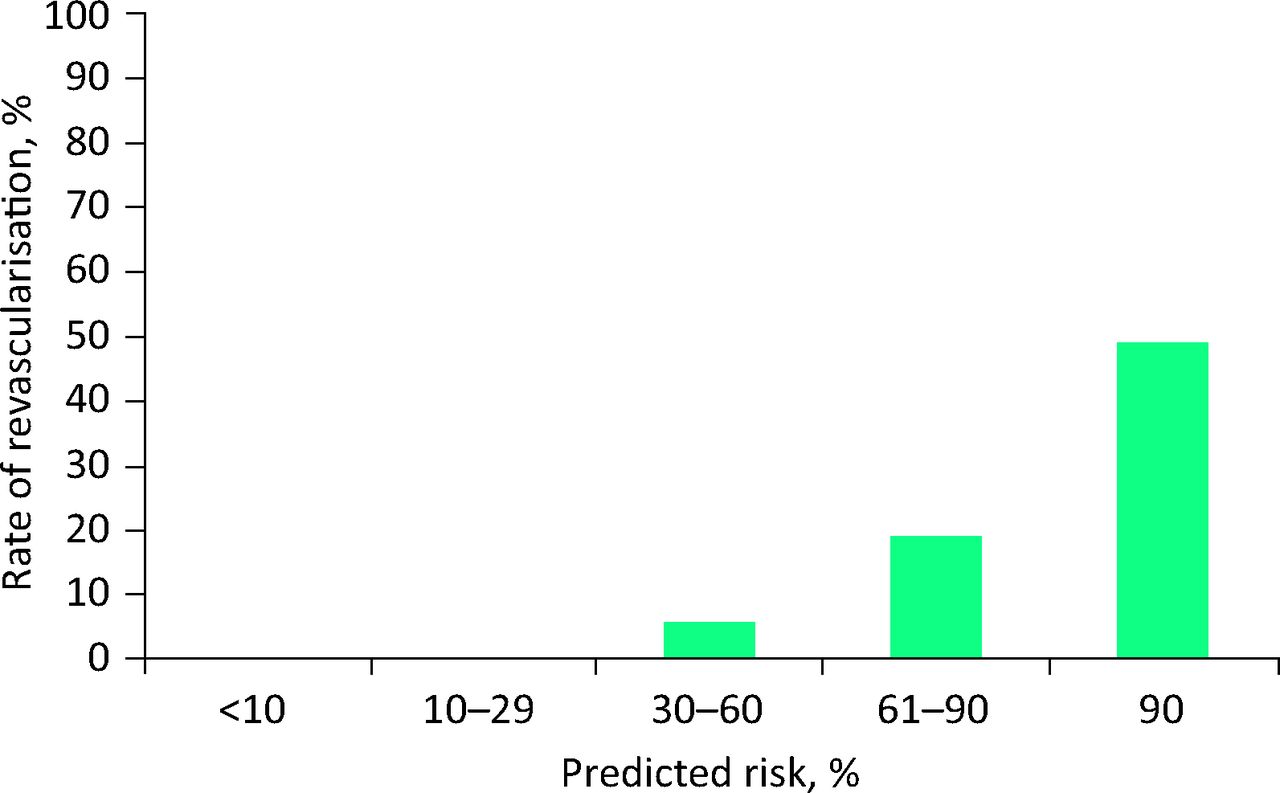
Proportion of patients revascularised by percutaneous coronary intervention or coronary artery bypass grafting in each risk group.
High- and very high-risk patients frequently required revascularisation and had a high incidence of prognostically significant disease
Sixteen patients (18.6%) in the high-risk group and 14 patients (48.3%) in the very high-risk group underwent revascularisation with PCI or CABS (Fig 3). Ten patients (11.6%) in the high-risk group and three patients (10.3%) in the very high-risk group underwent revascularisation for prognostically significant disease. Two patients (2.2%) in the high-risk group underwent functional imaging after angiography to assess the functional significance of lesions. Four patients in the very high-risk group underwent functional testing post-angiography (13.8%). Overall, eight patients (3.2%) across all risk groups required functional testing after anatomical tests (invasive angiography or CTCA) to assess the significance of stenoses. Six of these patients (2.4%) underwent myocardial perfusion studies and two (0.8%) had dobutamine stress echocardiography.
