
ABSTRACT
Parkinson’s disease (PD) was first described by James Parkinson in 1817. He noted the complex nature of this condition and that non-motor symptoms (NMS) underpinned the classic motor symptoms of PD. The concept of what PD is has therefore undergone substantial changes and it is now recognised that PD is a combined motor and non-motor syndrome and NMS are present during the prodromal phase of PD, starting up to 20 years before the first clinical motor signs emerge. PD may originate from pathology in the gut, olfactory bulb and lower brainstem rather than in the substantia nigra. Complex phenotypes of PD may exist where clinical NMS overshadow motor features. Therapy needs to be adjusted based on motor and non-motor loads, ideally using validated tools. Recently, a multimodal biomarker battery in PD has emerged and might play an important role in the future.
Key points
Parkinson’s disease is both a non-motor and motor disorder.
Motor symptoms present the visible syndrome of Parkinson’s disease, while non-motor symptoms span the journey of Parkinson’s disease from the prodromal to the palliative phase.
Late onset hyposmia and rapid eye movement sleep behaviour disorder appear to be robust markers for prodromal Parkinson’s disease.
The pathophysiology of Parkinson’s disease is now recognised to be the consequence of multiple neurotransmitter deficiencies leading to a multisystem degeneration.
Non-motor symptom subtypes of Parkinson’s disease have been recognised and future research will focus on subtype-specific treatment.
Introduction
Parkinson’s disease (PD) was first described by James Parkinson in his essay on the shaking palsy (1817).1 Already at this point, he described the condition as having a complex nature where non-motor symptoms (NMS) underpinned the classic motor symptoms of PD.1 However, for a long time PD has been considered as a motor condition with patients mainly suffering from stiffness (rigidity), slowness (bradykinesia) and shaking (tremor). During the last decade there has been increasing evidence published in the literature that PD is indeed a very complex multisystem disorder that is a combined motor and non-motor syndrome. Each patient with PD presents very differently with an individual response to medication, specific complications and a variable prognosis. However, we are not yet able to determine how these presentations differ exactly and how, based on these, one can predict the treatment response and prognosis.
In this article, we address some of the different and novel concepts that have been described in the context of PD.
Non-motor symptoms in the prodromal phase of Parkinson’s disease
In clinical practice, patients present when the motor symptoms, such as tremor, bradykinesia and rigidity, are present. The cornerstone for the management and treatment of PD has been a focus on control of motor symptoms. However, it has been shown that the ‘timeline’ for PD includes a variable period of 5–20 years, dominated by a range of NMS before the onset of motor symptoms.2 This is now regarded as the prodromal phase of PD and, recently, the International Parkinson and Movement Disorders Society (IPMDS) has devised specific research criteria for the diagnosis of prodromal PD.3 This will become relevant if we have effective neuroprotective therapies in PD, of which currently there are none.4 Therefore, in future, it may be possible to identify patients presenting with isolated or combined prodromal non-motor markers of PD who are at high risk of developing motor Parkinson’s.5 Table 1 summarises NMS that have been described in the literature as predating the onset of motor symptoms.6–22 Of these, rapid eye movement (REM) sleep behaviour disorder (RBD) and late onset hyposmia appear to be robust markers for future development of the motor aspects of parkinsonism and PD.23
Documented associations and suggested links between non-motor symptoms (associated with prodromal Parkinson’ disease) and the onset of motor Parkinson's disease.
Development of new diagnostic criteria
Currently, PD is still mainly diagnosed by applying the Parkinson’s UK Brain Bank criteria, which focus purely on motor symptoms; a wide range of different NMS that are now recognised to occur in the prodromal PD stage or in early PD are not included and are even regarded as exclusion factors in some cases. However, because of the growing evidence of a range of NMS in prodromal PD, the IPMDS convened a committee to revise the core motor criteria for PD. They have now published clinical diagnostic criteria for PD, which combine the central motor symptoms and additional new evidence, including NMS, to increase the likelihood that the central motor symptoms are indeed specific to PD.24 These criteria are meant to be applied in research studies and might also be useful to support the clinical diagnosis of PD even for health professionals who are inexperienced in PD.
Role of genes in the pathophysiology of Parkinson’s disease
The most common genes that have been described in relation to PD are LRRK2, Glucocerebrocidase (GBA), Parkin, PINK1 and DJ-1. Some of these genetic mutations have now been associated with specific non-motor features and as such the prodromal PD period may also be linked to genetic markers.
