
ABSTRACT
Cutaneous leishmaniasis is a parasitic disease caused by the Leishmania species, transmitted by the bite of an infected sandfly. The typical cutaneous lesion is a painless ulcer with a raised, indurated margin and often covered with an adherent crust. The lesions are mostly located on exposed sites such as the face and the extremities. Eyelid involvement is rare, making up only 2–5% of cases with facial cutaneous leishmaniasis. Herein, we report a 50-year-old male who presented with an erythematous plaque on the upper eyelid and multiple ulcerated nodules located on the extremities. Following microscopic examination of the lesional smear, a diagnosis of cutaneous leishmaniasis was made, and the patient was successfully treated with intramuscular meglumine antimonate therapy.
Introduction
Leishmaniasis is a protozoal disease caused by Leishmania species. Disease transmission occurs through the bite of a female sandfly infected with Leishmania parasites. 1 The disease has various clinical forms, such as cutaneous, mucocutenous and visceral, depending on the infecting Leishmania species and the host's immune response. Cutaneous leishmaniasis is the most common form, and although it typically presents as a skin ulcer on exposed regions of the body after a sandfly bite, atypical lesions on unusual sites may also be observed. 2 The eyelid is a rare site of involvement, consisting of only 2.5% of cutaneous leishmaniasis cases. 2 Herein we report on a case with eyelid leishmaniasis and multiple ulcerated lesions on extremities.
Case history
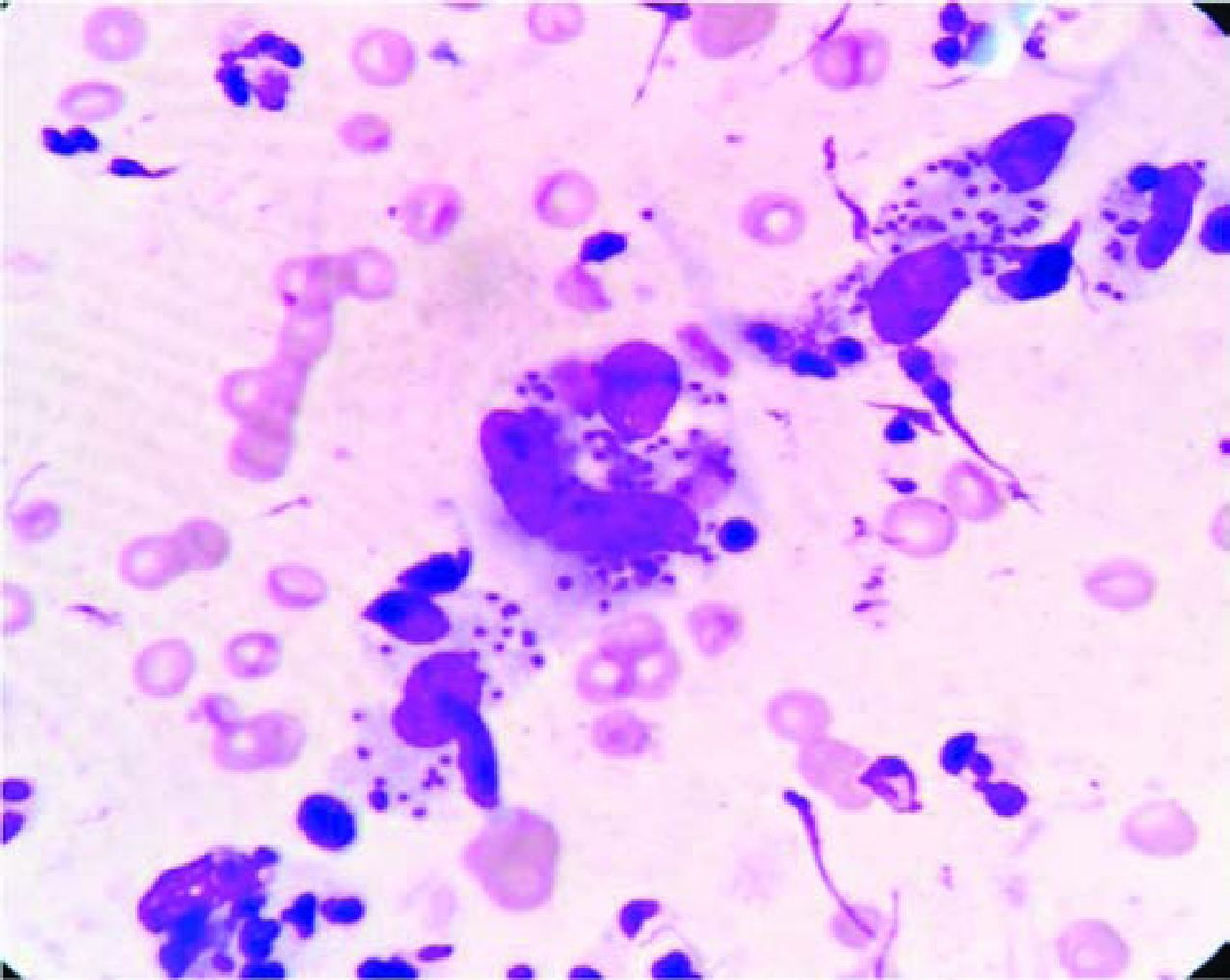
A 50-year-old male presented with a painless erythematous plaque on the eyelid that had been present for 7 months. Medical history revealed that he had migrated from Syria three months ago and he was bitten by a sandfly 10 months ago. Physical examination revealed an erythematous indurated plaque with central depression on the right upper eyelid (Fig 1), and six ulcerated