
ABSTRACT
The Royal College of Physicians' FallSafe care bundles constitute measures of good practice, some of which are recommended for all patients, some are additional measures for older and more vulnerable patients admitted to hospital, and there is another bundle for after an inpatient fall, to reduce the number of inpatient falls. In 2013 a dedicated healthcare assistant, trained by the falls team, started a monthly spot audit looking at preventative measures, on all inpatients on every ward of the trust. Monthly results were fed back to the ward managers, ward falls liaison nurses, doctors, therapists and pharmacy staff on each ward, to discuss at the monthly ward governance meetings. Training and advice on specific aspects of falls prevention were provided by falls nurse practitioners. In total, 9,679 patient episodes were recorded over the year. Compliance with the measures recommended by the FallSafe care bundles has improved following regular spot audit and training. This has led to an overall reduction in the number of inpatient falls. Despite this however, in the real world of changing patient demographics, ward closures and the increasing use of ambulatory care, the number of falls/1,000 bed days has increased.
Introduction
Over 280,000 patient falls are reported from acute, community and mental health units in England and Wales annually.1 They can cause serious injury and death and cost approximately £15 million per annum.2 Systematic review suggests multifactorial assessment and intervention can reduce falls by 20–30%.3 The Royal College of Physicians’ (RCP's) FallSafe quality improvement project took the successful components and formed them into care bundles to prevent and manage falls in clinical hospital wards in Southern England SHA.4,5 The FallSafe care bundles therefore represent measures of good practice, some of which are recommended for all patients, some are additional measures for older and more vulnerable patients admitted to hospital, and there is another bundle for after an inpatient fall, to reduce the number of inpatient falls (Box 1).
The FallSafe care bundles
Northumbria Healthcare NHS Foundation Trust (NHFCT) includes three teaching district general hospitals and six community hospitals. There are 58 wards of varying age, design layout and specialty (including mental health), with a total of 1,048 beds (of which 34% are single rooms and only 13% of bed spaces are visible from a nursing station). We report the experience of the NHFCT falls team in trying to implement these recommendations into routine clinical practice across a large NHS foundation trust.
Methodology
The existing NHCFT mandatory falls training for nurses and healthcare assistants (HCAs), provided by members of the falls team and renewed three yearly, already focused on specific aspects of falls prevention (including documenting and acting upon the relevant sections of the Falls Care Plan and on the importance of accurate incident reporting). All information for the audit was therefore able to be retrieved from the existing medical, nursing and therapy documentation without the need for modification.
The FallSafe care bundles were modified and some measures adapted to ensure a trustwide ability to comply and to allow easier audit.
Bundle for all patients
1. A history of previous falls and of ‘fear of falling’ is taken at the time of admission: this audit measure was assessed by the information recorded in the nursing admission document or the accident and emergency (A&E) admission document.
2. Urinalysis is conducted on admission: this measure was recorded from the A&E admission document, medical assessment unit documentation or the nursing admission document.
3. No prescriptions of night sedation: in order for this to be performed relatively easily by the falls HCA, without access to a medication reconciliation databases, this measure relating to ‘new prescriptions of night sedation’ was adjusted to ‘any prescription of night sedation’. This measure was collected from review of the drug kardex.
4. Appropriate footwear is in use: a significant number of elderly patients are admitted without suitable or appropriate footwear. For those without appropriate footwear, the trust purchased supplies of slipperettes. These come in two sizes and have a sole with rubber grips, which if worn appropriately, makes mobilising on the shiny hospital floors less hazardous. This measure was audited by assessing the patient at the patient's bed space.
5. A call bell is within site and reach: this measure was usually audited at the patient's bed space. Some patients, who were freely ambulant, were not included when using day rooms or sitting areas. However immobile patients, or patients who required assistance to mobilise, who were placed in such areas were audited.
6. Glasses are within site and reach: this measure was added into the care bundle for all patients and audited at the patient's bed space.
7. Mobility aids are within site and reach: this measure was also audited at the patient's bed space. We initially found there was a misplaced perception that by taking the walking aid away from a confused patient you will stop them attempting to mobilise. This had led to the walking aids being tidied at the end of the bay or deliberately placed away from the patient's immediate reach. Where this problem was encountered additional education was provided to the ward and therapy staff by the falls team.
Bundle for older and more vulnerable patients
8. Cognition assessment: this audit measure was assessed by reviewing the information recorded in the A&E admission document. This was part of an existing trust Commissioning for Quality and Innovation project (CQUIN).
