
ABSTRACT
The National Institute for Health and Care Excellence (NICE) updated its guidelines for chronic heart failure (HF) in 2010. This re-audit assessed interim improvement as compared with an audit in 2011. Patients with HF (preserved and reduced ejection fraction) attending a tertiary cardiac centre over a 2-year period (January 2013–December 2014) were audited. The data collected included demographics, HF aetiology, medications, clinical parameters and cardiac rehabilitation. In total, 513 patients were audited. Compared with 2011, male preponderance (71%) and age (68±14 years, (Mean ± SD)) were similar. 73% of patients lived outside of London. HF aetiologies included ischaemic heart disease (37% versus 40% in 2011), dilated cardiomyopathy (26% versus 20%) primary valve disease (13% versus 12%). For patients with left ventricular systolic dysfunction (n=434, 85% of patients audited) 89% were taking beta-blockers (compared with 77% in 2011), 91% an angiotensin converting enzyme inhibitor or angiotensin receptor blocker (86% in 2011) and 56% a mineralocorticoid receptor antagonist (44% in 2011); 6% were prescribed ivabradine. All patients were reviewed at least 6-monthly. Although 100% of patients were educated about exercise, only 21 (4%) enrolled in a supervised exercise programme. This audit demonstrated high rates of documentation, follow-up and compliance with guideline-based medical therapies. A consistent finding was poor access to cardiac rehabilitation.
Introduction
Heart failure (HF) represents a major economic challenge to all developed countries and their allied health economies. It is a common condition with an increased prevalence with age.1 Patients are prone to repetitive prolonged, costly and potentially lethal hospitalisations. The economic burden for HF accounts for 2% of most westernised health economies; the same has previously been demonstrated within the NHS.2 HF accounts for 1 million inpatient bed days (2% of the NHS total) and 5% of current emergency admissions to hospital, with 70% of the incurred costs being allied to hospitalisation.3,4 Notably, the prevalence of HF is predicted to further increase over the next decade because of an increasingly aging population. The pool of potential patients has also been expanded by the successes of strategies for treating other heart conditions, including primary percutaneous coronary intervention for ST-elevation myocardial infarction.5
HF may be subcategorised on the basis of cardiac imaging into populations with HF and preserved ejection fraction (HF-PEF), and HF with reduced ejection fraction (HF-REF) or left ventricular systolic dysfunction (LVSD). In terms of treatment strategy, there is now an established clear treatment regimen for patients with LVSD based on large randomised double blind controlled trials that have demonstrated the prognostic and clinical benefits of neurohormonal antagonism6–8 and beta adrenoceptor antagonists.9 Additionally for selected patients, further treatment options include cardiac resynchronisation therapy, implantable cardioverter defibrillators, cardiac transplantation and left ventricular assist devices. The evidence base for treatment within populations with HF-PEF has largely been disappointing and current guidance mandates the treatment of allied comorbidities with further trials ongoing within the area.10
The national3 and international guidelines11 summarise or reflect on the evidence base, with the most current recommendations from the National Institute for Health and Care Excellence (NICE)3 for chronic HF being published in 2010. Key priorities highlighted for implementation were as follows:
Ensure close monitoring of key clinical indices in patients with HF – functional status, fluid balance, heart rhythm, medication reviews and key biochemical parameters (eg renal profile).
Increase prescription rates of established medical therapies in HF-REF/LVSD (beta-blockers, angiotensin converting enzyme inhibitors (ACEi)/angiotensin receptor blockers (ARB) and mineralocorticoid receptor antagonists (MRA).
Widen access to cardiac rehabilitation through group-based exercise programmes designed for patients with HF, which should include a component of psychological and educational support.
Here we delineate the completed audit cycle as compared to the current guidance within a tertiary hospital within an established professorial HF unit.
The heart failure team
The HF team at the Royal Brompton Hospital accepts national tertiary referrals for patients with HF of all aetiologies, serving a population spanning a large geographical area. With respect to outpatient management, the core team is composed of:
four specialist HF consultants (one professor and three consultants)
three full-time HF specialist nurses with hospital-based roles and a remit to liaise with a larger network of secondary care and community based-HF nurses
two deanery subspecialty training senior cardiology registrars, alongside a number of research and senior clinical fellows
dedicated cardiac pharmacists
deanery core medical trainees.