erythematous nodules with raised indurated margins and overlying central crusts located on the distal regions of the right tibia, dorsum of the right foot and left forearm (Fig 2). A microscopic examination of the lesional smear stained with Giemsa revealed multiple amastigotes (Leishman–Donovan bodies) within the macrophages (Fig 3). The laboratory examination, including a complete blood count, erythrocyte sedimentation rate, C-reactive protein, blood chemistries and peripheral smear, gave results within normal limits and imaging examinations, including chest X-ray and abdominal ultrasonography, were unremarkable. Ophthalmological examination revealed no findings indicative of ocular involvement. With these findings, a diagnosis of cutaneous leishmaniasis was made. As there were multiple lesions and possible complications associated with eyelid involvement, systemic therapy was planned and intramuscular meglumine antimonate (Glucantime, Aventis, France) in a dose of 20 mg/kg/body weight was started. The patient tolerated the therapy well with mild symptoms of upper respiratory infection and arthralgia. After 20 doses of intramuscular Glucantime, all lesions, including those located on the eyelid, improved significantly (Fig 4) and the therapy was stopped. Clinical follow up was planned for the residual lesions and within two months of the follow up, most of the lesions, including the one on the eyelid, improved and were almost clear, except for the three lesions located on the right leg, which needed further local therapy in order to accelerate the healing process.

Erythematous indurated plaque with central depression on the right upper eyelid.

Multiple ulcerated lesions characterised by indurated raised margins, surrounding erythema and central adherent crusts on extremities.
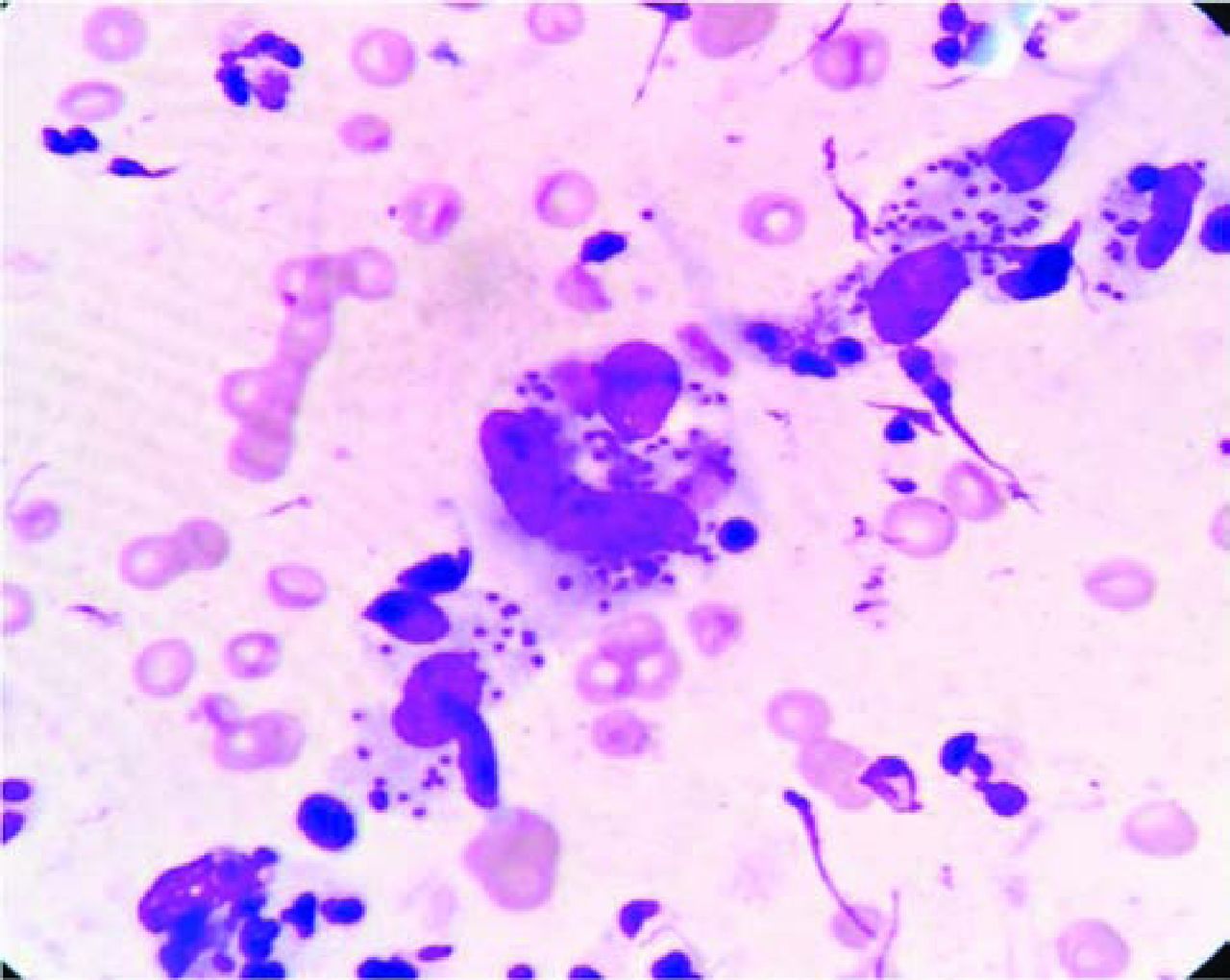
Multiple amastigotes in macrophages on microscopic examination (Giemsa stain, oil-immersion objective (magnification x100)).