LRKK2 gene mutations with the Gly2019Ser type have been shown to lower the risk of cognitive impairment in PD,25 while LRKK2 PD tends to have a risk of greater motor progression,26 as well as being prone to experiencing more sleep onset insomnia.27Parkin mutation patients have an earlier and more symmetrical onset with a slower progression of the disease, unlike LRKK2.25,28PINK1 and DJ-1 mutations may have progressive motor deficits as well as gait dysfunction, as outlined in rat models.29GBA mutation, as usually seen in Gaucher’s disease, is now recognised to be a major risk factor for the development of sporadic PD and is associated with cognitive decline as well as dementia.30
Genetic causes cannot currently be determined with sufficient evidence.31 As such, genetic testing is not routinely done in clinical practice and is not recommended. However, in patients with an early onset (<40 years of age), genetic testing in research settings may play an important role in further understanding the pathogenesis and progression of PD. In particular, as mentioned earlier, LRRK2 and GBA mutations may express specific NMS such as sleep disturbances or cognitive problems. In future, one might be able to predict the PD phenotype based on the affected gene and the management could be adjusted.
Role of the vagus nerve
Several groups have now reported that the entire gastrointestinal tract (GIT) might be affected in PD, often well before the motor symptoms occur, which is in line with the evidence of prodromal NMS. Shannon et al analysed biopsies from the colonic mucosa of untreated patients with PD and showed that all were positive for alpha-synuclein. They also reported on three cases with biopsies positive for alpha-synuclein and who, on follow-up, developed PD.32,33 As a consequence, it has been speculated that the GIT possibly acts as an entry for environmental factors that then further lead to PD, although others have disputed this finding.34 Another theory suggests that PD starts from the brainstem as originally suggested by seminal work from Braak and colleagues.35 Ulusoy et al were able to reproduce PD-like alpha-synuclein spreading, starting in the lower brainstem and moving towards more rostral regions in a rat brain.36 Furthermore, Holmquist et al showed that by injecting a toxic lysate of alpha-synuclein into the GIT, the vagus nerve is subsequently affected and the toxin actively spreads via the vagus nerve to the dorsal motor nucleus of the vagus nerve and further travels to the substania nigra.37 It is, therefore, not surprising to speculate that PD might, at least in part, be caused by an ingested pathogen working its way through the GIT, through the vagus nerve into the medulla.38
Motor and non-motor phenotypes
Commonly, we divide PD into different motor subtypes, such as tremor dominant subtype, akinetic rigid subtype and mixed subtype. However, Marras and Lang have recently reviewed the described motor subtypes and identified various problems. 39 Von Coelln and colleagues have also shown that motor subtypes appear to be unstable and change over time.40 In summary, these results underpin the fact that one cannot predict the progression of PD with great certainty based on motor subtypes.
Recently, it has become increasingly evident that within the wide range of different NMS occurring in patients with PD, specific NMS dominant subtypes might present. These subtypes seem to be more prominent at a prodromal and early stage of the condition, whereas some subtypes merge in advanced stages of PD with an increased rate of comorbidities. It appears the non-motor subtypes are very closely linked to our current understanding of the pathology of PD and, as such, non-motor subtypes might be more robust and stable compared with motor subtypes.
In future, one might be able to predict the response of PD patients to treatment and improve the treatment strategy based on the subtype that patients are presenting.
There are several studies that have described the existence of different non-motor phenotypes within PD. These reports are based on clinical experiences and include reviews,41 case reports, observational studies, retrospective and prospective studies42 and, finally, cluster analysis.43
Our group suggested seven different subtypes within a real-life PD cohort: Park cognitive, Park apathy, Park depression/anxiety, Park sleep, Park pain, Park fatigue and Park autonomic (Table 2).44 The pathophysiological explanation for the existence of these different subtypes is the fact that PD can spread via three different routes: brainstem route, olfactory to limbic route and neocortical route. Sleep and autonomic dominant subtypes are most likely related to a brainstem route; anxiety, depression and other serotonergic symptoms dominant subtypes to a limbic phenotype; and cognition and apathy dominant subtypes to a cortical phenotype.
