
ABSTRACT
A 55-year-old man presented with acute ST-elevation myocardial infarction. He received rescue angioplasty with one drug eluting stent. He developed marked breathlessness and haemoptysis two days later. Investigations led to the diagnosis of pulmonary haemorrhage, possibly from pneumonitis caused by ticagrelor. He was successfully managed with high-dose steroids and ticagrelor was replaced with clopidogrel. On stopping the steroids a month later, mild haemoptysis recurred and this was managed conservatively. Pneumonitis and pulmonary haemorrhage is rarely reported with acute myocardial infarction, but poses serious challenge to the patient and the clinician. Diagnosis may be delayed as breathlessness can occur due to myriad causes after myocardial infarction. Interrupting dual anti-platelet therapy after angioplasty could lead to devastating stent thrombosis.
Case presentation
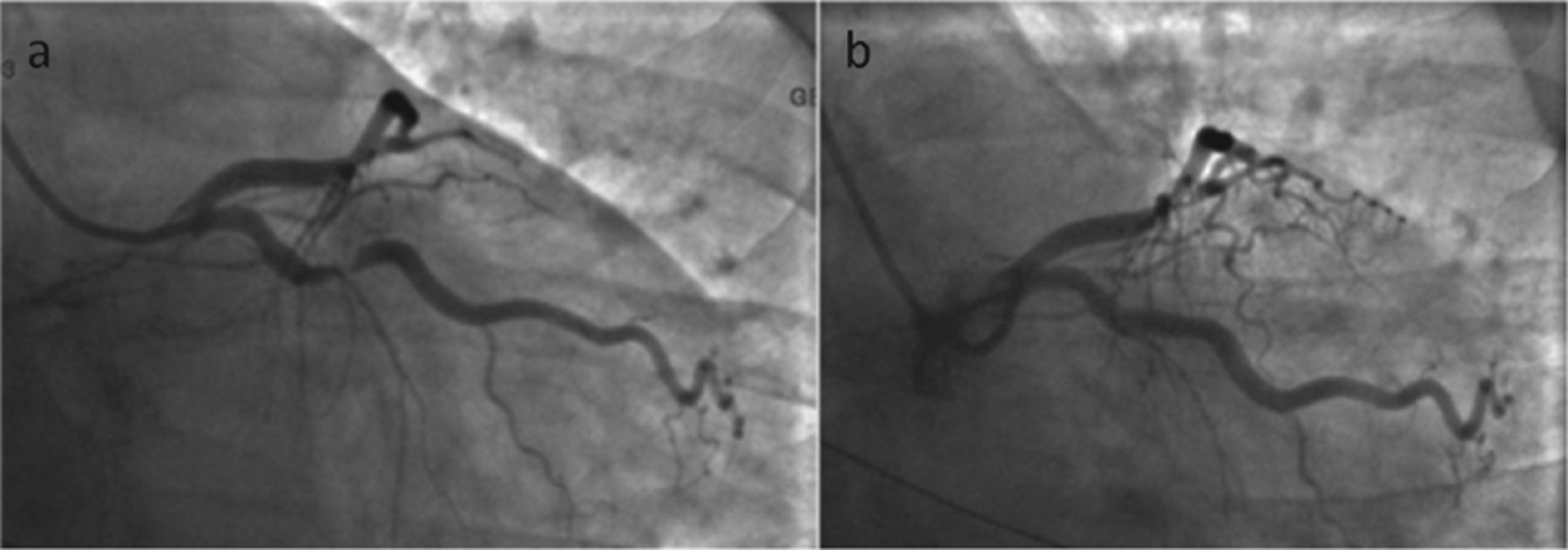
A 55-year-old hypertensive man developed chest pain while working on an off-shore oil station. Electrocardiogram (ECG) showed acute lateral ST-elevation myocardial infarction. He was treated with tissue plasminogen activator tenecteplase, low molecular weight heparin and aspirin. The ECG changes and chest pain completely resolved. He was transferred to our centre for coronary angiography on the same day. Prior to the procedure he was given ticagrelor 180 mg. Coronary angiogram (Fig 1) showed severe thrombotic stenosis in a large obtuse marginal branch of the left circumflex artery and diffuse distal left anterior descending artery disease. Heparin 4,000 IU and tirofiban were administered and the stenosis in the obtuse marginal artery was successfully treated with a 4.0x16-mm drug eluting stent. Following the procedure he was treated with aspirin 75 mg od and ticagrelor 90 mg bd. Later that day, he was also started on bisoprolol 1.25 mg od and simvastatin 40 mg od.

