
ABSTRACT
Chronic hepatitis caused by hepatitis C virus infection is one of the leading causes of liver cirrhosis and hepatocellular carcinoma globally. Over the last few years, there have been significant advances in our understanding of the immunopathogenesis of this infection, as well as revolutionary developments in the therapeutic armamentarium. The introduction of a number of new oral antiviral agents is already delivering major benefits to patients as they are generally well tolerated and are associated with excellent response rates in the majority. Nonetheless, a number of clinical scenarios remain challenging and research is ongoing in these areas. In this update, we review developments in both basic as well as translational research in the field.
Background
It is estimated that there are over 185 million people infected with hepatitis C virus (HCV) globally. Acute infection leads to chronicity in the majority of people (80–85%) with only a minority able to resolve the infection spontaneously. Persistent HCV infection is associated with the development of liver cirrhosis, hepatocellular cancer and liver failure, with approximately 500,000 deaths per year attributable to these causes. HCV has now become the most common cause of death in HIV-positive patients on therapy.1 However, new developments in antiviral drugs in the last 2–3 years have transformed the outlook for this disease.
Virology
HCV is an enveloped positive-strand RNA virus that encodes a single polyprotein that is processed into three structural and seven non-structural proteins. It displays enormous genetic diversity, which results from a high mutation rate and a high replication rate.2,3 Comparison of nucleotide sequences and phylogenetics of global HCV sequences has revealed seven different strains or genotypes differing by 30–35% of nucleotide sites. Within each genotype, there are further divisions into subtypes (more than 67 subtypes) that differ by 10–15%.4 Genotypes 1, 2 and 3 are widely distributed globally and are the most common genotypes in the west. A different pattern of sequence diversity is observed in parts of Africa and South-East Asia. For example, infections in Western Africa are typically caused by genotypes 1 and 2, while genotypes 3 and 6 are highly prevalent in Southern and Eastern Asia. In these regions, a remarkable diversity of subtypes is observed and it is believed that these patterns indicate that HCV has been endemic in these areas for a considerable length of time. By contrast, infection in Western countries is considered to be a more recent phenomenon, likely attributable to widespread parenteral exposure through blood transfusions and intravenous drug use. In the UK, the most prevalent genotypes are 1 and 3.1,4
Since the discovery of HCV (originally described as non-A non-B hepatitis) in 1989, substantial progress has been made in developing systems to dissect the viral life cycle, and major advances in our understanding of host–virus interactions and treatments has occured. In vitro culture systems began with sub-genomic replicons which required specific hepatocyte cell lines and tissue culture adaptation. Further work was facilitated by the discovery of the Japanese genotype 2 strain (JFH-1) which could support full replication cycles and produce infectious virions in vitro, albeit these systems also rely on modified hepatocyte cell lines. To date, these systems have facilitated a number of important discoveries including the identification of key cell entry factors such as CD81, scavenger receptor B1 and claudin-1. They have also helped to define the impact of antivirals in vitro demonstrating the generation of escape mutations in response to selection pressure.5 Recently, the generation of complete infectious viral life cycles in a mouse model with genetically humanised mice presents exciting new opportunities for evaluating vaccines and treatments.6
Epidemiology
Transmission of HCV is primarily through parenteral exposure. Infections occurring through receipt of contaminated blood products and through the use of contaminated healthcare-associated paraphernalia are still potentially common in certain countries. In the western world, since the advent of blood product screening, transmission has mainly occurred through intravenous drug use, although more recently there has been significant outbreaks of infection among HIV-positive men who have sex with men (MSM) in European, Australian and North American cities, with transmission linked mainly to high-risk sexual behaviours, as well as intranasal and intrarectal drug use.7 Indeed, a 15-year review of HCV seroprevalence data among MSM attending a large sexual health clinic in the Netherlands demonstrated an increase in prevalence from 5.6% in 1995 to a peak of nearly 21% in 2008.8 Genetic analysis of viral sequences from HIV-positive MSM acutely infected with HCV revealed several clusters of infection with different genotypes indicating several introductions of the virus into the MSM population and transmission clusters in MSM networks. Notably, in one study up to 25% of MSM treated for infection became reinfected within two years highlighting the scale of the problem.9
