
ABSTRACT
Neutropenic sepsis is a life-threatening condition with mortality rates reported to range between 2 and 21% in adults. It can occur following chemotherapy treatment, due to disease (such as haematological conditions affecting the bone marrow) and in patients on disease-modifying agents (such as patients receiving methotrexate for rheumatoid arthritis). Appropriate emergency treatment is essential and achieving intravenous antibiotic door-to-needle time of less than 1 hour is a key target. Shortfalls in the management of patients presenting to teams with limited expertise in this area were identified in the National Confidential Enquiry into Patient Outcome and Death report in 2008, leading to recommendations including the need for an acute oncology service (AOS) at all hospitals with either an emergency department or medical admissions unit. Practice at Weston General Hospital has been audited at three time points since 2008 (in 2008, 2011 and 2013–14) during which there have been several service developments relevant to the management of neutropenic sepsis, including the introduction of an AOS in June 2013. The percentage of patients in which intravenous antibiotic 1-hour door-to-needle time was achieved has improved from 14% (2008) to 31% (2011) to 79% (2013–14) and neutropenic sepsis mortality has decreased from 39% (2008) to 14% (2011) to 0% (2013–14).
Introduction
Neutropenic sepsis has been defined in the National Institute for Health and Care Excellence guidelines1 as a neutrophil count of <0.5x109/L and either a temperature higher than 38°C or other signs or symptoms consistent with clinically significant sepsis. This is based on neutropenic sepsis protocols usually defining neutropenia as an absolute neutrophil count of <0.5x109/L or <1.0x109/L and ‘falling’. The interpretation of ‘falling’ requires some knowledge of chemotherapy regimens and expected patterns of myelosuppression. Also, fever is a common but not the only manifestation of infection (for example, patients may present with hypothermia) and a clinically significant fever has been defined variously as 37.5, 38 or 38.5°C over different time points. Urgent treatment is necessary because delays in receiving antibiotic treatment result in increased mortality,2 and ‘door-to-needle time’ for administration of intravenous antibiotics should be less than 1 hour.3
The National Confidential Enquiry into Patient Outcome and Death4 and other reports3,5,6 have shown evident shortcomings in the management of oncological emergencies and indicate a need for around-the-clock access to oncology expertise. This led to the recommendation that all hospitals with either an emergency department (ED) or a medical admissions unit (MAU) should have an acute oncology service (AOS). An AOS should provide expert advice for managing patients presenting with toxicities arising from chemotherapy and radiotherapy treatments, acute cancer-related complications (in particular better management of metastatic spinal cord compression) and new cancers in the acute care setting.7 It has been an excellent advance to have UK Oncology Nursing Society guidelines produced for the management of oncological emergencies.8 Further to this, it is paramount that the AOS in each hospital ensures that these guidelines and related pathways and protocols are implemented in an effective and seamless manner for that particular hospital.
Process of care and audit of practice at Weston General Hospital
Chemotherapy is given at Weston General Hospital on an outpatient basis in an oncology and haematology day unit with six treatment chairs and two treatment beds. Workload has significantly increased with chemotherapy being given to more than 100 patients each week. There are no oncology inpatient beds at Weston General Hospital and so patients presenting with oncological emergencies are admitted under the medical on-call team. Patients present to the hospital by attending the ED, the oncology and haematology day unit or the MAU directly (following referral to the medical on-call team). The admitting doctor then assesses the patient and prescribes intravenous antibiotics, following which the nursing staff administers the antibiotics. Since the introduction of a Patient Guided Directive in April 2014, trained nursing staff have been able to administer intravenous antibiotics in cases of suspected neutropenic sepsis without needing to wait for a doctor's review.
The Multinational Association for Supportive Care in Cancer (MASCC) risk index9 is a scoring tool which identifies whether the neutropenic sepsis episode is either low risk (score ≥21) or high risk (score <21). By identifying patients with low-risk neutropenic sepsis, it might be possible to switch the route of antibiotic administration from intravenous to oral at an early stage (soon after 24 hours of intravenous antibiotics) and treat as an outpatient. It should however be noted that a UK clinical research network trial, the ORANGE trial (ORal Antibiotics for Neutropenic sepsis Giving Early hospital discharge), was set up to investigate this; however it was closed early because of poor recruitment.10 Given this to be the case, risk stratification of neutropenic episodes with the MASCC risk index and early discharge of low-risk cases with oral antibiotics and telephone follow-up is not currently done at Weston General Hospital. If this is introduced, clear audit would be necessary to evaluate its impact.
