
Abstract
People with dementia have worse outcomes associated with hospital admission, are more likely to have interventions and are less likely to be offered palliative care than people without dementia. Advance care planning for care home residents has been shown to reduce hospital admissions without increasing mortality. Studies have shown that staff confidence in managing delirium, a common reason for admission, improves with training. A service combining education for care home staff and advance care planning for care home residents with dementia was introduced to care homes in Boston, UK. There were improvements in staff confidence in recognition, prevention, management and knowledge of factors associated with delirium and dysphagia. 92% of carers rated the service >9/10. Admissions fell by 37% from baseline in the first year and 55% in the second and third years. All but one resident died in the preferred place of care.
Introduction
People with dementia in care homes in the UK have a relatively short life expectancy. More than half of care home residents die within eighteen months of admission.1 People with dementia in care homes are more likely to be admitted to hospital with avoidable conditions, stay longer, and are more likely to be readmitted and to die than similar people without dementia.2 This is in keeping with broader evidence showing that people with dementia have poorer outcomes associated with hospital admission,3,4 are more likely to have interventions,4–6 and less likely to be offered palliative care than their counterparts without dementia.4 Although admission to hospital might offer access to the benefits of modern medicine, those who die in hospital may spend the last days of their life in a noisy, alien environment, cared for by strangers and separated from those who love them or know them.
Decisions to send a care home resident to hospital instead of providing home-based, conservative and palliative care may not reflect their wishes or be in their best interests: 60–67% of respondents in one survey in England said they would prefer to die at home if circumstances allowed.7
Not only may sending people with dementia from care homes to hospital be futile, hazardous, and unwanted, it is poor value for money. Hospital admissions in the UK cost between £2,352 and £3,779.8 Costs of services offering alternatives to hospitalisation might be less than the cost of admission and might represent cost-effective interventions.
Developing services to prevent avoidable hospital admissions in people with dementia requires understanding of why they occur. Possible contributors are the difficulty faced by doctors and care home staff in predicting medical crises and prognoses in care home residents2 and inadequate training about the management of the clinical features of end-stage dementia (such as dysphagia) and the medical crises that result (such as bronchopneumonia).2 Advance care planning and better training in the care of end-stage dementia are potential interventions that could help. Lack of mental capacity to make future treatment decisions in some people with dementia can be overcome by making such decisions in their best interests.12
Studies in Canadian9 and Australian10 care homes have shown that residents often prefer to be managed in the care home rather than be admitted, and that offering advance care planning to all residents reduces hospital admissions, without increasing mortality. Savings from hospital admissions offset costs of these schemes. In the Canadian study, total healthcare and implementation costs were significantly lower for residents in intervention homes compared with controls (CAD $3,490 vs CAD$5,239 respectively).9 Detailed economic analysis was not conducted in the Australian study, but previous economic analysis showed that ‘hospital in the home’ treatment was less than half the cost of hospital treatment.11
The role of anticipatory care of the clinical features of end-stage dementia in reducing hospital admission is less well evidenced. However, delirium, which often precipitates hospital admission, is known to be partially preventable.13
From this analysis, we proposed that care of residents with dementia in care homes could be improved at acceptable cost by a programme offering advance care planning by trained nurses, combined with staff training in management of end-stage dementia. Such a programme could prevent unwanted hospital admissions, increase the chance of residents dying in their preferred setting, and improve their terminal care.
With funding from a local charity, the Bromhead Medical Charity, we put such a programme for care homes into practice in Boston, Lincolnshire, UK in 2011 (the Bromhead Care Home Service (BCHS)).
This report's purpose is to provide guidance for others wishing to set up a similar service. The two objectives were to examine steps required to put this programme into practice, and to demonstrate the effects of doing so.
Methods
The BCHS intervention
Two registered general nurses with extensive experience in care of inpatients with dementia and frailty (SG and SP) were seconded to provide the BCHS for a two-year period, supported by a consultant liaison psychiatrist (GG). Prior to introduction of the pilot, agreement with the local provider organisation for primary care services (PCT), local general practitioners and care home managers was secured. In view of the regulations surrounding the sharing of personal and sensitive patient information, agreement from the appropriate authority (the PCT Caldicott Guardian) was obtained. Seven care homes in Boston, with 283 places registered for care of people with dementia, were offered the service, which started in March 2011.