Immunology
The factors that determine the outcome of infection have been extensively investigated previously. Critical roles for the adaptive and innate immune response have been identified through both genetic and immunological studies. Genetic studies have linked clearance to certain human leukocyte antigen (HLA) alleles. For example, HLA-B*27 and HLA-A*03 have been linked to spontaneous clearance in a large single-source outbreak of HCV occurring in Ireland as a result of anti-D immunoglobulin contamination, while HLA-B*57 has been identified as protective in other populations.10,11 Further work on the immunological basis for these associations has identified critical immunodominant T-cell epitopes that are targeted in individuals possessing the protective alleles. These particular epitopes appear to have a high genetic barrier to the development of escape mutations which is proposed as the likely mechanism.12,13 Genetic studies also support a crucial role for the CD4+ T-cell responses. A number of genetic studies have identified very clear-cut associations between certain HLA class-II alleles and outcomes (HLA-DQB1*0301), and a recent large genome-wide association study (GWAS) also linked viral clearance with the HLA class II locus.10,14,15
A number of studies have also identified a major role for the innate immune response. Polymorphisms associated with the innate interferon-lambda 3 gene (IFNL3; also known as IL28B) have been linked with viral outcome in genotype-1 infected persons.15,16 This innate IFN is a cytokine possessing antiviral and immunomodulatory activity, however the specific mechanism that underpins its effect in HCV is not fully understood yet. Killer immunoglobulin receptor (KIR) genes which control the natural killer cell state of activation have also been linked to viral outcome.17 Our group has recently performed an analysis investigating the relative contribution of both the innate and adaptive immune responses on HCV outcome. We studied the collective impact of HLA and innate immune genes on viral outcomes in an Irish cohort of women who had been infected from a single source. The results indicate distinct and separate roles for both HLA and IL28B/KIR genes in the prediction of outcome. We found that these effects were not interactive but were additive, a finding echoed in a GWAS analysis.15,18 These results collectively indicate significant and independent contributions from both the innate and adaptive immune responses in the control of HCV infection.
Development of vaccines
With the advent of highly effective direct-acting antiviral drugs (DAAs), the role of a HCV vaccine in curtailing the current HCV epidemic has been placed into sharp focus. The high costs of DAAs however are likely to limit their widespread use in developing countries and even in high-income countries, and potential re-infection after successful treatment remains a significant concern especially in high-risk populations such as persons who inject intravenous drugs and MSM. In these populations, a preventative vaccine retains the potential to dampen the epidemic and protect key at risk groups from reinfection.
The highly diverse nature of the HCV means that a conventional vaccine targeting the highly variable envelope protein is unlikely to be effective, although if broadly cross-reactive neutralising antibodies could be elicited, this would be an ideal approach. As a consequence, work has been focused on the development of a T-cell vaccine. Evidence from human and animal studies has already indicated a crucial role for CD4+ and CD8+ T-cell responses in the clearance of infection. These studies have shown that after a primary infection, rapid recall of the memory T-cell responses leads to reduced viraemia and a higher likelihood of spontaneous resolution.19–21 The aims of a T-cell vaccine therefore would be to recapitulate these responses thus directing towards a more successful response rather than preventing infection in the first instance.
A number of different approaches have been used to try to induce protective T-cell responses, including peptide, DNA and viral vector-based vaccines; the latter use manipulated viruses to deliver antigenic material to host cells.21 Initial studies on chimpanzees using an adenoviral-based vaccine containing the non-structural region of the HCV genome demonstrated induction of potentially protective T-cell populations. Vaccinated animals showed strong T-cell responses and rechallenge experiments showed that these responses were briskly reactivated linking with viral control in 4 out of 5 animals.22 Phase-I safety and immunogenicity trials of two preventative vaccines are now available in humans. Barnes and colleagues used a prime-boost regimen of recombinant adenovirus vector (ChAd3 and Ad6) and modified vaccinia Ankara (MVA) vaccines encoding non-structural protein (NS)3–NS5 in healthy volunteers. These trials demonstrated that the vaccines induced robust and functional CD4+ and CD8+ T-cell responses to multiple antigenic sites, and that these responses were sustained for up to one year.21,23 Phase-II studies are currently underway in the USA.