9. Delirium assessment: this audit measure was assessed by reviewing the information recorded in the A&E admission document. This was part of an existing trust CQUIN.
10. Visual assessment: While this audit measure is in the care of the elderly nursing documentation, an actual visual assessment was rarely performed by nursing staff and instead the use of glasses was recorded. The physiotherapy teams were performing visual assessments, but were only initially documenting their findings for patients on the stroke pathway. By enlisting the physiotherapy team to document the visual assessments they perform on all patients, we were therefore able to assess this audit measure by reviewing the physiotherapy notes.
11. Bed rail assessment: assessed by reviewing the ‘bed height, rail and mat matrix’ included in the care of the elderly nursing documentation.
12. Lying and standing blood pressure: recorded using automated blood pressure monitoring devices as per a specific protocol included in the care of the elderly nursing documentation. Additional training and support was already in place for ward teams from the falls team prior to this audit.
13. Continence plan: assessed by reviewing the continence pathway included in the care of the elderly nursing documentation.
14. Cardiovascular or central nervous system (CNS) culprit medication: this measure was assessed by review of the drug kardex and comparing the medication list to the Medicines and falls in hospital: guidance sheet.6 This required additional training and support for the HCA from the falls team.
Bundle for after a fall
The falls team had previously modified the Nottingham University Hospitals’ Medical report following a fall and produced a sticker, which is inserted into the medical notes and is completed by the doctor or nurse practitioner after reviewing the patient who has fallen. This sticker and the medical and nursing responses to the fall, were audited by the falls team nurse practitioners against the measures recommended.7
Outcome data
Monthly audit results were fed back via e-mail to the ward managers, ward falls liaison nurses, doctors, therapists and pharmacy staff on each ward to discuss at the monthly ward governance meetings.
Data for falls and occupied bed days were collected from the trust incident reporting system and occupancy data, so that ‘falls/1,000 bed days’ could be calculated. When reporting an injury the National Patients Safety Agency classifications of harm were used.2
Results
Bundle for all patients
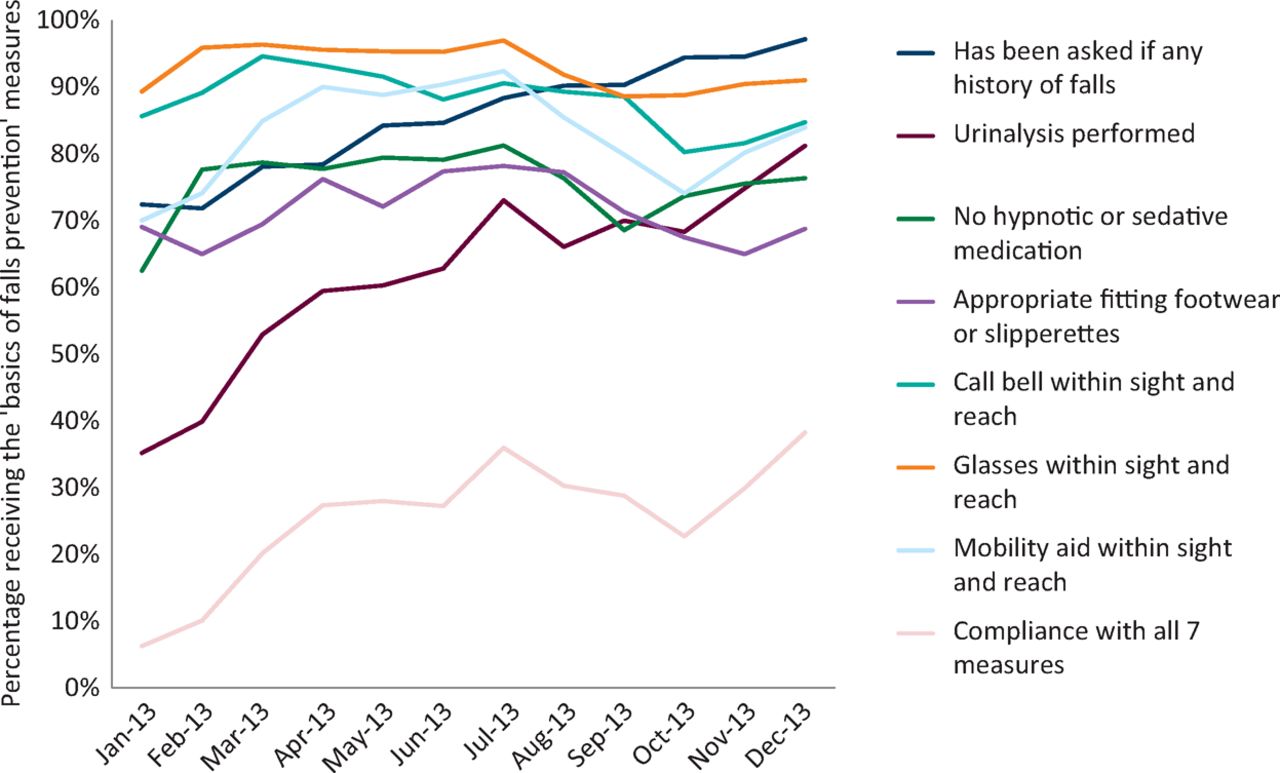
In total, 9,679 patient episodes were recorded over the year. Overall compliance with most measures improved (Fig 1). The percentage of all patients who received all 7 measures of inpatient falls prevention had risen from 6% to 38%. Specifically, 5 of the 7 measures had shown an absolute percentage improvement in compliance (falls history 25%; urinalysis 46%; glasses within reach 2%; walking aid within reach 14%; no sedative medications 14%), though 2 of the measures had no significant change from baseline (call bell within reach 1.0%; appropriate footwear 0%).