Coronary angiography-AP caudal image. a) Severe stenosis of the obtuse marginal artery; b) after drug eluting stent insertion
On day 2, the patient complained of productive cough and had low-grade temperature of 38°C. Cardiovascular and respiratory examination was unremarkable. Chest X-ray showed clear lung fields (Fig 2). Blood cultures were negative. An echocardiogram showed mildly impaired LV systolic function with a pulmonary artery systolic pressure of 42 mmHg (reference <36 mmHg).
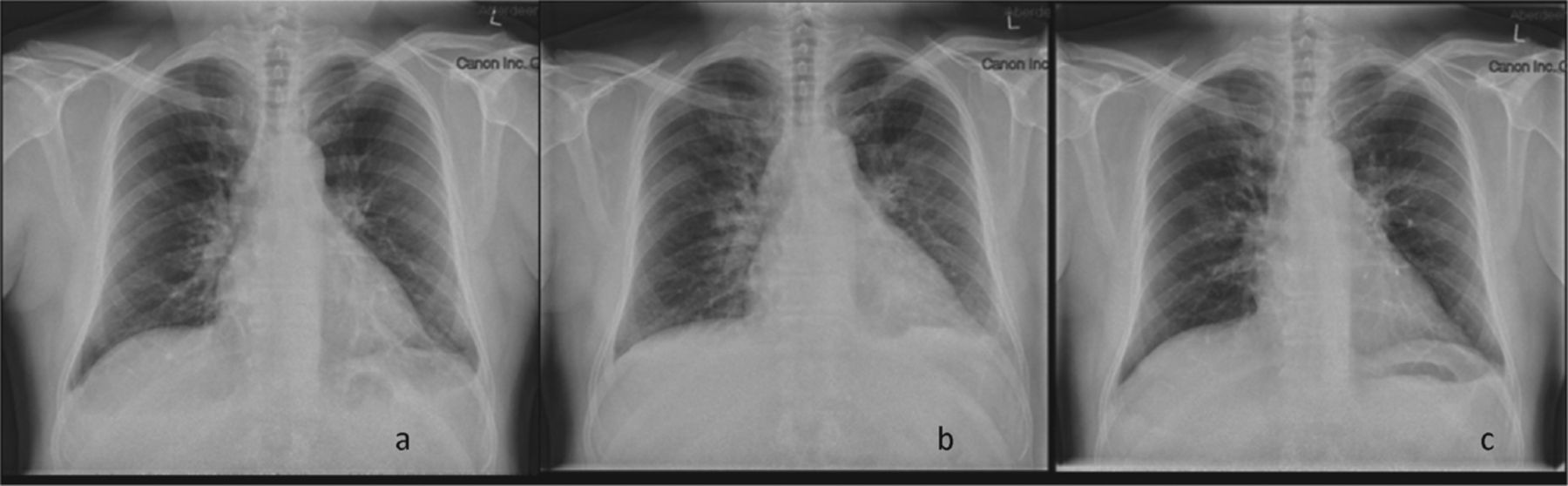
Chest X-rays. a) Day 2: largely clear lung fields; b) day 4: hazy peri-hilar shadowing and small left pleural effusion; c) day 15 near complete resolution.
On day 3, he was started on amoxicillin for suspected chest infection but with little symptomatic benefit. Over the following few days, he developed significant hypoxia (PaO2 was 7.27 kPa on 5 L O2 (Reference 11–13 kPa on air)), haemoptysis and bilateral lung crepitation. Clarithromycin was added to the treatment regime. Repeat chest X-ray showed bilateral hazy perihilar shadowing with some left basal pleural effusion.