Proposed phenotypes within Parkinson’s disease. Amended from Sauerbier et al.44
Validated tools for grading non-motor symptoms
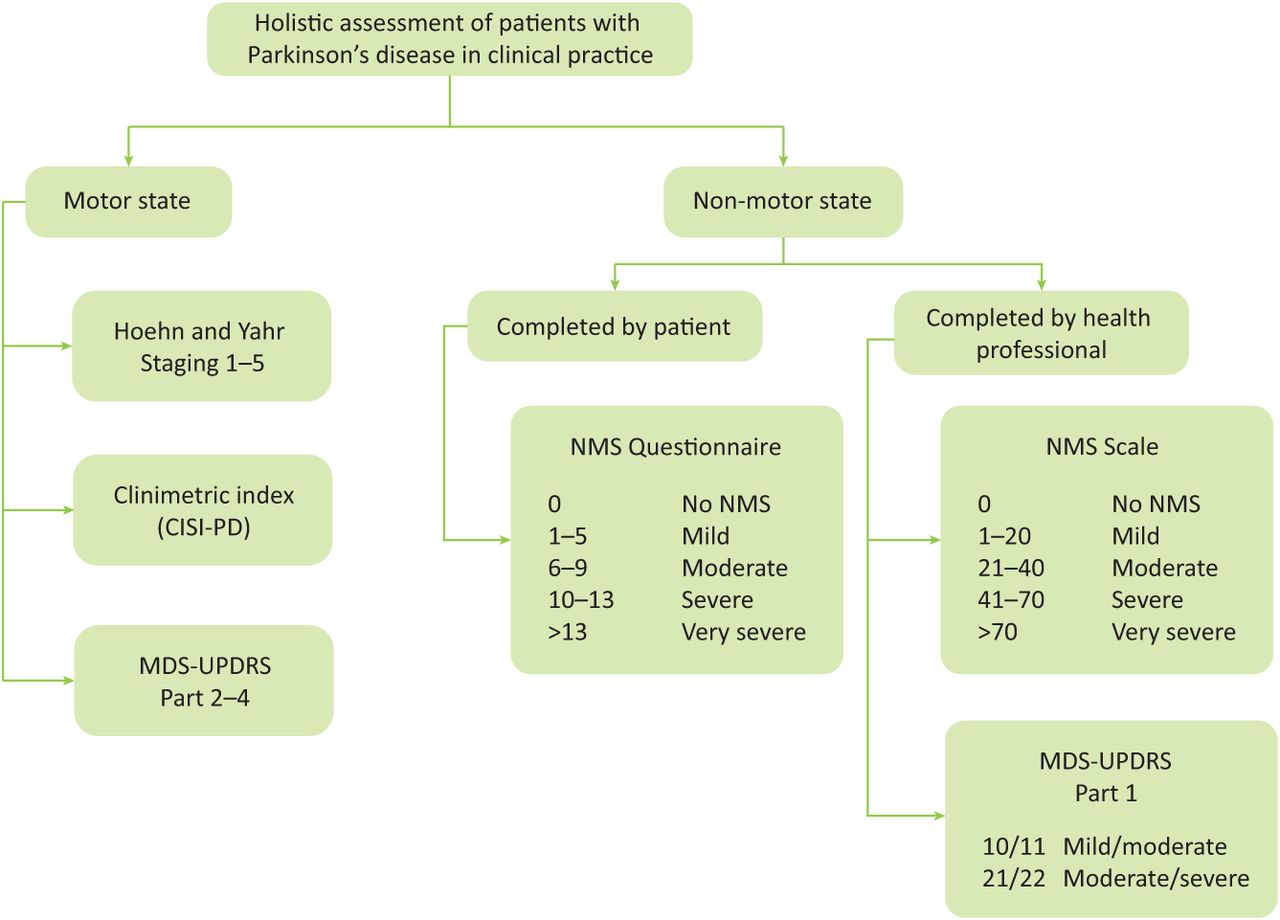
There are now several validated tools (completed by the patient as well as health professionals) available that empower patients to report their symptoms and allow clinicians to measure and grade the holistic burden. The available tools that address NMS include the NMS Questionnaire, the NMS Scale, as well as the IPMDS unified Parkinson's disease rating scale (UPDRS) part 1.45–47 In clinical practice, it is recommended to apply these tools together with a standard motor and clinimetric assessment, such as Hoehn and Yahr,48 UPDRS part 2–4 as well as clinical impression of severity index (Fig 1). As a consequence, the progression of the condition and the response to treatment can be measured in a structured manner, allowing for both NMS and motor symptoms to be addressed without the risk of remaining undeclared.