An education programme was developed based on the Stop Delirium! material created by the University of Leeds14 and delivered via small group teaching 6–8 times in each care home to ensure all members of staff had participated. It encompassed information about dementia, especially late-stage dementia with reference to the Gold Standards Framework prognostic indicator guidance.15 In addition, with advice from a speech and language therapist, educational material was developed on eating, drinking and dysphagia. Care homes were given a reference file with the above information.
Residents with confirmed or suspected dementia were identified through registers kept by local primary care providers (general practices) and the care homes. Care home staff approached either residents or their families about advance care planning. They then asked interested residents’ general practitioners (GPs) to refer to BCHS. BCHS prioritised residents with the most severe dementia using prognostic indicators from a UK national programme to promote end-of-life care, the Gold Standards Framework prognostic indicator guidance.15 Nutritional and functional status, mobility, tissue viability, cognition and mental capacity were assessed with view to establishing a baseline against which future assessments could be compared. The demographic details of the residents are outlined in Table 1.
Demographic information for care home residents with advance care plans.
Advance care planning was conducted with residents or on a best interest’s basis with carers. This process usually involved several meetings with residents and/or their families or nominated carers or attorneys. Where agreed, an advance care plan was drawn up and a ‘do not attempt cardiopulmonary resuscitation’ order was completed. These were endorsed by the resident’s GP. Copies of these documents were filed in records held by the care home, GP and local hospital.
The effect of BCHS was evaluated by:
comparison of the care home staff confidence in recognition, prevention and management of delirium and dysphagia before and after training
comparison of care home staff knowledge of factors associated with development of delirium and dysphagia
a carer satisfaction survey was sent to all carers who agreed to participate
comparison between desired and actual place of death of residents
comparison of hospital admission rates for the year before and following introduction of BCHS
comparison of the costs of BCHS against potential savings through reduction in admissions using National End of Life Intelligence Network maximum and minimum admission costs.8
This work was done as a service evaluation, under governance arrangements rather than as a research project. Only routinely collected data were examined, and data were collected and analysed only by staff responsible for the service.
Staff confidence