Clinical improvement after 20 days of 20 mg/kg/day intramuscular meglumine antimonate treatment.
Discussion
Cutaneous leishmaniasis is endemic in Afghanistan, Algeria, Iran, Iraq, Saudi Arabia, Syria, specific regions in Turkey, Brazil and Peru. 1 A typical clinical presentation is characterised by a painless ulcer with an indurated raised margin and a necrotic base that is covered by an adherent crust, which develops on exposed sides after an incubation period of 1–12 weeks following the bite of an infected sandfly. 1 The face is a common site of involvement in cutaneous leishmaniasis, however eyelid involvement is rare and only makes up 2–5% cases with facial cutaneous leishmaniasis. 2 It has been suggested that the frequent movements of the eyelid prevent insects from biting the skin in that region. 3
The diagnosis of cutaneous leishmaniasis is based on clinically typical lesions, history of exposure and the endemicity of the disease in the region. 1 The most commonly used diagnostic method is the presence of amastigotes (Leishman–Donovan bodies) in macrophages on the microscopic examination of the tissue smears (obtained as tissue biopsy, needle aspirates or slit-skin smears) stained with Giemsa or haematoxylin and eosin stain. 1 Diagnosing the classical form of cutaneous leishmanisis based on clinical findings is usually not difficult, especially if the morphology and distribution of lesions are typical; however, an accurate diagnosis of atypical lesions appearing in non-endemic areas or occurring at unusual sites, such as the eyelids, can be difficult. 4
Eyelid leishmaniasis can have various clinical presentations and has been reported as chalazion-like lesions, ulcerated nodules, erythematous plaques or eczema-like, chronic granulomatous blepharitis-like lesions. 2 Long-term complications of eyelid leishmaniasis include scarring, contiguous spread to conjunctiva, sclera and cornea, secondary infections causing the destruction of underlying soft and bony tissue, lacrimal duct stenosis, ptosis, lagophthalmos, entropion, ectropion, scleromalacia and even blinding. 2 , 5–9 Differential diagnosis of eyelid leishmaniasis include tumors (such as basal cell carcinoma, squamous cell carcinoma and keratoacanthoma), tuberculosis, syphilis, histoplasmosis, rhinoscleroma, dacryocystitis, blepharitis, furuncle, chalazion and eczema. 2,8 Because of the potential risks of ocular involvement and further complications, early diagnosis and treatment of eyelid leishmaniasis is important. 2
The lesions of cutaneous leishmaniasis are usually self-limited. The main aims of the treatment are to accelerate the healing of the skin lesions, reduce the severity of scarring and the risk of recurrence, and to prevent dissemination of the disease and further complications. 1,10 Treatment choices include local and topical therapies (cryotherapy, intralesional injection of pentavalent antimony derivatives, local heat therapy and various topical paromomycin preparations), oral or parenteral systemic therapies. 10 Local and topical therapies are the initial choice for the uncomplicated cutaneous lesions. 10 Lesions on cosmetically and functionally important areas, such as nose, ear, eyelids, fingers and toes, those associated with lymphangitis, multiple and persistent lesions, those effecting immunosuppressive patients and lesions persisting after clinical failure with local therapies require systemic treatment. 10 Most commonly used systemic agents are parenteral (intramuscular or intravenous) pentavalent antimony derivatives: sodium stibogluconate and meglumine antimonate. 10 Their efficacy is well established if they are given in adequate doses and for an adequate period. 1 The recommended dosage is 10–20 mg/kg/day for 10–20 days. 10 Because of the eyelid involvement and presence of multiple lesions, we treated our patient with 20 mg/kg/day meglumine antimonate for 20 days. The lesions responded well to the treatment, and during follow up, the lesions had almost cleared and no relapse or ocular complications were observed.
In conclusion, considering cutaneous leishmaniasis in the differential diagnosis of chronic erythematous plaques or ulcerated lesions of the eyelids may help early diagnosis and treatment and hence prevent further ocular involvement and complications.
- © Royal College of Physicians 2015. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.