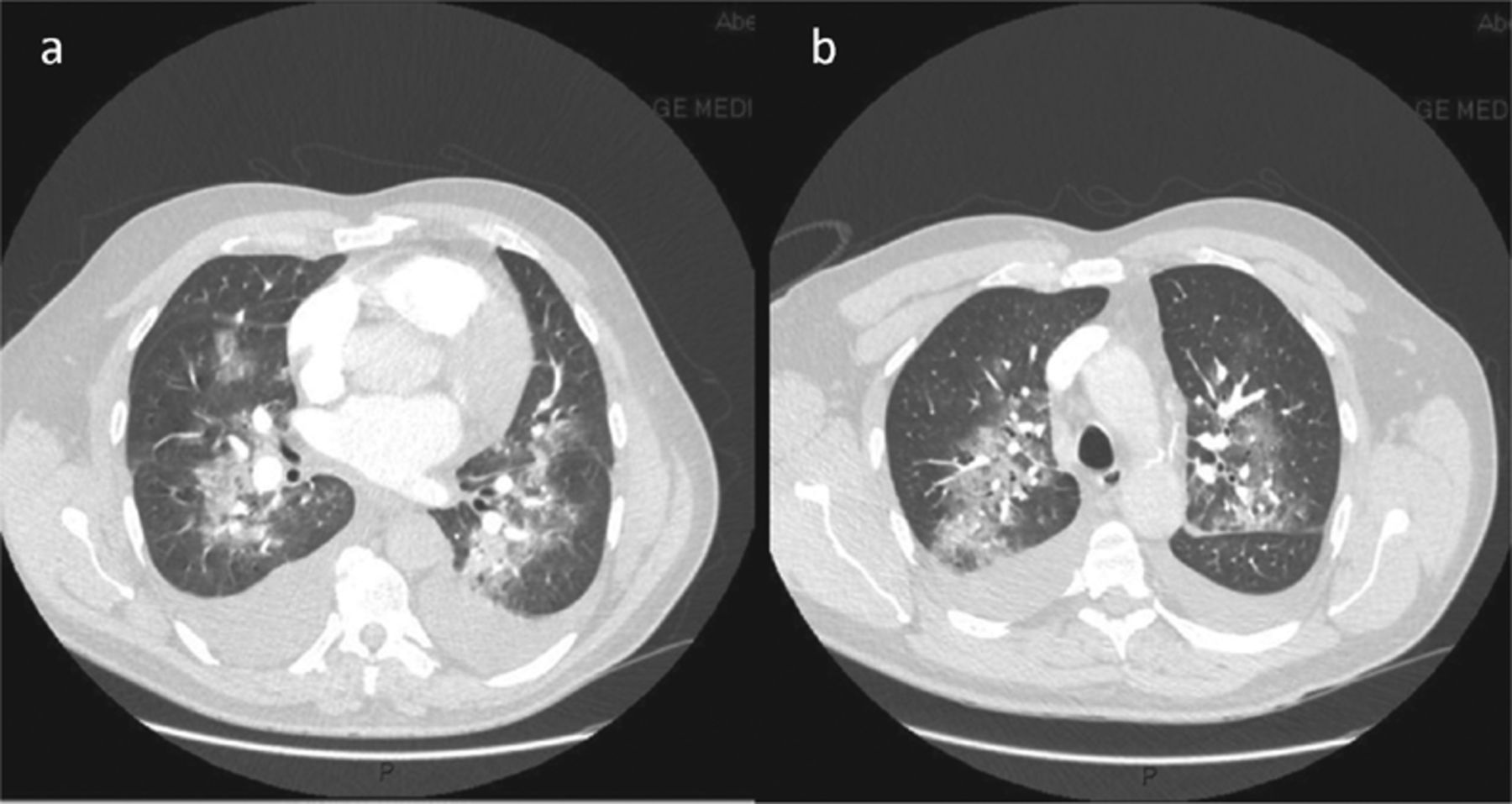
A computed tomography (CT) pulmonary angiogram was done on day 5 and this showed bilateral patchy ground-glass opacification in central distribution in keeping with inflammatory change and pulmonary haemorrhage (Fig 3).