In keeping with a prior survey of Stop Delirium!,14 staff confidence in the recognition, prevention and management of delirium was measured using an online Survey MonkeyTM questionnaire before and after training. Knowledge of causes and features of delirium was assessed using online questionnaires before and after training. The same model of evaluation was used for the dysphagia training programme. Fisher’s exact tests were used to establish the statistical significance of the results.
Carer satisfaction
All carers were invited to give their opinion on how care planning was conducted using a simple paper questionnaire.
Place of death
Data on deaths and place of death were collected from the care homes, and correlated with advance care plans.
Hospital admissions
Since there are seasonal changes in admission rates, data were collected from the local hospital information department for the calendar years before and after introduction of the service. All the care homes were within 5 miles of the local hospital, and there were no other secondary care providers within 28 miles.
Results
Education
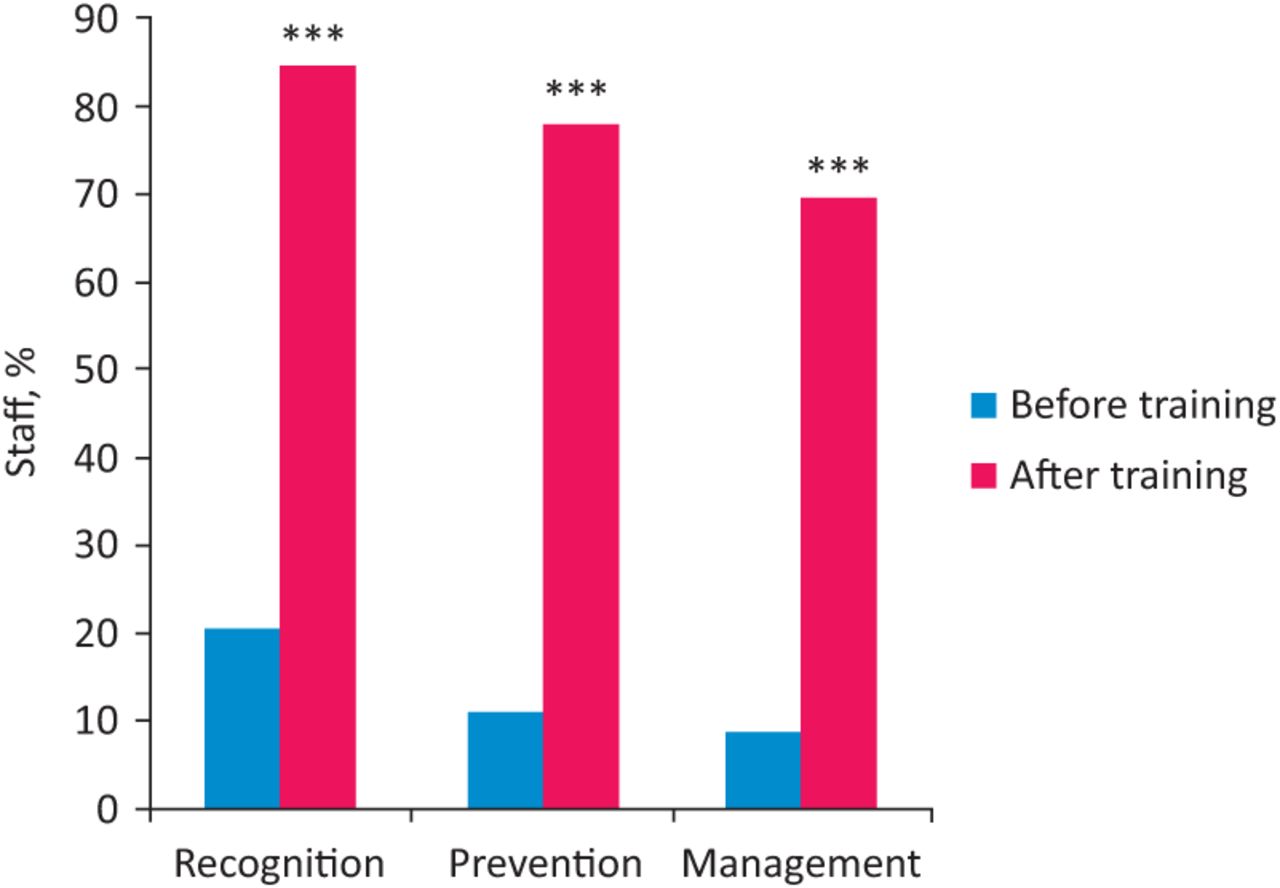
250 staff were trained, of which 124 and 90 completed pre- and post-education evaluation questionnaires respectively. Marked improvements in staff confidence were seen in recognition (64%), prevention (67%) and management (60%) of delirium which were all highly significant (p<0.01) (Fig 1), and an overall improvement in knowledge of factors which have been shown to precipitate delirium such as critical illness, dehydration, pre-existing dementia, catheterisation, restraint and visual impairment 16 was demonstrated. There were also marked improvements in confidence levels in recognition (55%, p = 0.0005) and management (48.4%, p = 0.0039) of dysphagia with more modest improvement in knowledge of signs of dysphagia in dementia (Table 2).

Percentage of care home staff confident or very confident in the recognition, prevention and management of delirium before and after training.***p = 0.0001.
Percentage of care home staff confident or very confident in the recognition, prevention and management of delirium, and the recognition and management of dysphagia.
Carers’ satisfaction
Questionnaires were sent to 80 carers who participated in advance care planning and who agreed to complete a satisfaction questionnaire; 64 (80%) were returned. Among this group, there were high levels of carer satisfaction; 92% carers rated the service >9/10. Few carers gave written reasons for ratings, but the comments of those who did were encouraging. One carer stated:
My mum had made a living will and it was something she always talked about with her family, this process has given me the confidence to know my mum’s ‘voice’ will be heard even though she can no longer communicate effectively. As a family we also feel we have been given the opportunity to be ‘heard’ for the first time.
Place of death
By April 2013, 102 care plans had been completed. 4/102 stated a preference to die in hospital. 67/68 residents who died during follow up, did so in their preferred place.
