
ABSTRACT
A 58-year-old man was referred for review due to the finding of splinter haemorrhages and digital infarcts. Further questioning revealed a history of unintentional weight loss and calf pain. There were no other clinical features of endocarditis, and no clear cause for the splinter haemorrhages on initial investigations. The discovery of widespread thromboembolic disease prompted a search for malignancy and an eventual diagnosis of oesophageal adenocarcinoma. Splinter haemorrhages resolved with anticoagulation and directed treatment of the underlying malignancy. This case report reminds clinicians of the potentially broad differential diagnosis associated with this clinical sign.
Case history
A 58-year-old male of Malaysian background was referred to the emergency department for investigation of three months of bilateral fingernail splinter haemorrhages, digital infarcts and a two-week history of bilateral calf pain. Directed questioning also revealed a productive cough and unintentional 5-kg weight loss. He had recently returned from Malaysia two weeks prior to admission and was otherwise well. There were no other clinical features of infection or gastrointestinal symptoms. The patient denied intravenous drug use, and there was no personal or family history of thrombophilia or connective tissue disorder.
Past medical history was significant only for hypercholestero-laemia and a remote history of malaria. Regular medications included low-dose aspirin and atorvastatin. He was an ex-smoker with a 10 pack-year smoking history.
Investigations
On examination, the patient looked clinically well and was afebrile. Multiple splinter haemorrhages were evident in the third and fourth fingers bilaterally (Fig 1), with dusky discolouration in the right second and third toes, and a single digital infarct in the fourth left toe. Pulses were palpable and equal bilaterally. There were no other peripheral stigmata of infective endocarditis. Heart sounds were dual with a soft apical pan systolic murmur audible. Abdominal examination was unremarkable, with no hepatosplenomegaly. Calves were bulky, symmetrical and minimally tender to palpation. Urinalysis was unremarkable.

Splinter haemorrhages on third and fourth fingers of right hand (also found on left hand).
Investigations revealed a normochromic normocytic anaemia, normal white cell count and a C-reactive protein of 32 mg/L (reference value <5). Anti-nuclear antibodies were detected with a nucleolar pattern at a titre of 1 in 2560. Extractable nuclear antigen and dsDNA antibodies and anti-neutrophil cytoplasmic antibodies were not detected and screens for underlying causes of vasculitis, thrombophilia and haemolysis were all negative. Blood and urine cultures were persistently negative. Electrocardiography and chest X-ray were both normal.
An initial transthoracic echocardiogram demonstrated thickened mitral leaflets and a small, mobile, echodense lesion on the atrial surface of the anterior mitral leaflet. A subsequent transoesophageal echocardiogram did not detect any vegetations or septal defect. Arterial Doppler studies were normal; however lower limb venous duplex studies revealed bilateral extensive venous thrombi in the deep veins. Computerised tomography chest, abdomen and pelvis revealed segmental and sub-segmental pulmonary emboli, portal vein thrombosis and extensive intra-abdominal lymphadenopathy. In view of the extensive thrombosis, positron emission tomography imaging was arranged to detect any underlying malignancy. This revealed markedly increased glucose metabolism in the distal oesophagus and proximal stomach with uptake in regional lymph nodes. Endoscopic ultrasound allowed direct visualisation of a 3-cm ulcerated exophytic mass across the gastro–oesophageal junction and into the lower oesophagus, extending beyond the serosa with celiac axis lymph node involvement (Fig 2). Tissue biopsy and lymph node fine needle aspiration biopsy were consistent with adenocarcinoma.
