
A previously healthy 25-year-old male was admitted to the emergency department with severe chest pain soon after the consumption of 20 units of alcohol and snorting an unspecified amount of cocaine.
The chest pain was described as a central dull ache, radiating to the jaw and exacerbated by deep inspiration, eating and coughing. On examination, blood pressure was 118/68 with a regular pulse of 108 bpm. Oxygen saturations were 99% on air. Heart sounds were normal, jugular venous pressure was not raised and the chest was clear. The anterior chest wall was tender to palpation.
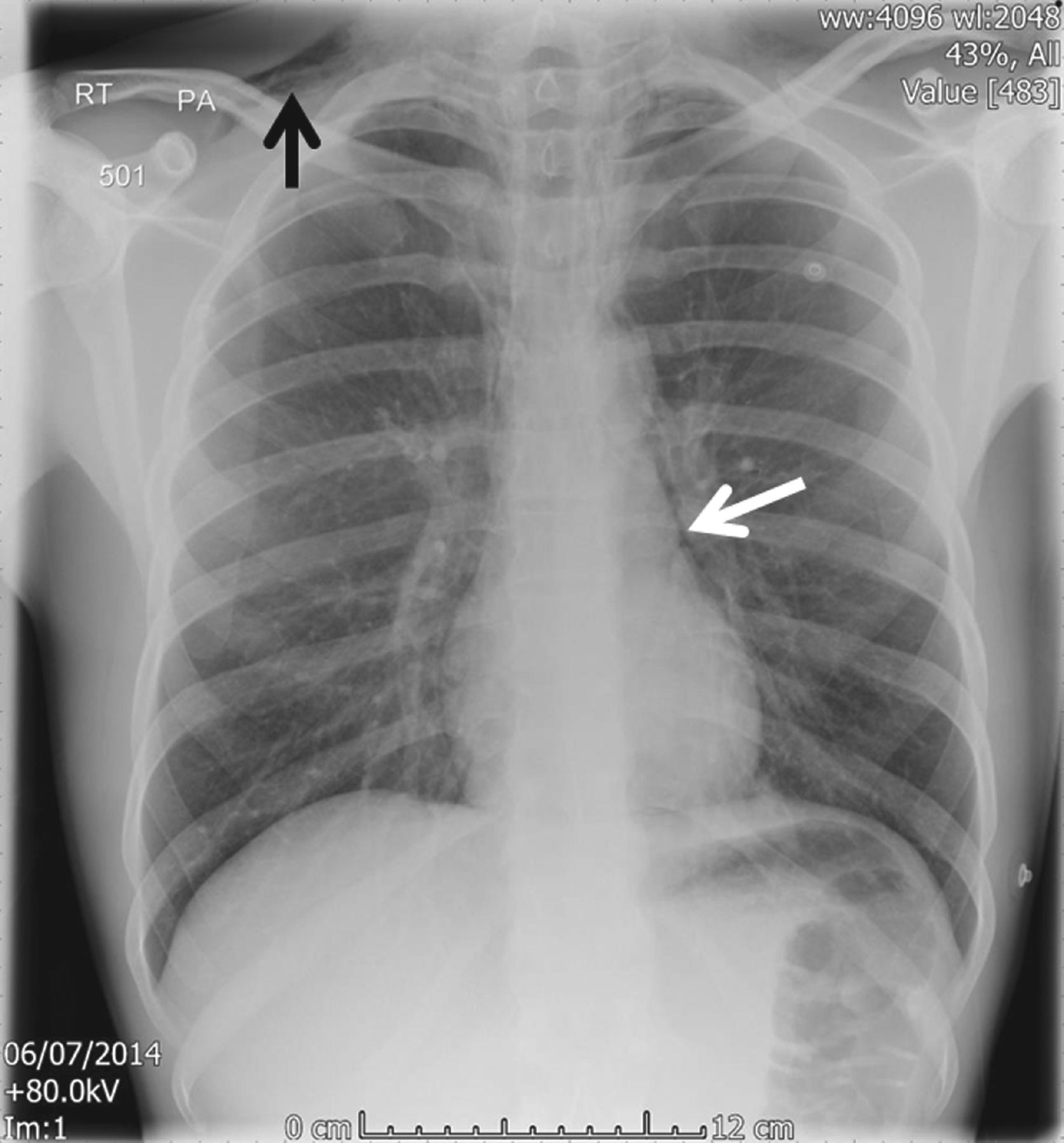
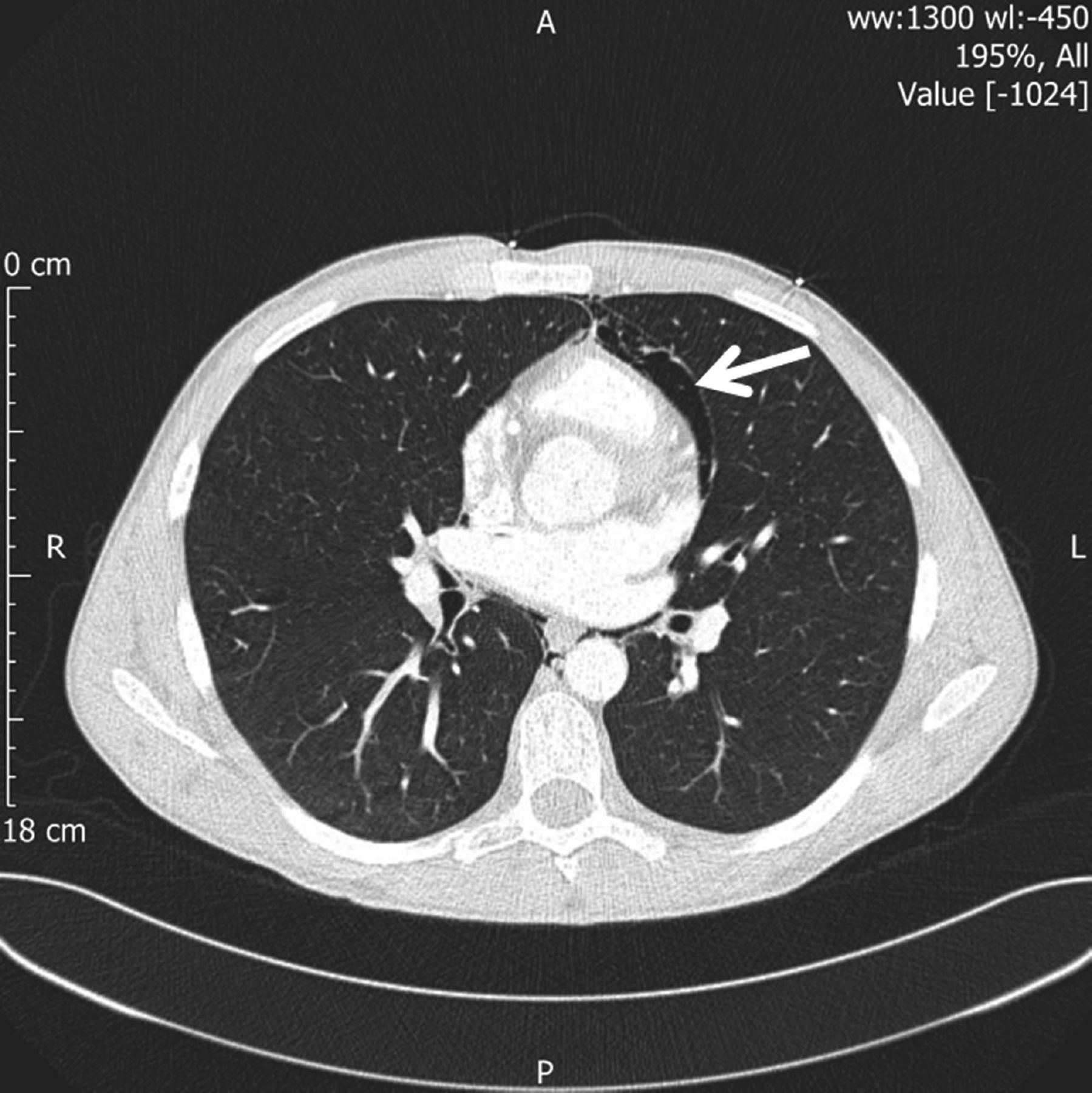
An electrocardiogram showed a sinus tachycardia, normal axis and no ischaemic changes. Blood tests on admission revealed an elevated troponin T of 44 ng/L (normal range, <14) (11 hours post-pain onset). He was referred to the cardiology team and a transthoracic echo demonstrated normal left ventricular systolic function and no regional wall motion abnormalities. The admission chest X-ray (Fig 1) demonstrated surgical emphysema in the right and left supraclavicular area (more obvious on the right) (black arrow) and a pneumo-mediastinum (white arrow). A computerised tomography chest scan confirmed these findings (Fig 2). Oral contrast did not show any leak from the oesophagus. Subsequent coronary angiogram demonstrated unobstructed coronary arteries. He was reviewed by the thoracic surgical team and treated conservatively. A follow-up chest X-ray two weeks later showed that the pneumomediastinum had resolved.

Admission chest X-ray.
