
Abstract
Heart failure (HF) and atrial fibrillation (AF) are among the commonest cardiovascular conditions encountered in clinical practice and frequently coexist. Over the last decade, they have evolved into global cardiovascular epidemics. This, in turn, has huge clinical and economic implications. There is ample evidence that AF and HF have a mutually deleterious effect on each other. AF is not only a marker of HF severity but also affects HF prognosis independently. This article presents the close pathophysiological relationship between AF and HF and the adverse prognostic consequences of this bidirectional interaction. The scope of various therapeutic modalities and their potential impacts are discussed briefly.
Key points
Heart failure (HF) and atrial fibrillation (AF) have been recognised as global cardiovascular epidemics.
They frequently co-exist, are interdependent and have a mutually adverse prognostic impact.
Rate control remains the mainstay of therapy with rhythm control reserved for a specific group of patients.
Stroke prevention is one of the most important aspects of AF care in the HF population.
Introduction
Heart failure (HF) and atrial fibrillation (AF) are among the commonest cardiovascular conditions encountered in clinical practice and frequently coexist. Up to 40% of patients with HF either have, or go on to develop, AF and approximately 40% of patients with AF present with (or develop) HF.1 Heart failure predicts the development of AF and conversely the presence of AF predicts the development of HF. Both are increasingly prevalent phenotypic manifestations of a multitude of different primary or secondary cardiac pathologies (Fig 1).
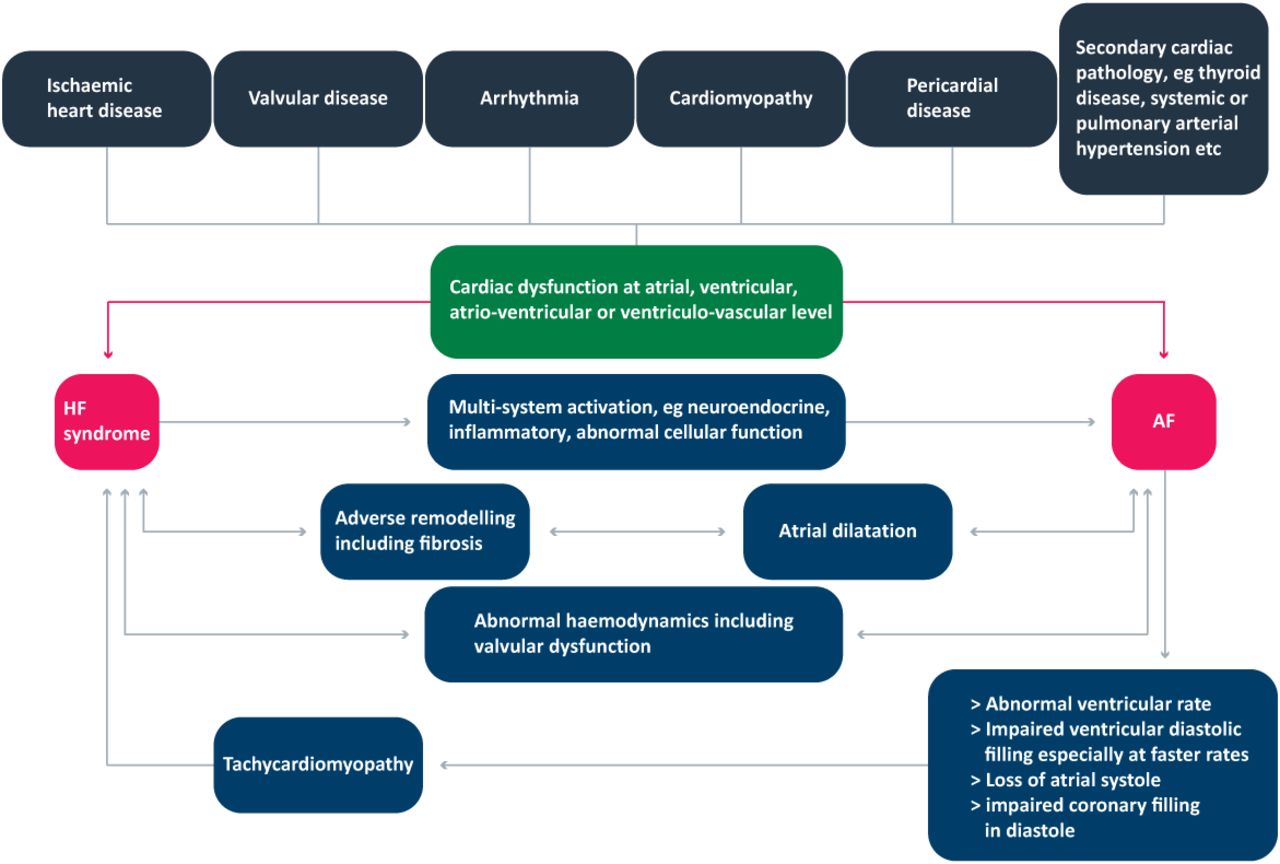
Interrelation between HF and AF demonstrating the causality of each and the mechanisms for one worsening the other. AF = atrial fibrillation; HR = heart failure. Adapted from Anter E, Jessup M, Callans DJ. Atrial fibrillation and heart failure: treatment considerations for a dual epidemic. Circulation 2009;119:2516–25.