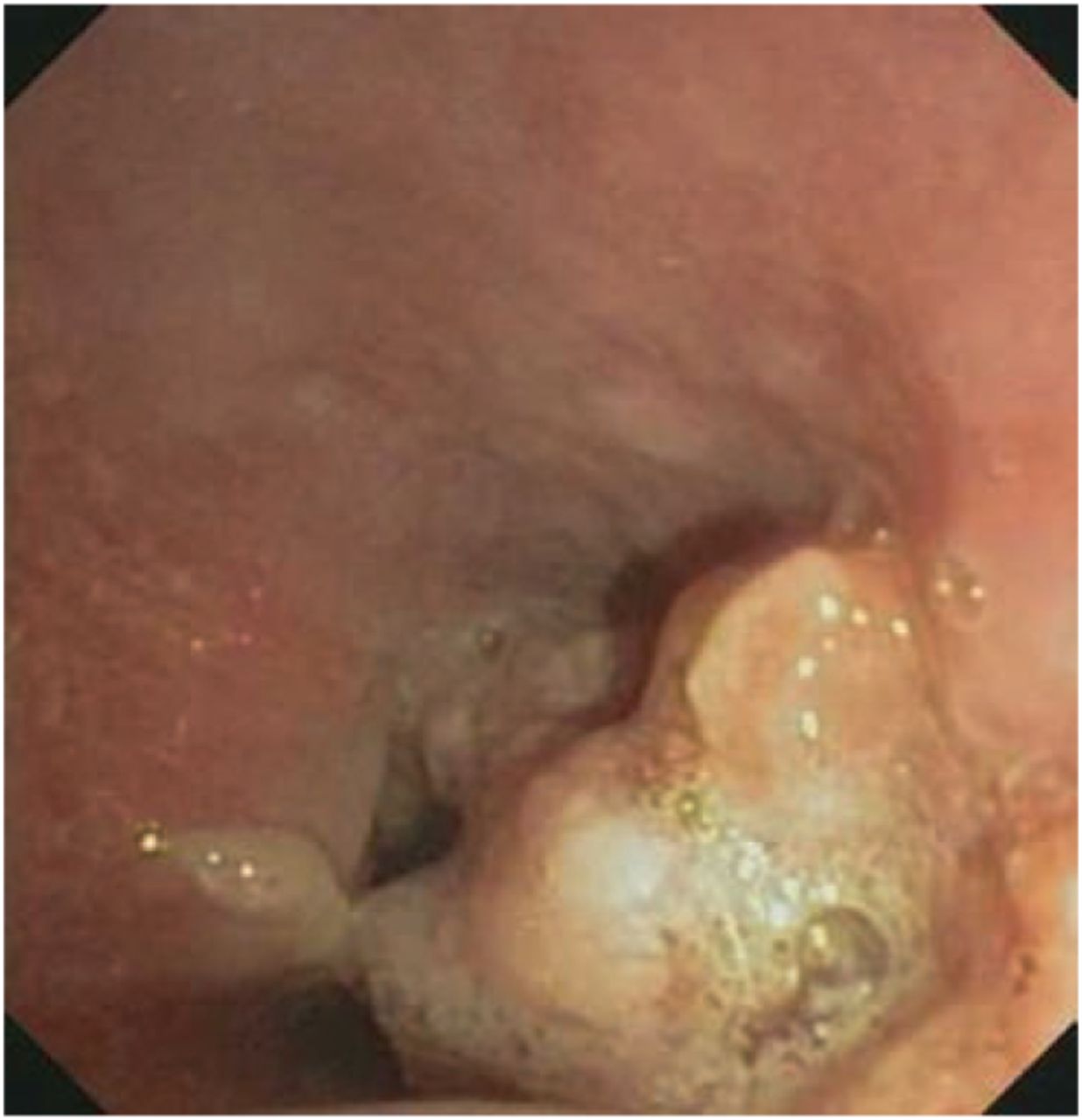
Hemi-circumferential mass at the lower third of the oesophagus.
The patient was commenced on therapeutic anticoagulation with enoxaparin and low-dose aspirin. An oncology opinion was sought regarding locally advanced oesophageal adenocarcinoma with nodal disease. Surgical resection was not advised and the patient commenced combination chemotherapy with epirubicin, cyclophosphamide and capecitabine. The patient received six cycles of combination chemotherapy, intravenous paclitaxel, local radiotherapy and maintenance therapy with irinotecan.
Notably, splinter haemorrhages and digital infarcts gradually and fully resolved following treatment (Fig 3).

Resolution of splinter haemorrhages with anticoagulation and chemoradiotherapy.
Discussion
Splinter haemorrhages have been recognised as a diagnostic sign of subacute bacterial endocarditis since the association was first described in 1920.1 Evolving literature has revealed an association with manual trauma,2 connective tissue diseases including systemic lupus erythematosus and rheumatoid arthritis,3 and the coagulopathy of antiphospholipid syndrome.4 Case reports have also described splinter haemorrhages occurring in the context of tick bite,5 histoplasmosis6 and certain drugs.7 The pathogenesis of splinter haemorrhages has been variably attributed to increased capillary fragility or embolic phenomena.2 Although the broad differential includes malignancy as a possible cause,8 there are very few case reports describing the clinical association in detail.
The above case report highlights the occurrence of splinter haemorrhages in the context of thrombosis and embolism due to underlying malignancy. In this case, splinter haemorrhages were the presenting feature of malignancy and most definitive finding on clinical examination. Resolution following anticoagulation and chemoradiotherapy supports the hypothesis of splinter haemorrhages manifesting due to thrombosis and hypercoaguability associated with underlying malignancy. Although this patient had experienced unintentional weight loss, it was the development of splinter haemorrhages that prompted referral for review. This report of malignancy presenting with splinter haemorrhages encourages clinicians to broaden the differential diagnosis when investigating this seemingly superficial clinical sign.
- © 2016 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.