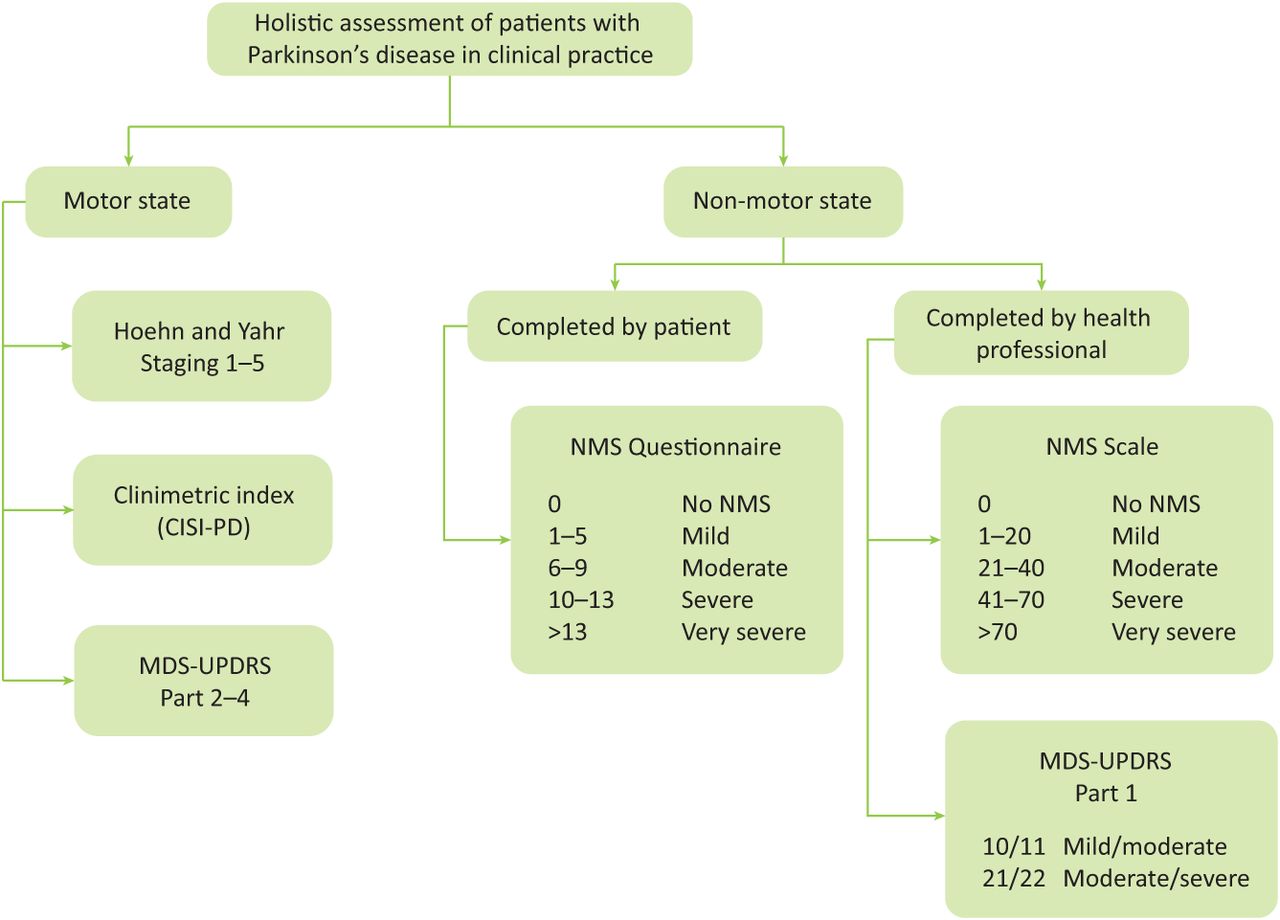
A proposed algorithm for holistic motor and non-motor assessment of patients with Parkinson’s disease in clinical practice. CISI-PD = clinical impression of severity index- Parkinson’s disease; MDS = movement disorders society; NMS = Non-motor symptoms; UPDRS = Unified Parkinson’s disease rating scale.