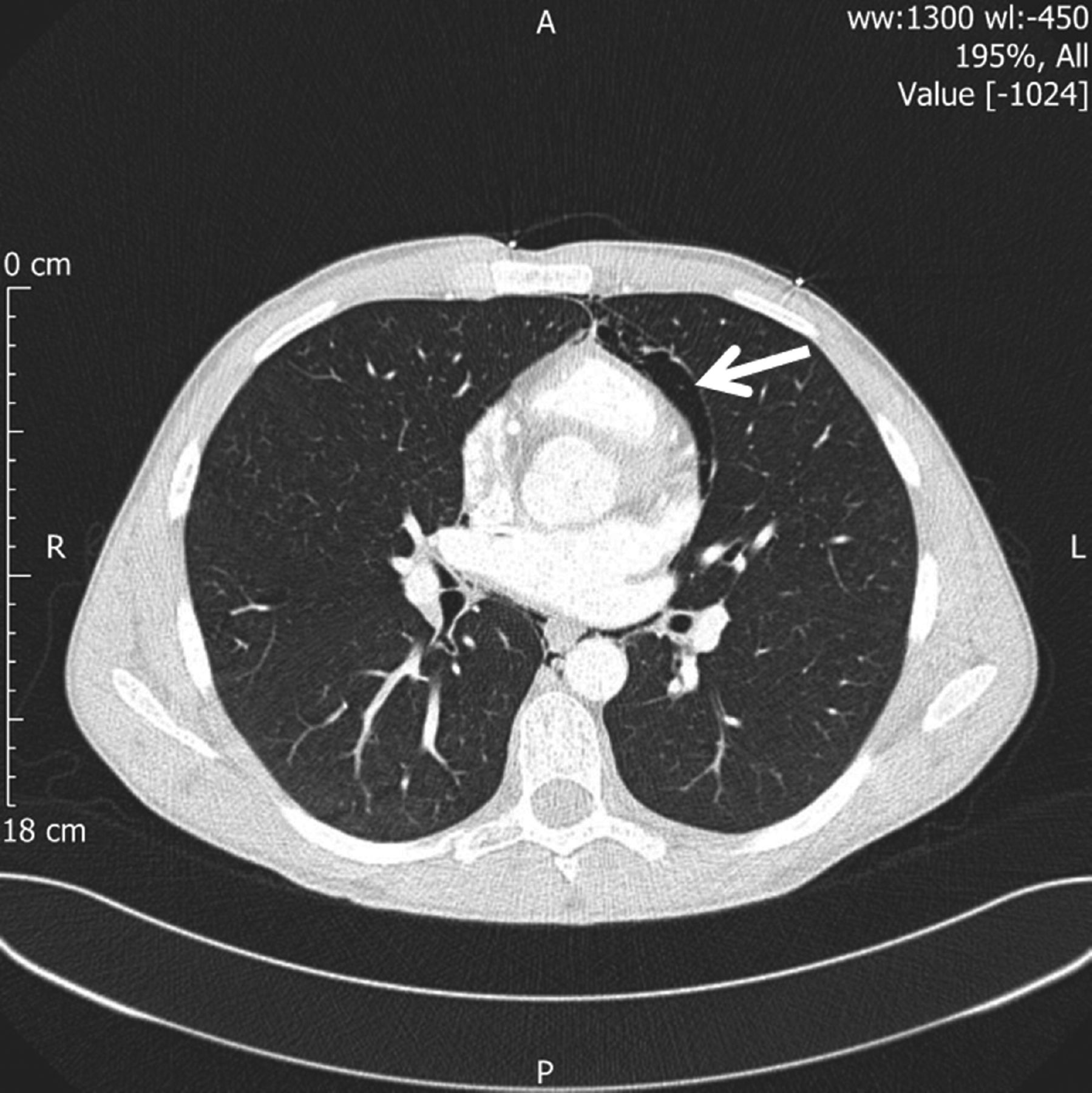
CT chest demonstrating pneumomediastinum.
Chest pain following cocaine use is a common presenting symptom.1 The majority of patients are young, male, smokers and have a previous history of cocaine abuse.2 The differential diagnosis of cocaine-induced chest pain includes:
aortic dissection
coronary artery vasospasm
acute coronary syndrome
pulmonary haemorrhage
pneumothorax
pneumopericardium
pneumomediastinum.2
Pneumomediastinum is an uncommon complication of cocaine use and occurs more often when smoked rather than following nasal inhalation.3 It has been hypothesised that the forceful snorting and Valsalva manoeuvre increase the pressure in the alveoli which can cause alveolar rupture and pneumomediastinum.3,4 In addition the direct toxicity of the cocaine on the lung tissue may produce rupture.3,4 Cocaine-induced pneumomediastinum is a benign condition and symptoms usually subside after 24 hours.5
- © Royal College of Physicians 2015. All rights reserved.








{kind=link}
{kind=link}