As well as several service developments at Weston General Hospital since 2008 relevant to the management of neutropenic sepsis, the official launch of the AOS was in June 2013. The AOS at Weston General Hospital is a nurse-led service (two experienced oncology nurses with access to support from oncology and haematology specialty doctors and consultants). Based on three audits performed in 2008, 2011 and 2013–14, we report the impact of these service developments on intravenous antibiotic 1-hour door-to-needle time and neutropenic sepsis mortality. Lessons learned will be discussed.
Methods
Three audits of neutropenic sepsis have been done at Weston General Hospital since 2008 and are presented in this paper. Neutropenic sepsis was defined as a neutrophil count <1.0x109/L and either a temperature higher than 38°C or other signs or symptoms consistent with clinically significant sepsis. Having the same definition of neutropenic sepsis for all three audits ensured consistency for when comparing results from these audits.
Audits 1 and 2 were retrospective and included patients presenting between 1 January 2008 and 31 January 2008 (12-month period) and between 1 January 2011 and 1 June 2011 (6-month period), respectively. All adult patients (aged 18 years and older) who had neutropenia in the time periods of the audits were identified through coding for audit 1 and using the ICE desktop for audit 2. For both audits, hospital notes for those patients who had been admitted to Weston General Hospital were retrieved and review of the notes determined if they presented with neutropenic sepsis. Data were collected by completing an audit proforma for each neutropenic sepsis episode.
Audit 3 is prospective and patients were identified by various methods. These include referral to the AOS team by the ED, admitting hospital team or oncology and haematology day unit, depending on the route of patient admission. Also a flagging system is in place that generates a daily report for all patients who have attended the ED and who are also on the Somerset Cancer Register. This report is reviewed daily by the AOS team and patients listed on it are followed up. A door-to-needle time review is undertaken on all patients admitted with possible neutropenic sepsis and entered on a specifically made neutropenic door-to-needle time database. The time that the patient presents to hospital (door time), the pathology blood test time, and the time of administration of intravenous antibiotics (needle time) are recorded. Tumour site, chemotherapy regime, chemotherapy dosage (whether full or partial), blood results, whether the patient required admission and any relevant comments are also recorded. Since the introduction of the AOS at Weston General Hospital in June 2013, monthly audit reports, with door-to-needle time figures and whether there are any learning points or recommended improvements needed, have been produced and distributed to key staff involved in the management of neutropenic sepsis at the hospital. Key staff groups include all medical and nursing staff working in the ED, MAU and the oncology and haematology day unit. Also, the AOS team liaises with any specific person or team member if any urgent concerns have been raised at the time of collecting data. This prospective approach to audit is ongoing and in this paper we present figures for the first year since this audit approach has been adopted (ie from 17 June 2013 to 16 June 2014).
Outcomes assessed in the analysis of all three audits were (1) the percentage of patients in which intravenous antibiotic 1-hour door-to-needle time was achieved and (2) the neutropenic sepsis mortality (expressed as a percentage of the total number of cases presenting with neutropenic sepsis).
Details and dates of service developments that have occurred over the time period of the three audits are listed in Box 1.
Service developments at Weston General Hospital
Results
Audit 1 (2008)
In this retrospective audit, 36 cases of neutropenic sepsis were identified in 35 patients (one patient had two episodes in the 12-month period). Of these cases there were 19 patients with solid tumours receiving chemotherapy, 10 patients with haematological malignancy receiving chemotherapy, two patients with congenital neutropenia, two patients with rheumatoid arthritis receiving methotrexate, one patient with Crohn's disease, and one patient receiving carbimazole.