Imaging in Parkinson's disease
Given that PD is characterised by the dysfunction in cholinergic, serotonergic, noradrenergic and dopaminergic pathways, multimodal imaging techniques are being used to understand the pathophysiology of PD and to find ways to detect the early stages of PD (prodromal PD) and new methods of differentiating PD from atypical PD.
Metaiodobenzylguanidine (mIBG) myocardial scintigraphy was initially applied in heart disease in order to measure postganglionic presynaptic cardiac sympathetic sympathetic innervation. Consequently, reduced myocardial mIBG uptake has been illustrated to be useful not only in the diagnosis of PD but in differentiating PD from other neurodegenerative parkinsonisms such as multiple system atrophy (MSA) and supranucelar palsy (PSP).49 There are no set guidelines for the use of PD neuroimaging in clinical settings, even though it has been used in research for almost 30 years.50 It has been demonstrated that both single-photon emission computed tomography (SPECT) and positron emission tomography (PET) can differentiate between degenerative and non-degenerative parkinsonisms effectively. While structural or diffusion weighted and metabolic PET are capable of being able to distinguish between PD and atypical parkinsonisms, they require complex enhancement techniques.50
Early parasympathetic dysfunction has been described to occur in early stages of PD. C-donepezil PET is able to successfully image the systemic parasympathetic denervation, detecting a distinct decrease in acetylcholinesterase density in the small intestine and pancreas of patients with PD and might serve as a marker for early PD in the future.51
Biomarkers
A recent review assessing the accuracy of clinical diagnosis of PD concluded that the accuracy has not significantly improved during the last decade and biomarkers might be important in ascertaining correct clinical diagnosis and progression pattern in future.52–54 Several studies have tried to establish potential biomarkers for the diagnosis and progression of PD, including clinical (eg prodromal NMS), biochemical (eg saliva, biopsy, blood, CSF), genetic (eg GBA, PINK 1, SNCA, DJ-1, SNCA, LRKK2, Parkin) as well as imaging biomarkers (eg PET, SPECT, magnetic resonance imaging (MRI), transcranial sonography, functional MRI).50 Given that the pathological hallmark of PD is Lewy-bodies, which constitute aggregate alpha-synuclein, previous studies have focused on detecting alpha-synuclein in biological fluids such as cerebrospinal fluid, saliva or blood. However, the data from different studies are contradictory and show inconsistencies.52,53 Recently, Mollenhauer et al, as part of the DeNoPa study, investigated multiple biomarkers that might act as progression markers in PD.55 They were able to establish an assembly of ten explanatory biomarkers, including MDS UPDRS I, the Autonomic-Scale-for-Outcomes in PD, the Epworth Sleepiness Scale, the RBD Screening Questionnaire and RBD confirmed by polysomnography as well as voxel based morphometry units of cortical gray-matter and hippocampus, which exhibited substantial comparative worsening in PD patients when compared with healthy controls. Relative improvement was displayed in the severity of NMS by applying the NMS Scale and two depression scales (Beck Depression Inventory and Montgomery-Asberg Depression Scale).55 Interestingly, cognitive measures and select laboratory markers were not considerably changed in PD patients when compared to the healthy controls and further work in measuring cognition is required.55,56
It is unrealistic to expect that a single biomarker will fulfill all of the criteria of accurate diagnosis and disease progression. Indeed, using a combination of biomarkers is the most likely rational approach.
Conclusions
NMS are integral to motor PD. Motor subtypes have been extensively described in the literature and associations of motor PD with progression and genetics are being investigated. Several descriptions of different non-motor phenotypes within PD that appear to be closely linked to our current understanding of PD pathology have also been described. The latter may have an important role in refining future clinical trial populations as well as developing subtype specific treatments.5
- © 2016 Royal College of Physicians
References








{kind=link}
Jump to section
- Article
- ABSTRACT
- Key points
- Introduction
- Non-motor symptoms in the prodromal phase of Parkinson’s disease
- Development of new diagnostic criteria
- Role of genes in the pathophysiology of Parkinson’s disease
- Role of the vagus nerve
- Motor and non-motor phenotypes
- Validated tools for grading non-motor symptoms
- Imaging in Parkinson's disease
- Biomarkers
- Conclusions
- References
- Figures & Data
- Info & Metrics