The prevalence of HF and AF has steadily increased over the years. This is in part through an ageing population and development of more effective therapy that improves outcomes associated with other cardiovascular conditions (such as myocardial infarction). In Europe, HF has an estimated prevalence of 30 million with 1 in 5 lifetime odds of developing HF.2 Similarly, 2% of Europeans have AF, with a projected prevalence of 14–17 million by the year 2030.3 The lifetime risk of AF is 1 in 4 (as derived from community-based cohorts in Framingham and Rotterdam studies).
Interactions between HF and AF
Prognosis
The presence of AF is associated with an increased risk of mortality in patients with HF.4 This adverse prognosis is observed in patients with left ventricular (LV) systolic dysfunction (HF with reduced ejection fraction (HFREF)) as well as those with preserved left ventricular function (ie HF with preserved LV systolic function (HFPEF)). For instance, the SOLVD (Studies Of Left Ventricular Dysfunction) trial demonstrated that even in asymptomatic patients with an LV ejection fraction of <35%, mortality was 34% when AF was present and 24% when it was not. The mortality in new-onset AF (12%) was also greater than for persistent AF (7%).5 Sub-group analysis of the CHARM (Candesartan in Heart Failure Assessment of Reduction in Mortality and morbidity) study revealed that AF has an independent and deleterious effect on long-term all-cause cardiovascular mortality in HF patients. The absolute mortality risk was highest in patients with LVEF <35%; however, those with HFPEF had the highest relative risk of death (hazard ratio (HR) 1.37, 95% confidence interval (CI) 1.06–1.79) in contrast to HFREF (HR 1.22, 95% CI 1.04–1.43).6 Similarly, meta-analysis by Mamas et al (using data derived from 16 studies and incorporating over 50,000 patients) showed that AF had a negative impact on total HF mortality with an odds ratio of 1.40 (95% CI 1.32–1.48, P<0.0001) in randomised trials and 1.14 (95% CI 1.03–1.26, P<0.05) in observational studies. Again, this was applicable to HFREF as well as HFPEF patients.4
We have previously summarised scientific evidence showing the negative prognostic effect of AF in HF patients (Tables 1 and 2).7 However, it is not entirely clear whether AF per se is the cause of increased mortality or merely a marker of more advanced HF.
Prognostic impact of AF in HF: summary of randomised trials.