Treatment
Eradication of infection (sustained virologic response (SVR)) is the goal of therapy and such cure is associated with both limiting and even reversal of liver disease progression. Until recently, therapies for all genotypes required the administration of IFN-α and ribavirin, but success rates were modest (50% success for genotype 1) and treatments were associated with considerable adverse effects particularly for those with advanced liver disease. The development of a cell culture system accelerated drug discovery and development and in the last number of years there has been a revolution in the development of novel antiviral treatments that target different areas of the viral life cycle. There are three main drug targets of these specific DAAs – the protease, NS5A and NS5B (the viral RNA polymerase) proteins.
The first wave of these drugs emerged in 2011 with the licensing of the first generation protease inhibitors (PIs) (‘-previrs’). These agents target NS3–4A by binding to the catalytic site of the enzyme and thus inhibit HCV polyprotein production. Telaprevir and boceprevir were licensed for use in conjunction with IFN and ribavirin for genotype-1 infected patients. These agents improved the rates of SVR from 50% to appoximately 70%. Adverse effects were relatively frequent with this regimen and included anaemia and rash. The next wave of PIs includes simeprevir (recently licensed), faldaprevir, asunaprevir and ABT-450, among others. Further PIs are in development aiming to increase genotypic cover and to raise the genetic barrier to resistance.24,25
Inhibitors of the RNA-dependent RNA polymerase enzyme NS5B (‘-buvirs’) can be divided into nucleoside/nucleotide and non-nucleoside inhibitors. Nucleoside/nucleotide inhibitors act as a false substrate for the RNA polymerase enzyme which leads to viral chain termination. Sofosbuvir and dasabuvir are examples of this drug class. Importantly, these drugs exhibit pan-genotypic activity and possess a high barrier to the development of resistance. Also in development are non-nucleoside inhibitors of the RNA-dependent RNA polymerase enzyme function, which act by binding to the surface of the protein, altering its conformation and limiting further viral replication.25
NS5A inhibitors (‘-asvirs’) bind to the NS5A protein and interrupt the development of the replication complex, interfering with the assembly and release of viral particles. First-generation NS5A inhibitors include daclatasvir, ledipasvir and ombitasvir, and demonstrate consistent activity against diverse genotypes. Some resistance is observed but further agents are in development with extended genotype coverage and enhanced resistance barrier.24,25