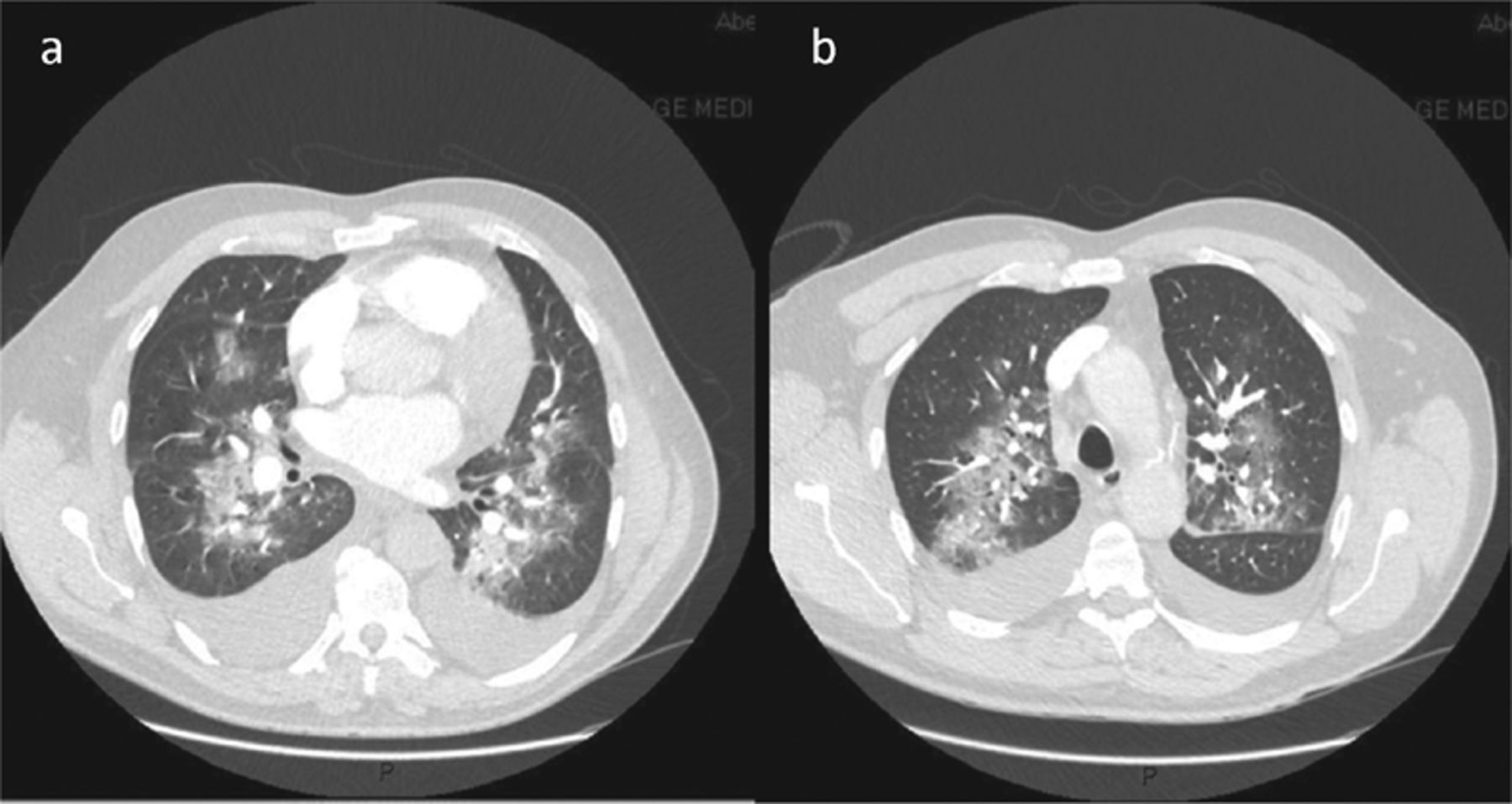
Computerised tomography pulmonary angiogram was performed which ruled out pulmonary embolism, but showed pulmonary haemorrhage and inflammation.
A repeat ECG showed rapid rise in central pulmonic pressure to 70 mmHg with no change in LV function. Haemoglobin fell from 153 to 123 g/L (reference >126 g/L). Prothrombin time was marginally prolonged at 13.2 sec (reference range 10–12.6 sec) but activated partial thromboplastin time was normal. C-reactive protein (reference 5 mg/L) increased from 4 mg/L on day 1 to 293 mg/L on day 6. He was reviewed by the respiratory and renal teams. Anti-neutrophil cytoplasmic antibody, anti-nuclear and anti-glomerular basement membrane antibodies were negative and complements C3 and C4 were within normal limits. A diagnosis of pneumonitis and secondary pulmonary haemorrhage was made; ticagrelor was suspected to be the cause.