The HF team operates within the larger hospital network of consultant specialists in advanced cardiac imaging (echocardiography, cardiac magnetic resonance, nuclear, cardiac CT), cardiomyopathy, structural heart disease, interventional cardiology and cardiac surgery. A full palliative care team works alongside the HF team.
Outpatients with HF are served by seven consultant-led and four specialist nurse-led clinics with a weekly multidisciplinary team meeting for complex case discussion in parallel with further weekly forums for advanced device therapies and joint cardiology/cardiothoracic meetings for structural heart disease and revascularisation.
Methods
All HF patients attending Royal Brompton Hospital under the care of the HF team were included throughout two audit periods (2010–11 and 2013–14) following release of the NICE HF guidelines in 2010.3 Patients with reduced or preserved ejection fraction were included, irrespective of their underlying aetiology. Outpatient reviews were audited for compliance with key indicators relating to three priorities for implementation described in the NICE guidelines.3 The first priority was patient monitoring, including assessment of clinical (functional capacity, fluid status, heart rhythm etc) and biochemical (serum urea, creatinine, electrolytes and estimated glomerular filtration rate (eGFR)) parameters at least 6-monthly in stable patients; second was prescription of evidence-based medication in HF-REF patients at maximum tolerated doses, specifically a beta-blocker and ACEi/ARB licensed for HF alongside and MRA if indicated; third was rehabilitation provision, including the education of all patients regarding the benefits of exercise in chronic HF and referral to an evidence-based rehabilitation programme.
The second audit period assessed improvement following the implementation of agreed action. Where appropriate, statistical analysis was performed using the Chi-Squared test, SPSS X7 (IBM, New York, USA). As the work completed represented a departmental audit, local ethical approval was not required.
Agreed action implemented following first audit period
Firstly, after an initial pilot period using a hard copy pro-forma began during the first audit period, an electronic data capture system was introduced covering the key monitoring indices outlined in the NICE guidelines. This system was extended to all HF clinics within the institution for the second audit period, enabling the complete capture of demographic data, HF aetiology, prescribed medication, heart rhythm and rate, measures of clinical follow-up (functional capacity, fluid status, renal profile etc) and compliance with rehabilitation. Secondly, after particular challenges with the provision of HF-based rehabilitation programmes were highlighted during the first audit period, further questions were added to better understand the process and highlight potential alternative solutions. Finally, a widespread education programme on evidence-based therapies in HF was introduced – targeted particularly at junior multidisciplinary team members in order to create more opportunities for appropriate treatment instigation and up-titration – alongside concerted engagement initiatives with GPs and referring secondary care trusts and patient education to provide ongoing senior support.
Results
Clinical characteristics
In total, 292 and 500 patients were included in the 2011 and 2014 audit cycles, respectively. There was a similar age profile (67±14 in 2011, 68±14 2014, p=0.33) and male preponderance (70%, p=0.87) in both groups (Table 1). Compared with 2011, a greater proportion of the patients in the 2014 cohort were from outside of London (74% versus 65%, p<0.0001).
Demographics and clinical characteristics
The predominant HF aetiologies were ischaemic heart disease (36% (in 2011) versus 37% (in 2014), p=0.81), idiopathic dilated cardiomyopathy (19% versus 25%, p=0.08) and primary valve disease (11% versus 13%, p=0.49) (Table 1). In 2014, there was a significant increase in the proportion of patients with HF-PEF (8% versus 19%, p<0.0001). There were small numerical variances in the mean heart rate (71±23 in 2011 versus 68±12 in 2014, p=0.01) and left ventricular ejection fraction (38±5 in 2011 versus 40±13 in 2014, p=0.01) of undetermined clinical significance.