Prognostic impact of AF in HF: summary of observational studies
Symptoms of HF
AF is more likely to occur in patients with more severe HF symptoms (eg NYHA I, 10%; NYHA 4, 50%). Prolonged exposure to AF with a fast ventricular response also contributes to LV systolic dysfunction – a tachycardiomyopathy.
Stroke risk
AF confers a greater degree of stroke risk in HF patients as the presence of HF carries a weighting of 1 point in the CHADSVASC risk stratification tool for AF and stroke. The risk of stroke is equivalent both in HFREF and HFPEF alike at a rate of up to 4.4% per 100 patient years.8
Treatment of AF in patients with HF
Treatment algorithms for both are extensively discussed in guidelines elsewhere9 and are beyond the scope of this article. However, the main principles of the treatment of AF in patients with HF can be summarised as follows.
Rate or rhythm control
The commonest form of rate control is with AV nodal blocking agents such as beta blockers, rate-controlling calcium channel antagonists (provided LV systolic function is preserved) and digoxin.9 Management of both occurring together is extrapolated from trials in AF that contain between 20 and 30% of patients with HF and HF trials that contain between 10 and 30% of patients with AF.
However, the optimum target rate to achieve in AF is difficult to determine with any degree of precision. Current guidelines define adequate rate control in atrial fibrillation as maintenance of the ventricular rate response between 60 and 80 bpm at rest and between 90 and 115 bpm during moderate exercise.
Special considerations for AF ventricular rate control in HF include:
The optimum heart rate suggested in the AF-CHF trial (in which rate versus rhythm strategies were compared in HFREF patients) was 80 bpm at rest and less than 110 bpm with exertion. This trial also demonstrated no significant benefit in rhythm compared with rate control.11
Beta blockers are the most commonly indicated.9 It is unclear whether the beneficial prognostic effects of beta blockers in sinus rhythm in patients with HFREF are generalisable to similar patients with AF,10 but currently beta blockers remain the preferred rate-control agent in HFREF.
Digoxin is suggested in patients unable to tolerate beta blockers. This may include patients with acute decompensated HF in whom the negative inotropic effect of beta blockers may exacerbate congestion.
The role of cardiac glycosides in HF and AF has lately become controversial because of reports suggesting increased mortality in HF and AF patients on digoxin therapy.11 This evidence was based on observational studies and post hoc analysis and should therefore be viewed with these limitations in mind. So far, DIG trial is the only randomised controlled trial (RCT) in patients with HF and sinus rhythm but it did not present a direct comparison between digoxin and other rate-control agents. On the other hand, there is no RCT studying patients in AF with digoxin. Moreover, there is the confounding bias that physicians are likely to prescribe digoxin in patients who are more unwell and may have a higher overall mortality anyway. Nevertheless, it would be prudent to say that till we have more robust data available, digoxin should be used with caution in HF patients, keeping serum levels less than 1.2 ng/mL.12
By contrast, rhythm-control strategies (using anti-arrhythmic medications) have shown no benefit over rate control in terms of mortality, stroke prevention or hospitalisation. However, they can be reserved for patients who are intolerant to rate-control medications or remain symptomatic despite adequate rate control. A number of trials have looked at rate versus rhythm control. The Atrial Fibrillation in Congestive Heart Failure (AF-CHF) trial prospectively randomised 1,376 HFREF patients to amiodarone or rate-control medication. The cohort was followed up for three years looking at all-cause mortality, stroke and HF admission. The difference in mortality in the two arms was not significant (27% and 25%, respectively). In addition, there was increased morbidity from torsades and bradycardia in the rhythm-control arm.13 Similarly, the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM)14 and Rate Control versus Electrical Cardioversion for Persistent Atrial Fibrillation (RACE)15 trials have demonstrated similar findings. The latter, however, were not exclusive to HF patients and arguably, were underrepresented by a younger patient cohort who may be more symptomatic as well as in an earlier phase of the disease and, thus, are likely to gain more from rhythm-control compared with a rate-control strategy. It follows, therefore, that rhythm control should be reserved for patients who are particularly symptomatic with AF despite adequate rate control.