Compliance with the ‘-Bundle for all patients’ January–December 2013 (n = 9,679).
Bundle for older and more vulnerable patients
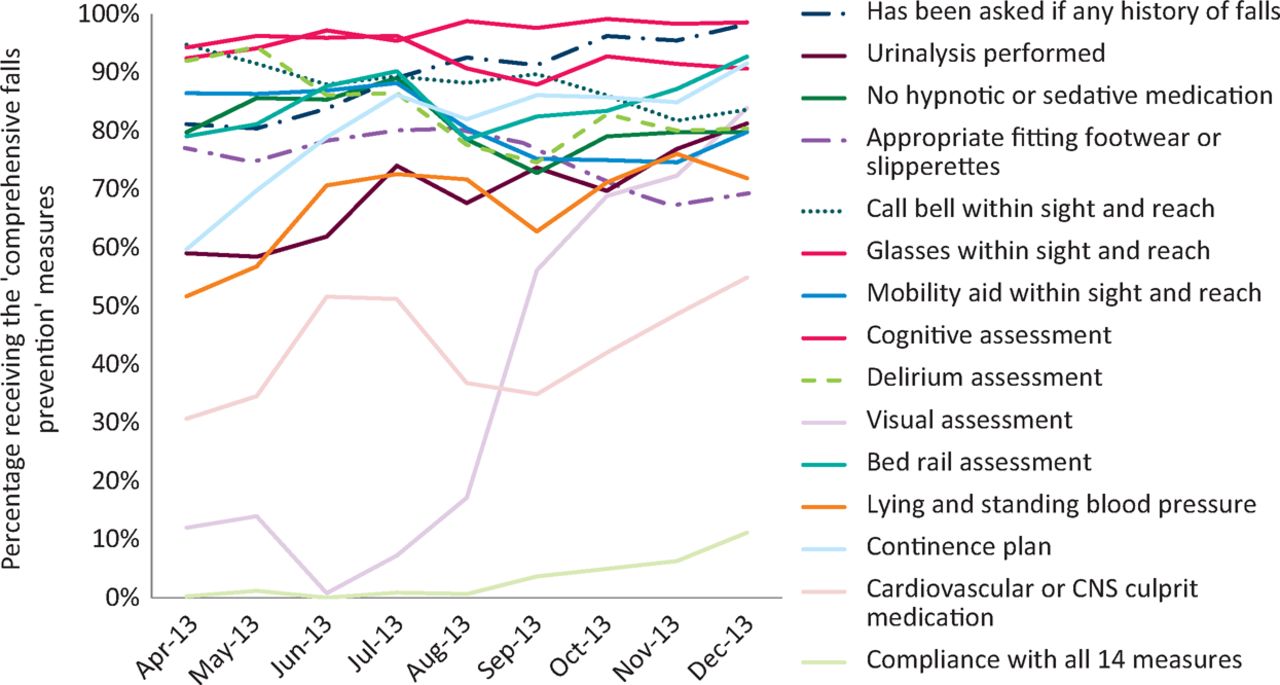
3,276 patient episodes were recorded over 9 months (Fig 2). The percentage of patients who had received all 13 measures of inpatient falls prevention had risen from 0 to 11%. All but one of the additional measures had shown improvement in compliance (dementia assessment 7%; visual assessment 72%; bedrail assessment 14%; postural blood pressure recorded 20%; continence assessment 32%; cardiovascular/CNS culprit medication assessment 24%; delirium assessment 12%).