Ticagrelor was replaced with clopidogrel 75 mg/day. He was started on prednisolone 60 mg/day at day 5. Over the course of the following few days, the haemoptysis and shortness of breath resolved. His clinical improvement was mirrored by improvements in the inflammatory markers (Fig 4). Chest X-ray changes progressively resolved with near complete resolution on day 15. He was discharged home on day 15, with a reducing course of prednisolone for one month. After stopping his steroid regimen, he presented with recurrence of haemoptysis. CT chest revealed a mild bronchiolitis pattern and a bronchoscopy was normal. A CT after 6 months was normal. He managed to continue on dual-antiplatelet therapy during this period without interruption. This is reported to the Medicines and Healthcare products Regulatory Agency (MHRA) as a probable adverse effect of ticagrelor.

a) blood results; b) observations. a = morning; b = afternoon; c = evening.
Patient's perspective
A couple of days after angioplasty, I developed a bit of a dry cough, suffered loss of voice and hoarseness and started to cough up small amounts of blood in my sputum. My chest felt as though it was rattling and I was bringing up more blood in my sputum and had difficulty breathing. I can also recall the foul taste in my mouth and found I needed to regularly rinse my mouth with antiseptic mouthwash to relive the taste. My partner asked ‘what is the taste like’ and I recall my reply was simply ‘death’ as it was hard to describe.
Discussion
This is a case report of a rare but potentially life-threatening pneumonitis and pulmonary haemorrhage. The patient was initially treated with thrombolysis and anti-coagulant therapy. The biological half-life of tenecteplase is 65–132 minutes,1 heparin is 60 minutes2 and tirofiban is 9 hours. Hence, it seems unlikely that these agents caused the pulmonary haemorrhage on day 3. The rapid improvement on steroids, and mild recurrence on steroid withdrawal, supports an immune mechanism for this complication. All other medications apart from ticagrelor were continued further, suggesting ticagrelor as a possible causative agent. There has been one previous case report of ticagrelor-induced pulmonary haemorrhage, reported by Whitmore et al.3
Dual anti-platelet therapy is routinely advised for patients with acute coronary syndrome. Studies from the late 90s and early 2000s showed dual antiplatelet therapy to improve outcomes in patients undergoing percutaneous coronary intervention after acute myocardial infarction,4,5 but has to be balanced against the potential bleeding risk.
Ticagrelor, a reversible and direct acting oral adenosine diphosphate receptor antagonist, is an anti-platelet agent used in the treatment of patients presenting with acute coronary syndrome. It was found to significantly reduce mortality and bleeding compared to clopidogrel in the treatment of acute coronary syndrome (ACS) in the multicentre randomised controlled PLATO trial.6 These favourable outcomes of ticagrelor compared to clopidogrel have been demonstrated in all ACS patients regardless of whether or not they have undergone percutaneous coronary intervention.7 Hence, ticagrelor is currently the most widely used second anti-platelet agent in this group of patients.
Pulmonary haemorrhage is a rare complication after acute myocardial infarction. The differential diagnosis of pulmonary haemorrhage may include pulmonary oedema, pneumonia and pulmonary embolism. Other causes of pulmonary haemorrhage include autoimmune conditions, infections (viral or fungal), other cardiac disorders (such as mitral stenosis), idiopathic pulmonary haemosiderosis, and coagulopathy caused by drugs and diseases. Pulmonary haemorrhage secondary to drug reactions have been described with amiodarone, infliximab and propylthiouracil.8,9 The symptoms, signs and X-ray changes of pulmonary haemorrhage are non-specific. Diagnosis is by CT imaging and broncho–alveolar lavage.
The natural history of this condition and success of steroid therapy if delayed are unclear. In the case report by Whitmore et al, the patient presented 10 days after starting treatment with ticagrelor. He had more significant haemoptysis than our patient and this persisted even after replacing ticagrelor with clopidogrel. As a result of this, dual anti-platelet therapy was completely withdrawn and the patient underwent coronary artery bypass surgery (as acute stent thrombosis could occur without dual anti-platelet therapy). Lung biopsy at the time of surgery showed alveolar septal wall fibrosis with inflammatory cell infiltrate, indicating that this is a rapidly progressive condition.
In summary, pneumonitis and pulmonary haemorrhage are rare but serious adverse effects after myocardial infarction. Awareness among clinicians that ticagrelor could cause this serious adverse effect could lead to early diagnosis. Steroid therapy is one potential avenue.
Learning points
Clinicians should have a high index of suspicion for diagnosis for diagnosing pulmonary haemorrhage after myocardial infarction.
Ticagrelor could be a potential cause.
High-dose steroid regime seems to be a therapeutic option.
- © Royal College of Physicians 2015. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.