Five of the 36 cases (14%) received intravenous antibiotics within 1 hour. Neutropenic sepsis death occurred in 14 of the 36 cases (39%) and 2 of the deaths were in patients receiving methotrexate for rheumatoid arthritis. Of the two deaths of patients receiving methotrexate, one was a 79-year-old patient with Felty's syndrome who had been on methotrexate for rheumatoid arthritis for five years. The patient was admitted from a residential home with respiratory compromise and clinically dehydrated with vomiting, mouth ulcers and limited oral intake. Neutrophil count was 1.1x109/L on admission and 0.9x109/L the following day and intravenous antibiotics were started at 6pm in the evening of the day after admission. The patient's background fitness was poor and ceiling of care was ward based given their frailty. Despite treatment with intravenous fluids and antibiotics, the patient became less responsive over the next few days and died as a result of pneumonia, neutropenia secondary to methotrexate and a cerebrovascular event. The other patient was 58 years old, had had Still's disease since the age of 12 years, had been on methotrexate for five years, and was admitted as a general practitioner referral unwell and hypotensive. On admission, the patient was apyrexial, but there was evidence of haemodynamic compromise with blood pressure of 87/38 mmHg and heart rate of 100 bpm. Neutrophil count was 0.2x109/L. Intravenous fluids and intravenous antibiotics were given 6 and 8 hours after admission, respectively, and the patient died the following day. Gram-negative bacilli (Pseudomonas) were grown on blood culture. The patient had persistent leg ulcers (five years) and these were the likely source of infection. The death certificate listed cause of death as (1a) sepsis (pseudomonas); (1b) bilateral leg ulcers; and (1c) renal failure. Although neutropenia secondary to methotrexate was a contributory factor to this patient's death, it had not been included on the death certificate. Subsequent review of the death certificates of all patients included in this audit showed that nearly one-third (4 of 14) of the patients who died from neutropenic sepsis had no record of neutropenic sepsis either as a cause of death or as a contributory factor on their death certificate. This implies that neutropenic sepsis mortality data cannot accurately be obtained from death certification.
Audit 2 (2011)
This audit was done following service developments put in place after audit 1 to improve the outcomes of patients with neutropenic sepsis. In this retrospective audit, 29 cases of neutropenic sepsis were identified involving 25 patients (4 patients were admitted twice during the 6-month period). Of these cases there were 14 patients with solid tumours receiving chemotherapy, 8 patients with haematological malignancy receiving chemotherapy, 1 patient with leukemia causing pancytopenia, 1 patient with autoimmune cytopenia and 1 patient with rheumatoid arthritis receiving methotrexate.
Nine of the 29 cases (31%) received intravenous antibiotics within 1 hour. Neutropenic sepsis death occurred in 4 of the 29 cases (14%) and 1 of the deaths was in a patient receiving methotrexate for rheumatoid arthritis. This patient was 79 years old, had been on methotrexate for five years, and was admitted with right pleuritic chest pain, productive cough and respiratory compromise. On admission, the patient was apyrexial, tachycardic (heart rate 100 bpm) with blood pressure maintained at 150/50 mmHg, and tachypnoeic (respiratory rate 28 breaths per minute) with oxygen saturation of 86% on 5 L/minute oxygen. Neutrophil count was 0.5x109/L. Intravenous antibiotics were prescribed 4 hours after initially seeing the admitting doctor, and these antibiotics were not given for a further 2.5 hours. The patient deteriorated and despite the involvement of the intensive care team died the next day following cardiopulmonary arrest and attempted resuscitation. Cause of death was bronchopneumonia and neutropenic sepsis as a result of methotrexate drug treatment.
Audit 3
In this prospective audit, covering the first year since the official launch of the AOS at Weston General Hospital (17 June 2013 to 16 June 2014), 76 cases of neutropenic sepsis were identified. Sixty of the 76 cases (79%) received intravenous antibiotics within 1 hour and there have been no deaths from neutropenic sepsis in this time period. The last time that a death from neutropenic sepsis was seen at Weston General Hospital was June 2012.