Monitoring
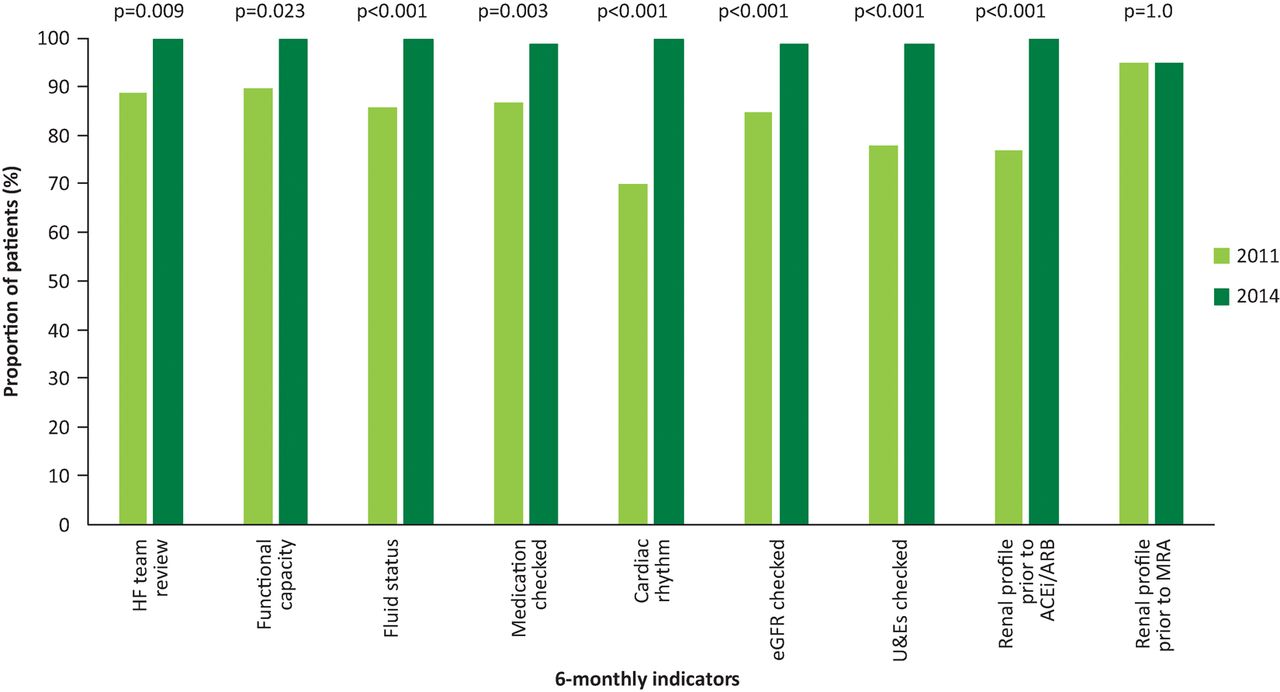
Key clinical (functional capacity (89%), fluid status (90%), medication review (87%), heart rhythm (70%) and biochemical (eGFR (85%), urea and electrolytes (78%)) indicators were monitored at least 6-monthly in a high proportion of patients during the initial audit cycle, and this subsequently increased significantly to near 100% completeness for all parameters upon re-audit in 2014 (Fig 1). Similarly, the proportion of patients with a documented renal profile prior to initiation of an ACEi/ARB also increased (75% in 2011 versus 100% in 2014, p<0.001; Fig 1). By contrast, only a static small proportion of those commenced on an MRA did not have documented renal function (5% in 2011, 5% in 2014, p=1.0; Fig 1).

Monitoring: NICE 6-monthly indicators. The proportion of patients receiving the relevant monitoring at least 6-monthly. ACEi = angiotensin-converting-enzyme-inhibitor; ARB = angiotensin receptor blocker; eGFR = estimated glomerular filtration rate; HF = heart failure; MRA = mineralocorticoid receptor antagonist; NICE = National Institute for Health and Care Excellence; U&E = urea and electrolytes.
Medication in left ventricular systolic dysfunction
In comparison to the 2011 cohort, in 2014 the proportion of HF-REF patients prescribed the maximum tolerated dose of a beta-blocker (89% versus 77% in 2011, p=0.004), ACEi/ARB (91% versus 86% in 2011, p=0.002) and MRA (56% versus 44% in 2011, p<0.001) all increased significantly (Fig 2). In the 2014 cohort, 29 (6%) patients were prescribed ivabradine.