Admissions to hospital
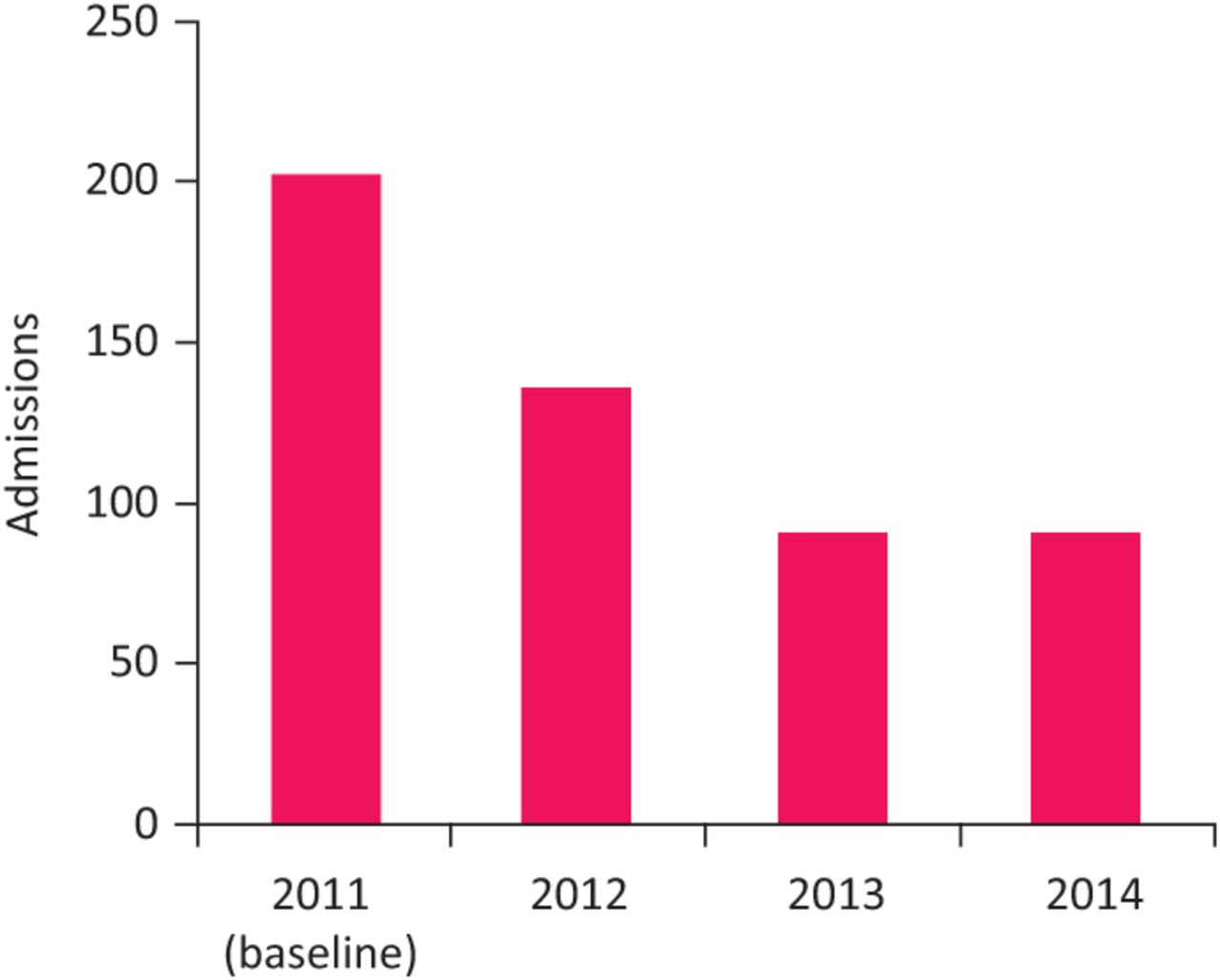
A fall of 66 admissions from the baseline of 202 was seen in the first year (2012) and exceeded in the second (2013) and third (2014) with a fall of 111 from baseline, which represents a 55% fall in admissions (Fig 2).

Admissions to hospital from pilot care homes before (2011) and after introduction of the service (2012, 2013 and 2014).