Since medications used for rhythm control (eg class 1a, class 1c agents, dronedarone) all have an increased mortality in HFREF, any rhythm-control technique that obviates the need for antiarrhythmic agents offers a clear advantage. Pulmonary vein isolation by using various catheter ablation techniques has emerged as an encouraging option in this regard. Its role in HF has shown early promise, but remains to be defined16 particularly in terms of long-term prognosis. To date, a number of small trials have shown very promising results17,18 (as risks of the procedure were not increased – when comparing patients with impaired versus normal LV function – and LV systolic function improved during long-term follow-up) while larger randomised trials are underway.19,20 Depending upon the results, AF ablation may potentially become an important first-line option in patients with HF. Finally, surgical ablation techniques (such as Cox maze procedure) are available to patients undergoing cardiac surgery. They have been shown to be safe and effective, including in patients with HF.
Pacing strategies can also be employed in patients with both AF with a fast and slow ventricular response (bradycardia pacing with subsequent rate-control medications) and in patients with refractory AF with fast ventricular response (pacemaker implantation with subsequent AV node ablation). This ‘pace-and-ablate’ strategy, however, does not eliminate AF per se. Studies conducted so far are small, non-randomised and mostly from single centres. Results are promising but further larger trials are warranted.
Lastly, development of newer antiarrhythmic drugs such as selective atrial-specific ion-channel blockers (eg vernakalant) may offer an advantage over previously available ones but their role in HF population needs further studies.
Thromboprophylaxis
Patients with AF and HF have their risk of stroke and systemic embolism doubled compared with either condition alone.21 Hence, thromboprophylaxis with oral anticoagulants is of paramount importance and has been shown to be safe and effective.22 Warfarin is thrice as effective as aspirin and novel oral anticoagulants (NOACs) are at least as good as warfarin. NOACs include inhibitors of either thrombin (dabigatran) or activated factor X (apixaban, edoxaban and rivaroxaban). Results from major trials (RELY, ARISTOTLE, ENGAGE AF-TIMI48, ROCKET) have been encouraging.23 Dabigatran was the first NOAC introduced into clinical practice. Comparison with warfarin in the RELY trial shows that its dose of 110 mg twice daily is superior for bleeding but non-inferior for thromboembolic protection, whereas 150 mg twice daily is non-inferior for bleeding but superior for thromboembolic protection. Apixaban, on the other hand, has been shown to be superior to warfarin in efficacy and associated with less gastrointestinal, intracranial and other major bleeding. Other factor X inhibitors are non-inferior to warfarin and associated with less intracranial and other major bleeding but higher gastrointestinal haemorrhage. Rivaroxaban and edoxaban have the added advantage of being once daily as well. Importantly, several NOAC reversal agents are currently in development and idarucizumab (which is a fully humanised monoclonal antibody fragment) has recently received global approval as a specific reversal agent for dabigatran.24
Finally, a small number of patients are unable to receive oral anticoagulation because of drug intolerance or bleeding contraindications. Left atrial appendage occlusion devices (such as Watchman device) hold promise in such cases but need further experience and long-term data.25
Conclusions
The prevalence of both AF and HF are increasing and they frequently coexist. Concurrence of AF and HF is associated with a higher risk of morbidity and mortality than either condition alone. There is no clear-cut evidence so far that rhythm control is superior (in terms of long-term mortality) to rate control. Radiofrequency catheter intervention techniques are promising and it is hoped that larger trials (looking at outcome data) would help incorporate these into the standard management algorithm. Finally, novel oral anticoagulants are a welcome addition to the therapeutic armamentarium available to the clinician. Future insights into mechanisms of disease and development of new therapeutic modalities continues to hold promise in this challenging field.
- © 2016 Royal College of Physicians
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.