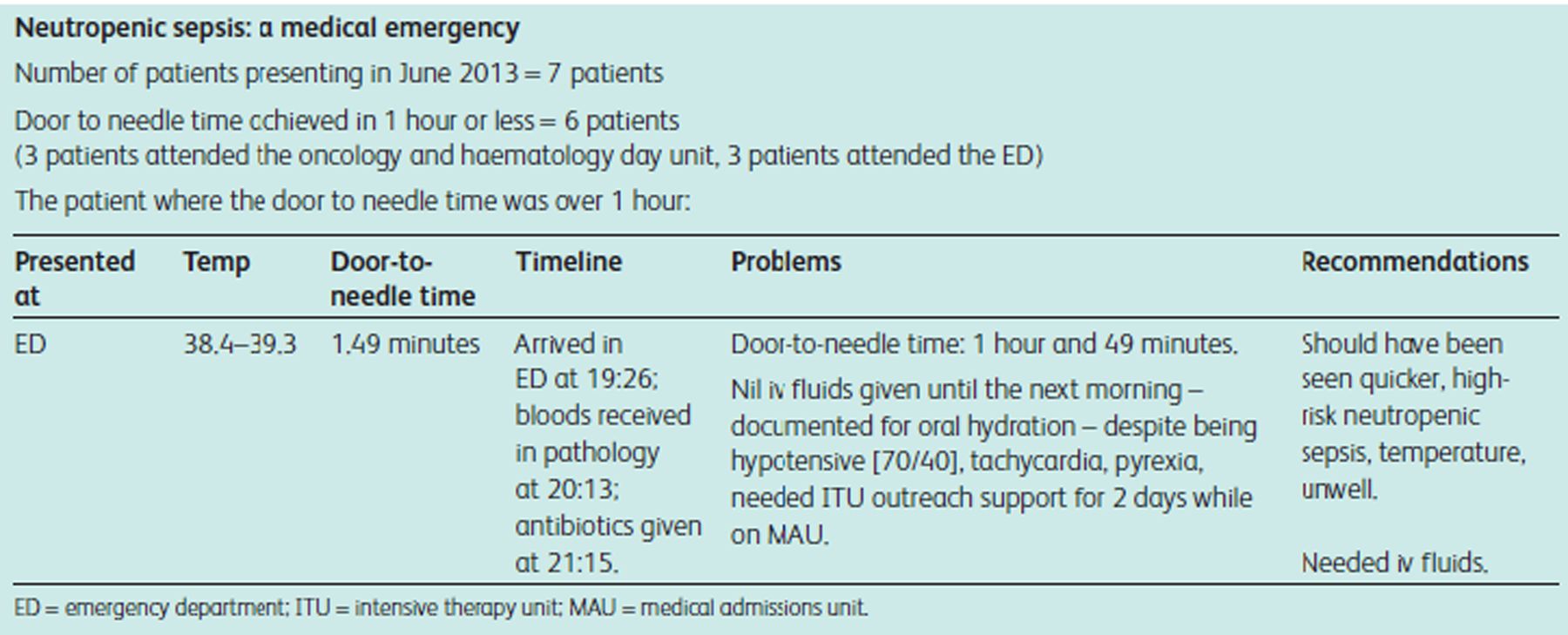
As part of this ongoing prospective audit, a monthly report with audit results and learning points is distributed monthly to key staff involved in the management of patients with neutropenic sepsis (see Box 2 for an example of a monthly audit report).