Cost impact
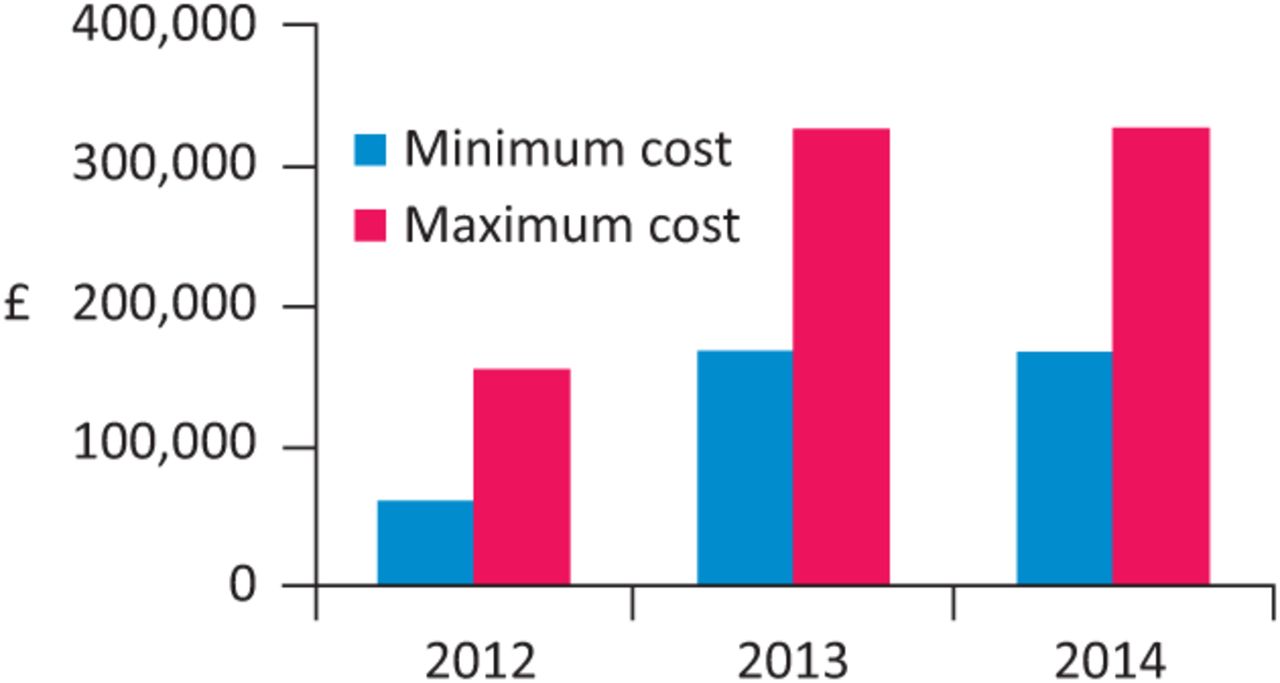
Using National End of Life Intelligence Network figures, cost of admissions minus cost of the service was estimated (Fig 3).
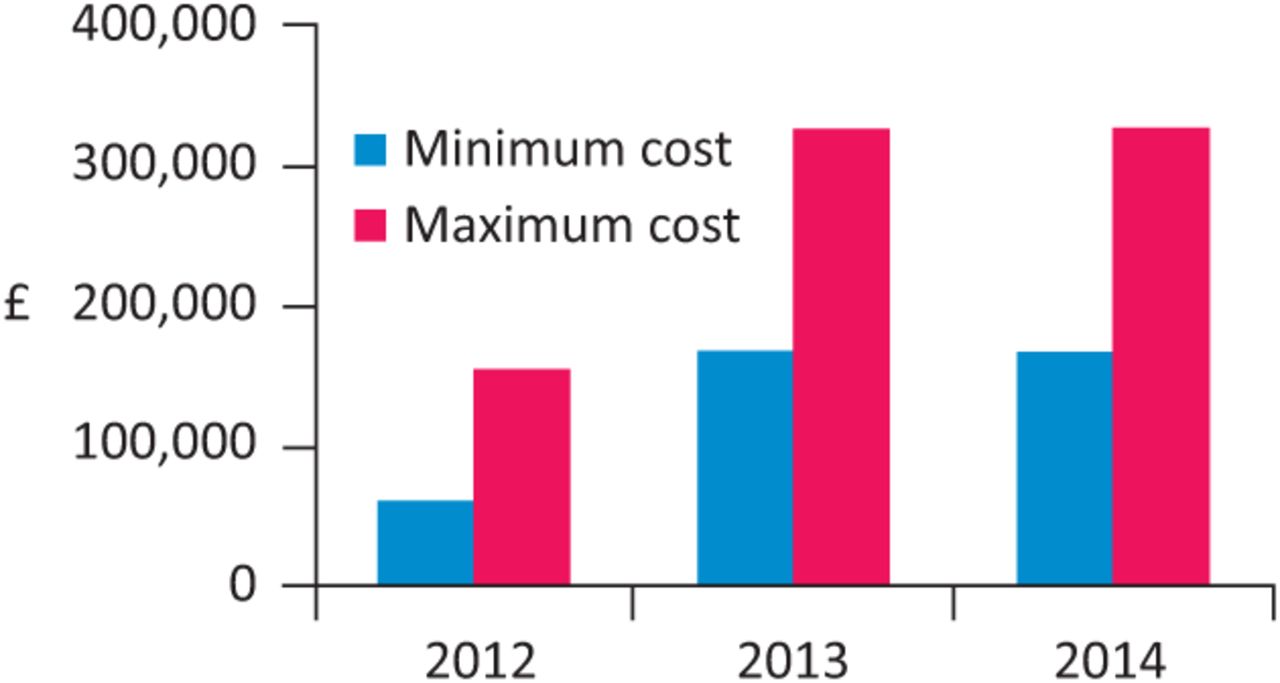
Cumulative net savings using minimum and maximum NEOLIN admission costs minus cost of service.