Compliance with the ‘Bundle for older and more vulnerable patients’ April–-December 2013 (n = 3,276).
Bundle for after a fall
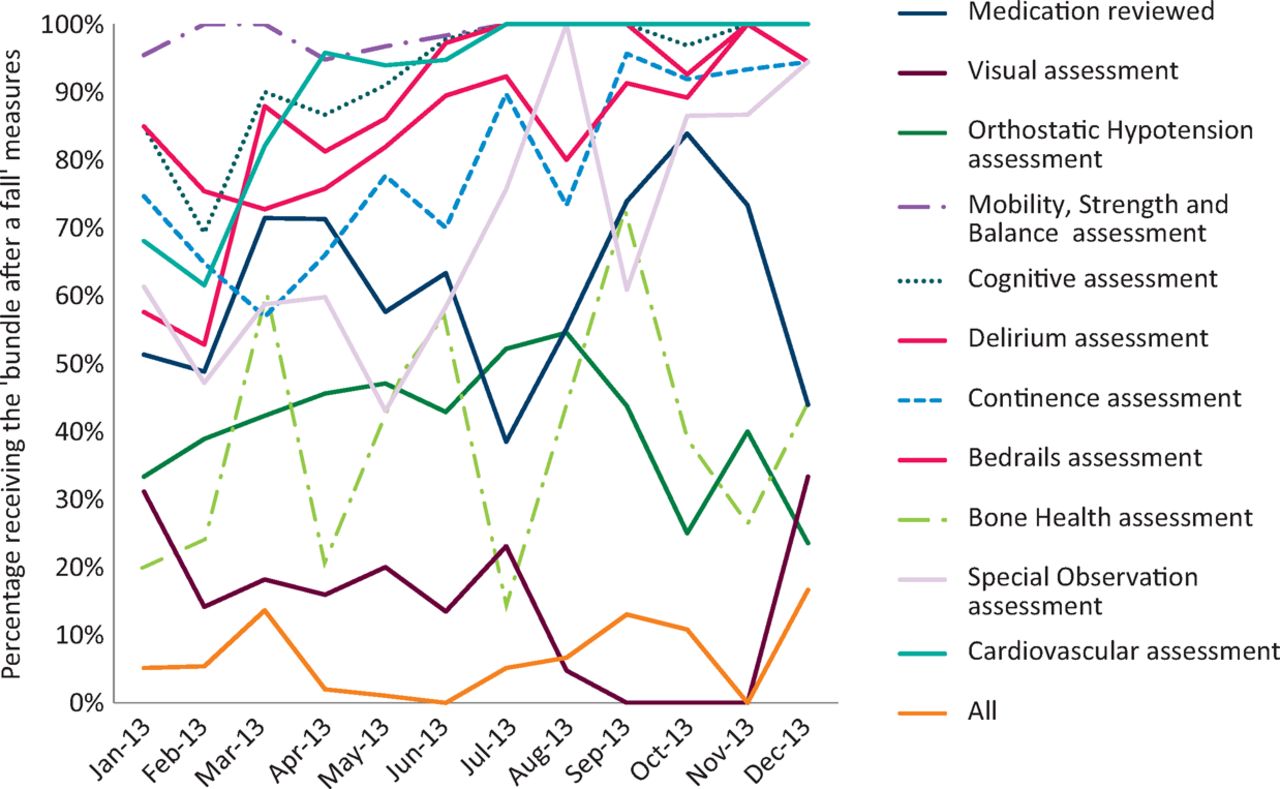
687 inpatient falls were reviewed over the year (Fig 3). 9 of 11 post fall measures had improved (mobility, strength and balance review 5%; impaired cognition review 15%; delirium review 42%; continence frequency/urgency review 19%; risk vs benefit bedrails review 9%; bone health/osteoporosis/fracture risk review 24%; special observation consideration 33%; impaired vision review 2%; cardiovascular assessment 32%) while 2 measures declined (medication review 9%; orthostatic blood pressure review 9%). The percentage of all patients who had received all 11 post fall measures had risen from 5 to 17%.