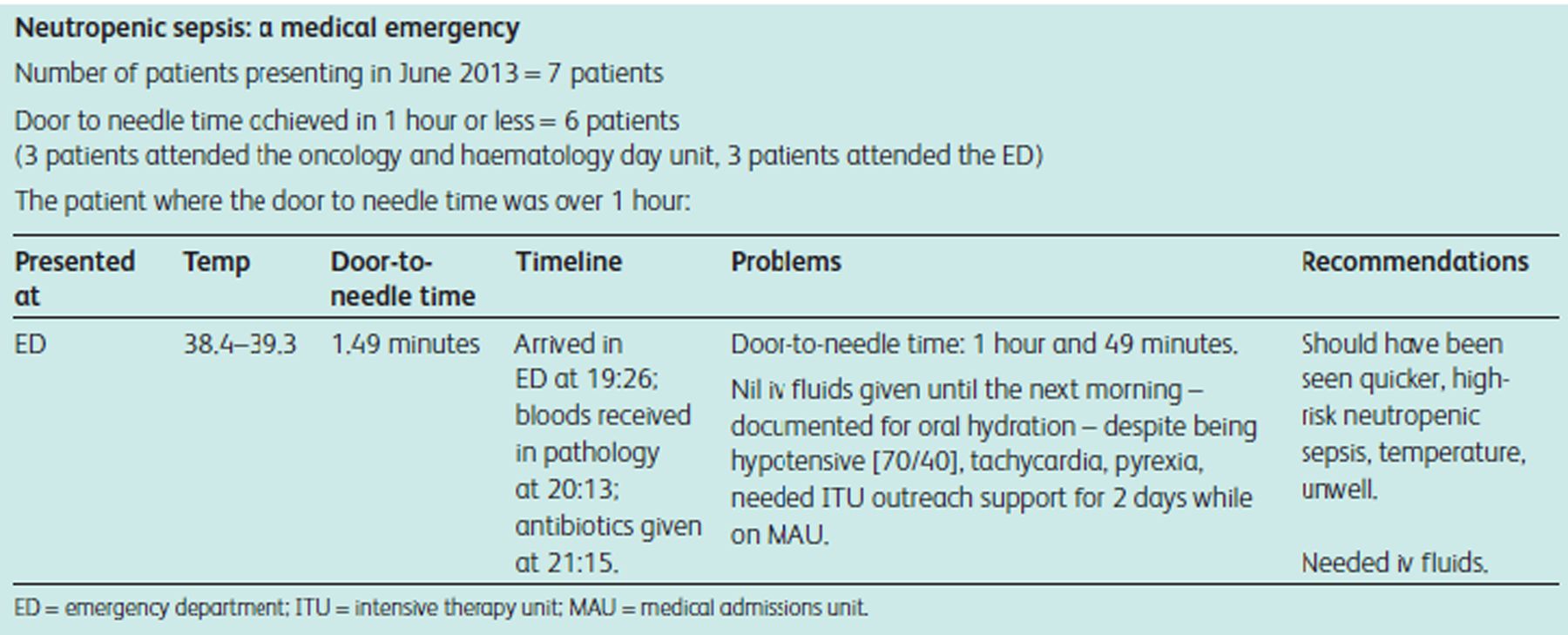
Example of monthly audit report with feedback (distributed as part of ongoing prospective audit since June 2013)
Audits 1, 2 and 3
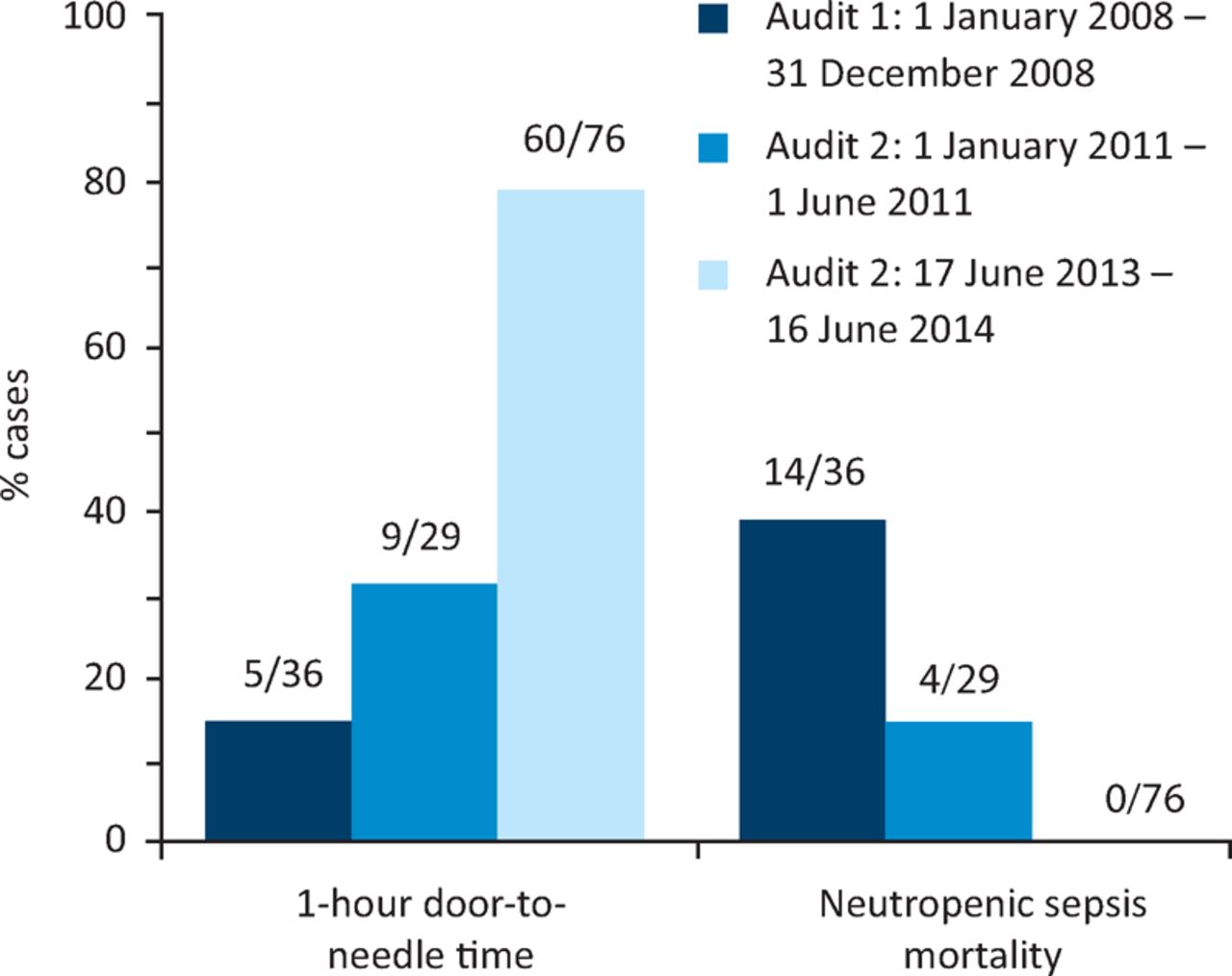
Improvements in door-to-needle time and neutropenic sepsis mortality from audit 1 to audit 2 to audit 3 are shown in a bar chart in Fig 1.
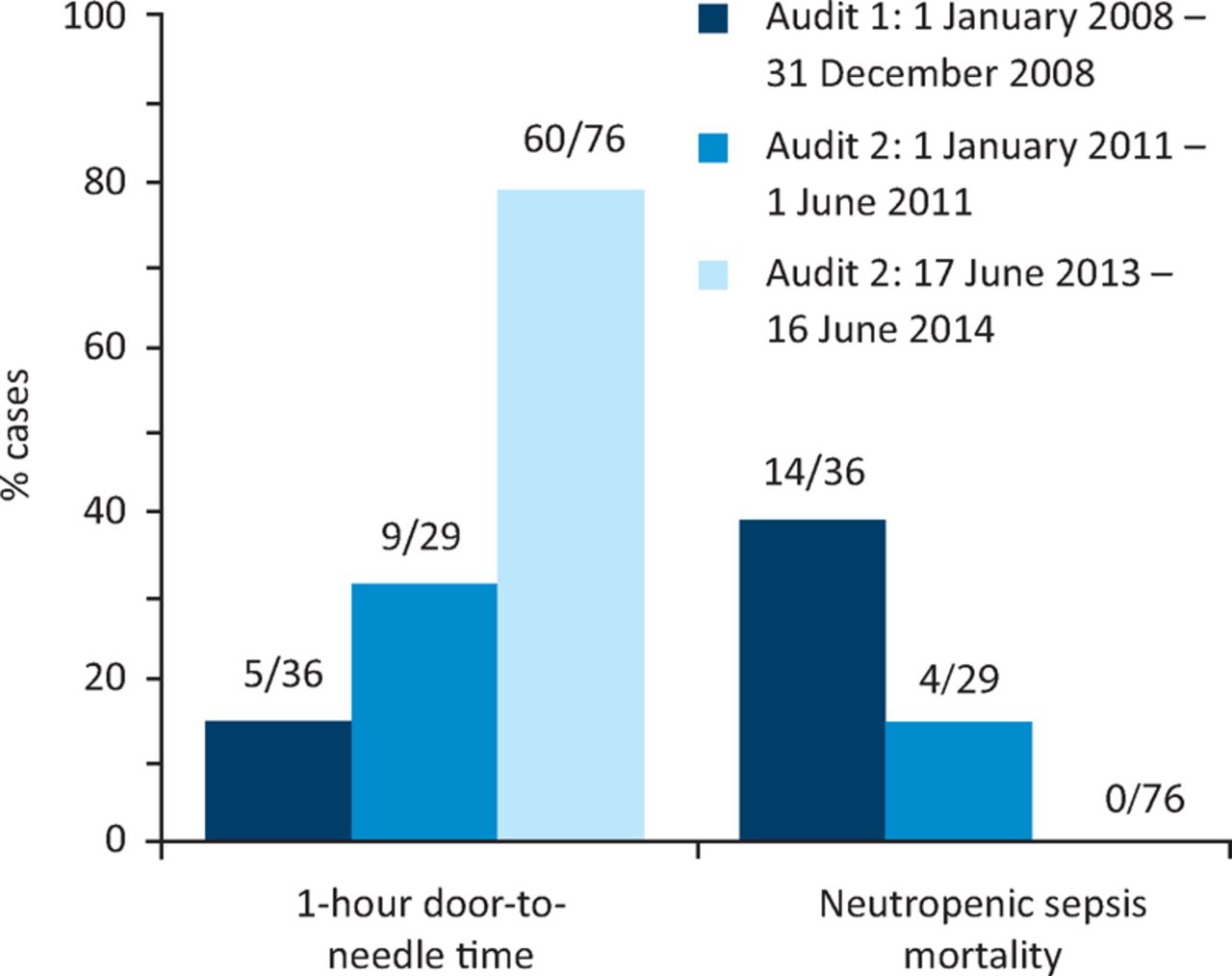
One-hour door-to-needle times and neutropenic sepsis mortality figures for audits performed in 2008, 2011 and 2013–14.
Discussion
An increase in the incidence of neutropenic sepsis is evident over the time period of the three audits (36 cases in audit 1 over a 12-month period, 29 cases in audit 2 over a 6-month period, and 76 cases in audit 3 over a 12-month period) and this reflects an increase in the chemotherapy treatment workload at Weston General Hospital. However, data collection methods for the first two audits and their retrospective nature may have led to cases being missed. Despite chemotherapy treatment workload greatly increasing, significant improvements in the management of patients with