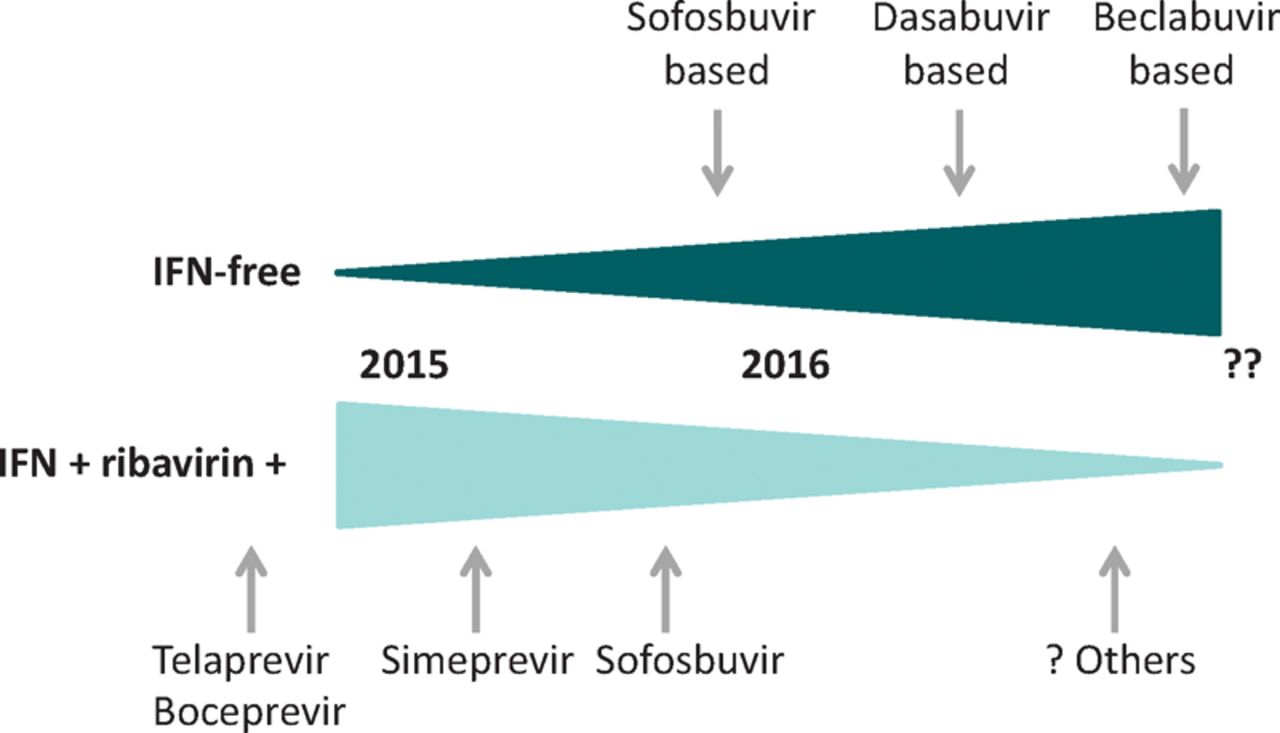
Current treatment strategies for treating HCV include combining the novel agents with IFN and ribavirin or new all-oral ‘IFN-free’ combinations of DAAs. Success rates with these approaches have seen very high rates of SVRs in a number of recent trials in patients with different genotypes, treatment histories and disease stages. As seen in HIV therapy, it is clear that combination drug therapy will remain critical in order to limit the development of resistance and enhance effectiveness. In addition, the very high current costs associated with the new oral antivirals means that it is likely that IFN-containing regimens will remain viable options for the time being (Fig 1).

Emerging HCV therapies. Cartoon illustrating the possible emergence of new therapies for HCV. The upper triangle shows DAA drugs only treatments, while the lower triangle shows IFN-based therapies. The shape of the triangle indicates the likely switch from IFN-based to IFN-free treatment. DAA = direct-acting antiviral; HCV = hepatitis C virus; IFN = interferon.
Recent NICE guidelines have recommended the use of these new agents in specific disease settings either as an all oral regime or in combination with IFN and/or ribavirin and new guidance will be emerging.26
The future of HCV – a UK perspective
While the era of DAAs and all-oral IFN-free therapy for HCV infection has clearly arrived, it brings with it many new challenges. The high cost of these therapies presents a major hurdle to the implementation of these highly efficacious regimes both nationally and internationally. In 2014, pending the approval by NICE of the new agents, the UK adopted an early access programme. Interim commissioning for HCV therapy by NHS England approved the use of sofosbuvir plus daclatasvir or ledipasvir with or without ribavirin for certain specified patient groups such as those with decompensated cirrhosis and those with a high risk of death. Following this, in 2015 approval for treatment of patients with compensated cirrhosis with an all oral antiviral regime was obtained and sofusbuvir is now available to those without cirrhosis in combination with conventional therapies (IFN and ribavirin). Discussions are now turning to the next wave of approvals for treatment with the focus remaining on a stratified approach which would ensure that those in most pressing need of treatment will be able to access these emerging regimens rapidly (Fig 2).