Frequent deviation from protocol
One-third (33%) of the very low-risk group and one-third (32%) of the low-risk group were referred for a test other than CTCA. Just under one-third (27%) of the moderate-risk group were referred for tests other than stress echocardiography, and one-third (32%) of the high-risk group were referred for tests other than angiography. In a small proportion of cases this was done on the advice of the supervising consultant. Seventeen patients (6.7%) were sent for ETT in the absence of known coronary disease.
Stress echocardiography and CTCA had a significant false-positive rate
Six patients (6.5%) had a stress echocardiogram suggestive of ischaemia, with no significant flow limiting coronary disease found at angiography. Exercise was the stressor in all cases. This may represent a training issue as the test is more technically demanding to perform and interpret than dobutamine stress echo. Two patients (5%) had false-positive CT coronary angiograms.
Discussion
Most UK hospitals offer a RACPC, and this is a popular and well-used service to primary care. However, there are many challenges to running an effective service. Overall, 40% of open access referrals to RACPC were deemed inappropriate. These patients were discharged without a test or referred directly on to general cardiology outpatients.
CG95 recommends no test in those with a predicted very low risk (<10%) and none of the patients in this group were found to have significant CAD. The guideline recommends no test in the very high-risk (>90%) group. Approximately half of such patients in our cohort (48%) were revascularised by percutaneous coronary intervention or coronary artery bypass grafting (seven patients for each). Five patients (17%) had immediate PCI at the time of angiography. This is a high rate of revascularisation and is similar to rates seen in acute coronary syndromes. Three patients (10%) were found to have prognostically significant disease, which would not have been identified had they been treated medically without angiography. The guideline does recommend discussing with the patient whether they would be willing to undergo revascularisation for prognostic reasons, and considering sending very high-risk willing patients for angiography.
In our population, patients with a moderate predicted risk of significant CAD (30–60%) had a low observed incidence of significant disease. These patients underwent revascularisation at a low rate, though more frequently than low-risk patients (5% vs 0%). CTCA performed well overall. There was a low rate of both false positives and technical failure. In a recent study, CTCA outperformed ETT in two cohorts of patients referred to the RACPC, with only a very minor additional cost.9 Though CTCA is generally substantially more expensive than ETT (approximately four-to-five-fold), it generated far fewer needless onward referrals owing to a lower rate of false positives. Interestingly, the Task Force on the management of stable CAD of the European Society of Cardiology, which reported in 2013, recommends CTCA for their ‘low-intermediate-risk’ group.10 This grouping uses a similar tool to CG95 but includes patients with a pre-test risk between 15–50%, therefore overlapping somewhat with our moderate-risk group.
Approximately one-third of each group (low-, moderate- and high-risk) underwent a different test than that specified by CG95, owing to deviations from the protocol. This was an unexpected result and implies that the guideline is not necessarily straightforward to follow in the real world. We are unable to establish from our dataset the exact cause of these deviations but they may reflect training issues, or in some cases decisions for good clinical reasons (for example stress echocardiography performed in place of CTCA to avoid radiation exposure in a young woman).
Conclusions
On the basis of this audited pilot study, the local RACPC is introducing an alternative strategy, based on a modification of NICE guideline CG95. All patients with a predicted moderate or low risk of CAD (≤60%) will undergo CTCA, while all patients with a high or very high risk (>60%) will continue to be referred for formal diagnostic angiography. In view of the demographic similarities between the moderate-risk group and those at lower risk, as well as the very low rates of significant disease and revascularisation, we believe this strategy will safely reserve resource-intensive functional imaging for the assessment of known CAD. The excellent sensitivity and negative predictive value of CTCA makes it the logical choice to rule out disease in low-risk patients. Patients with a very high predicted risk of CAD (>90%) will continue to be referred for formal angiography as they frequently require revascularisation and a significant proportion have prognostically significant coronary disease.
Acknowledgements
The authors would like to acknowledge the contributions of Harriet McCullough, Terri Thompson and Deborah Price.
- © Royal College of Physicians 2015. All rights reserved.








{kind=link}
{kind=link}
{kind=link}