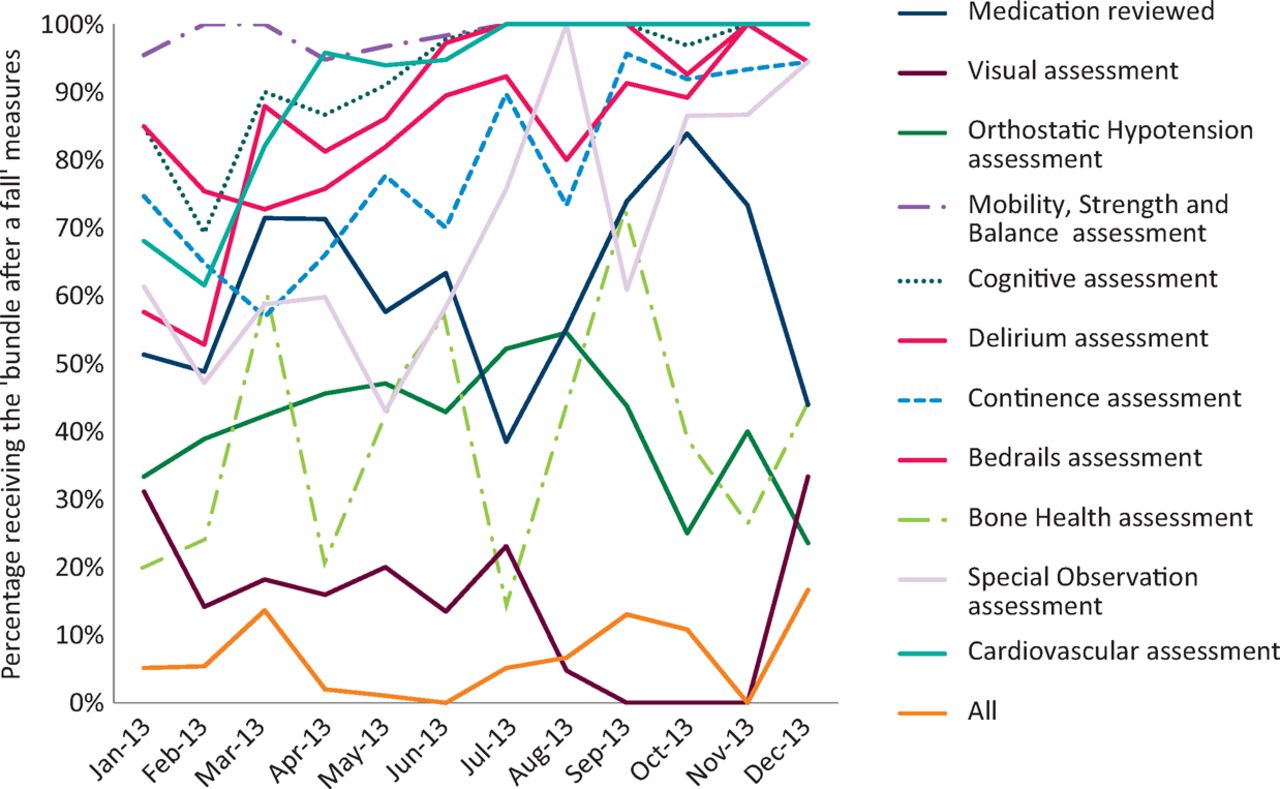
Compliance with the ‘Bundle for after a fall’ January–December 2013 (n = 687).
Falls data
The total number of inpatient falls fell by 6% in 2013 compared to 2012 (3,386 vs 3,607). Similarly the number of patients who suffered moderate, serious or catastrophic harm as a result of an inpatient fall (death, fracture, subdural haematoma etc) fell by 4% (157 vs 150).
However the number of falls/1,000 bed days rose by 0.3% (9.1 to 9.4).
Conclusions
This is the first report on the effectiveness of the RCP FallSafe care bundles, when applied to all patients in a NHS foundation trust, to reduce inpatient falls. It demonstrates that the RCP FallSafe care bundles can be applied across a wide range of inpatient specialties, including acute geriatrics, geriatric rehabilitation and orthogeriatric wards, where older and more vulnerable patients are typically found and also which report the highest number of inpatient falls.
In order to implement the many measures in the RCP FallSafe care bundles the whole multidisciplinary team needed to be informed and involved, including the nursing staff, medical staff, therapists, pharmacists, estates and management. This also meant adaptation of some of the measures to make it practical to apply them across all wards and also easily auditable without any additional resources.