Discussion
We describe implementation of an initiative to provide advance care planning and an educational programme to care homes to support the recognition and management of dementia complications that might drive hospital admission, with particular focus on delirium and dysphagia. We have also provided evidence of service impact: care home staff felt more confident in providing these aspects of care, carers reported high level of satisfaction with advanced care planning, the majority of residents going through the end-of-life scheme died in their preferred place, and a reduction in hospital admissions was observed after introduction of the service.
This study has limitations because evaluation was not undertaken experimentally and was ‘in house’ rather than external; however it demonstrates that previously studied measures can be put into practice and intended effects seen. ‘In-house’ evaluation may lead to a positive bias. Evaluation of the implementation was done post hoc, so there is risk of recall bias or failure to record important information. Furthermore, by assessing staff confidence but not their actions, whether improved confidence translated into changes in practice or whether improvement in confidence is sustained is unknown.
Changes in admissions may be vulnerable to time-trend bias. There is growing momentum in the UK to deliver care closer to home, and the possibility that the admission results are confounded by other parallel service initiatives needs to be considered. While we could have examined trends in other nursing homes in Lincolnshire, differing medical service provision, geography and ownership may have significantly confounded this and we have no information on interventions at these other locations. For example, in Sheffield, introduction of a locally enhanced service, whereby care homes are covered by a single general practice providing regular visits, has resulted in reduction of hospital admissions,17 demonstrating that other service models can enhance health service support to care homes to reduce hospital admissions.
This service was implemented in an urban setting where proximity between care homes and acute hospital may favour high admission rates. The reduction observed here might not occur in areas with care homes with lower hospital admission rates, such as rural areas. Locally, implementation of the service, based on evidence from elsewhere in the world, was deemed a success and the local clinical commissioning group now funds the service across a wider area and includes residents with frailty.
In terms of impact, the results are compatible with Canadian and Australian studies; they build on work in the UK done by the Gold Standards Framework but demonstrate that additional benefits may well be realisable in the UK setting.
The proportion of people dying in their preferred setting is high compared to previous surveys,18 an encouraging outcome. Assuming the reduction in hospital admissions observed in this project was due to the BCHS, we cannot be sure whether it was advance care planning, staff education or the combination that was responsible. Our understanding is that it is the combination of both aspects, since the intervention staff were responsible for making the advance care decisions but were not responsible for delivering the care in the care homes when terminal events transpired, which depended on the care home staff themselves. We initially restricted our project to people with dementia, but see no reason why the approach should not be helpful to frail care home residents without this diagnosis – the Canadian and Australian studies were not limited to people with dementia. It should be noted though, that in UK settings, up to 80% of care home residents have cognitive impairment.
The costing work is not an economic study. However, there are much wider economic implications for health and social care services. The cost of additional community services, which may be required to enable residents to remain in care homes, was not considered, nor does it take into account the effect on acute providers. While there may be lost income due to emergency admissions, additional bed capacity is likely to improve provision of elective procedures.
Why was implementation successful?
The benefits of initial funding, leadership and implementation of a service which affirms knowledge and helps to manage uncertainty in the care of care home residents with dementia are important factors. A local respected clinician was able to implement the service with charitable funding and support from local stakeholders at a time when there was little recognition of the needs of this patient population among public sector organisations. The importance of this work is that it demonstrates that it is possible to use existing evidence to implement a service, which, although modest both in cost and design, had a significant impact on the choices of care available to care home residents with dementia nearing the end of life. We believe the success of this model of care should be attributed to its empowerment of care home staff, families and doctors by affirming knowledge and using care planning to manage the uncertain end-of-life trajectories of people with dementia. The Bromhead Medical Charity has awarded a further grant to allow development of a more extensive care home service in Lincoln, which will build on what has been learned from this service.
Funding
This service was implemented with a two-year grant from the Bromhead Medical Charity and subsequent commissioning by the local commissioners of health care.
Acknowledgements
This work could not have been carried out without funding from the Bromhead Medical Charity and the dedication of one of the authors, Susan Pieniak, who has sadly died.
Footnotes
↵†deceased 20 June 2014
- © 2016 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}