neutropenic sepsis have been achieved. From 2008 to 2014, intravenous antibiotic door-to-needle time within 1 hour has improved from 14 to 79% and neutropenic sepsis mortality has decreased from 39 to 0%. In fact the last death from neutropenic sepsis at Weston General Hospital was in June 2012. Of note, 2 and 1 of the neutropenic sepsis deaths in the 2008 audit and 2011 audit, respectively, were in patients on methotrexate for rheumatoid arthritis, which indicates that improvements in managing neutropenic sepsis are of importance for any patient at risk of myelosuppression and not just for patients with cancer receiving chemotherapy.
Ongoing monthly distribution of audit figures and real-time feedback with visible presence of the AOS team in essential clinical areas have led to a learning rather than a blame culture, and achieving high standards in the management of neutropenic sepsis has become engrained as a key hospital target. Although difficult to determine the impact of each particular service development, collectively the management of neutropenic sepsis has been greatly improved. Continued education of key staff is paramount to sustaining and improving this service, particularly in view of staff turnover and the rotation of some staff to other hospital placements. One important factor since the introduction of the AOS at Weston General Hospital has been the willingness of the acute medical and emergency department teams to be an integral part of the process in delivering this care. Also one should not ignore the importance of educating patients and their relatives about neutropenic sepsis and what they need to do.
While we continue to work on how to improve the process even further, we feel that other hospitals can learn from what has already been achieved at Weston General Hospital. Given the improvements seen and that neutropenic sepsis mortality has fallen from 39 to 0%, the culture at our hospital is that a neutropenic sepsis death should now be regarded as a ‘never event’. Lessons learned have been fed back to other hospitals in our Strategic Clinical Cancer Network.11
- © Royal College of Physicians 2015. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.