Some measures were already in place as part of a trust CQUIN (eg dementia, delirium assessment) or care of the elderly pathways (eg continence), and required no additional resources or time from the falls team, while others required additional education (eg walking aids) or were controversial and met with resistance from some medical teams (eg performing a routine urinalysis for fears of the indiscriminate use of antibiotics).
Some measures deserve specific comment. Continuous non-invasive beat-to-beat blood pressure monitoring is now the gold standard for accurately detecting postural hypotension in routine clinical practice.9 While this was available, it could not be provided everywhere in the trust. Using a manual sphygmomanometer requires specific training and is now no longer routinely performed on the wards due to the presence of automated blood pressure devices. We had therefore compromised and developed a protocol that could be applied on all wards, to all applicable patients and that would not be dependent on a few skilled staff that could use still use a manual sphygmomanometer. Therefore HCAs, after training and using standard automated blood pressure monitors, were asked to record three blood pressure measurements within the 3 minutes of standing to assess for evidence of postural hypotension. If there was a strong clinical suspicion for postural hypotension not detected by this method then patients could be referred to the falls team for consideration of non-invasive beat-to-beat blood pressure monitoring.
It was recognised, that there are patient groups admitted to hospital where it is entirely appropriate to prescribe sedatives, or for them to be taking potentially ‘culprit’ cardiovascular or CNS medication. A ceiling effect was therefore reached early in the year, caused by the characteristics of the patients admitted, for these two measures. We did not assess whether medications were reviewed or adjusted; however work is ongoing with the pharmacy medication reconciliation teams to highlight these medications, so that the individual clinical teams can consider change if they feel appropriate.
There were also logistics problems with some measures. After an initial improvement in appropriate footwear, the supply of slipperettes ran out in the middle of the year and remained problematic for the rest of the year. This led to a fall in use of slipperettes and an increase in patients with no suitable or inappropriate footwear. A regular supply of slipperettes has subsequently been funded by the trust and education regarding what constitutes suitable footwear communicated to patients, carers and staff through training and a publicity campaign.
Where required, providing patients with a suitable walking aid within 24 hours of admission to hospital, also was problematic. Ambulances tend to bring acutely ill patients into hospital without their usual walking aids, and therapy services, which can assess and provide suitable walking aids, are often limited at the weekend.
Although the trust has had a robust nurse-led patient incident reporting culture (reinforced during mandatory training and post-fall follow up) for many years, and we were confident all falls were reported, because we did not use the FallSafe under-reporting measure5 we cannot confirm whether this was actually the case. Therefore changes in reported falls may reflect more complete reporting. NHFCT has consistently reported higher than average inpatient falls/1,000 bed days data when compared nationally1,2 and we feel in some part this is due to the reporting culture. Falls/1,000 bed day rates are similar to that reported in wards equivalent to the FallSafe wards at the end of the intervention.5
The number of inpatient falls can be affected by many factors including environmental, staff and patient factors. A dedicated falls team is essential to provide the necessary training and support to implement the FallSafe care bundles. We modified our mandatory training to incorporate e-learning packages, work books and ward-based training to address the differing needs of the ward staff. A falls liaison nurse was appointed on each ward as ward ‘falls champion’ to help disseminate information and act as a learning resource for other ward members. During the study period ‘intentional rounding’ has been implemented by the trust, additional nursing staff rostered overnight and one-to-one nursing guidance implemented.
The trust has a high percentage of single rooms and non-visible bed spaces. The falls team have looked at task lighting, flooring, bed rails, one-way glides, crash mats, and bed and chair alarms.
Pressures to reduce length of stay and hospital admissions has also led to a marked increase in the use of ambulatory care for the ‘fitter’ patients; therefore patients who are admitted to hospital tend to be frailer, have more comorbidity and be at a higher risk of an inpatient fall. We also had a number of ward closures, ward reconfigurations and long periods where patients were being ‘boarded out’ from their usual ward due to bed pressures. All these factors could contribute to the increased falls/1,000 bed days observed.
Compliance with the measures recommended by the FallSafe care bundles, has improved following regular spot audit and training. This has led to an overall reduction in the number of inpatient falls. Despite this, in the real world of changing patient demographics, ward closures and the increasing use of ambulatory care, the number of falls/1,000 bed days has increased. FallSafe advocates, falls team, trust board members and clinical commissioning groups should be aware of possible confounding influences and limitations when setting possible target measures for inpatient fall reduction.
- © Royal College of Physicians 2015. All rights reserved.








{kind=link}
{kind=link}
{kind=link}