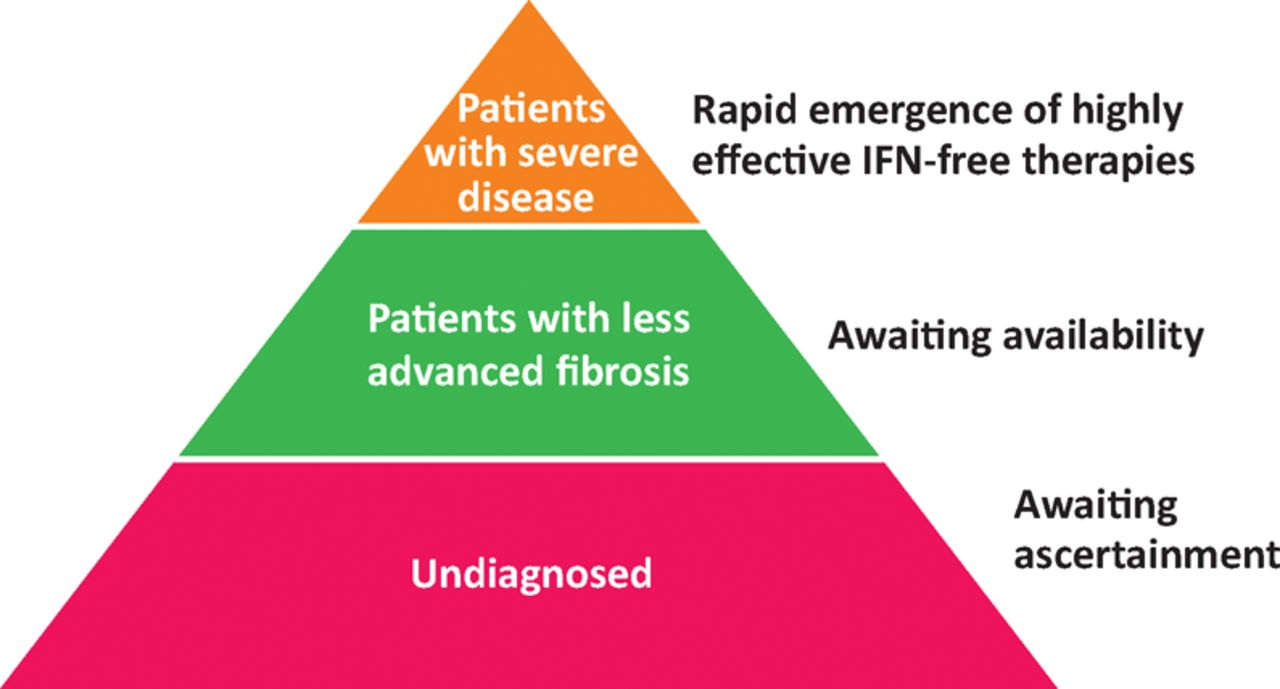
The pyramid or ‘iceberg’ of HCV therapy. Patients with severe disease at the top of the pyramid are already able to access the newest therapies. Those with less severe disease are awaiting these; however a large number of individuals remain undiagnosed and/or outside healthcare services. HCV = hepatitis C virus; IFN = interferon.
What about the future in HCV research and treatment? In 2012, the Medical Research Council, together with industrial partners, funded STOP-HCV, a consortium designed to use stratified medicine to optimise treatment in patients with HCV infection. Goals include studies of patients with genotype-3 infection to identify the best treatment options for this prevalent infection in the UK. Work within the consortium is focusing on understanding different host and viral genetic factors, biomarkers and pre-treatment variables, in order to optimise the use of the new treatments and to highlight the specific factors that are associated with treatment failure in special ‘difficult-to-treat’ groups such as those with cirrhosis.
In the longer term, as the new regimens emerge and hopefully become more readily available, attention must turn to identifying all those infected, and ensuring they have good access to healthcare. This is not a simple problem, but if tackled effectively this could have a huge impact on the spread of this disease as well as the outcome of infection. Hopefully a future update on HCV will be able to report on the success of this type of intervention.
Funding
PK is funded by the Wellcome Trust (WT091663MA), NIHR Biomedical Research Centre (Oxford), Oxford Martin School and MRC (UK) STOP-HCV.
- © Royal College of Physicians 2015. All rights reserved.








{kind=link}
{kind=link}