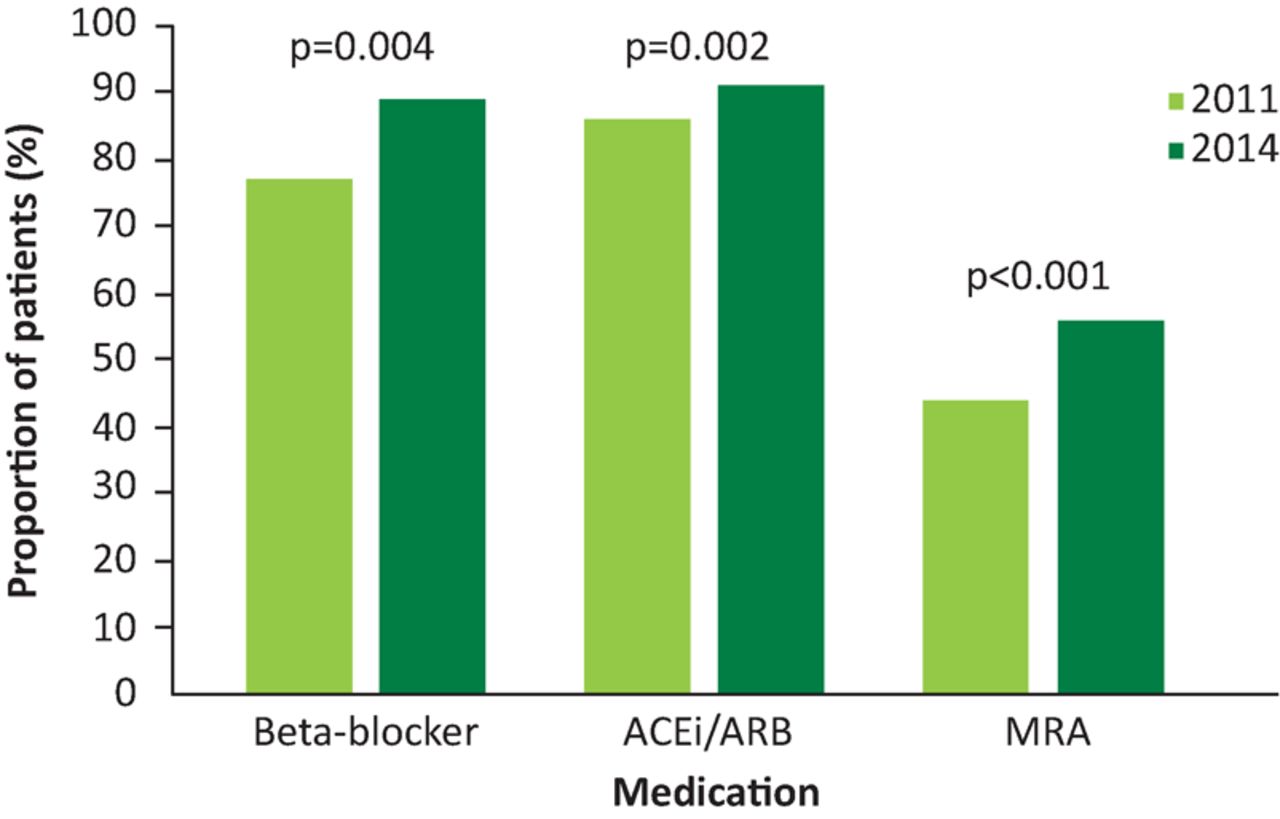
Left ventricular systolic dysfunction medication prescribing. The proportion of patients with left ventricular systolic dysfunction prescribed the relevant prognostic medical therapy. ACEi = angiotensin-converting-enzyme-inhibitor; ARB = angiotensin receptor blocker; MRA = mineralocorticoid receptor antagonist.
Rehabilitation
Over the course of the audit period, there was a significant increase in the number of patients being educated about the benefits of exercise in chronic HF (36% in 2011 to 100% in 2014, p<0.001, Fig 3). Despite this, access to rehabilitation remained low, with only a small proportion being either referred (6% in 2011 versus 3% in 2014, p=NS) or enrolled (1% in 2011 versus 4% in 2014, p=NS) on a supervised exercise programme with an evidence base in HF.
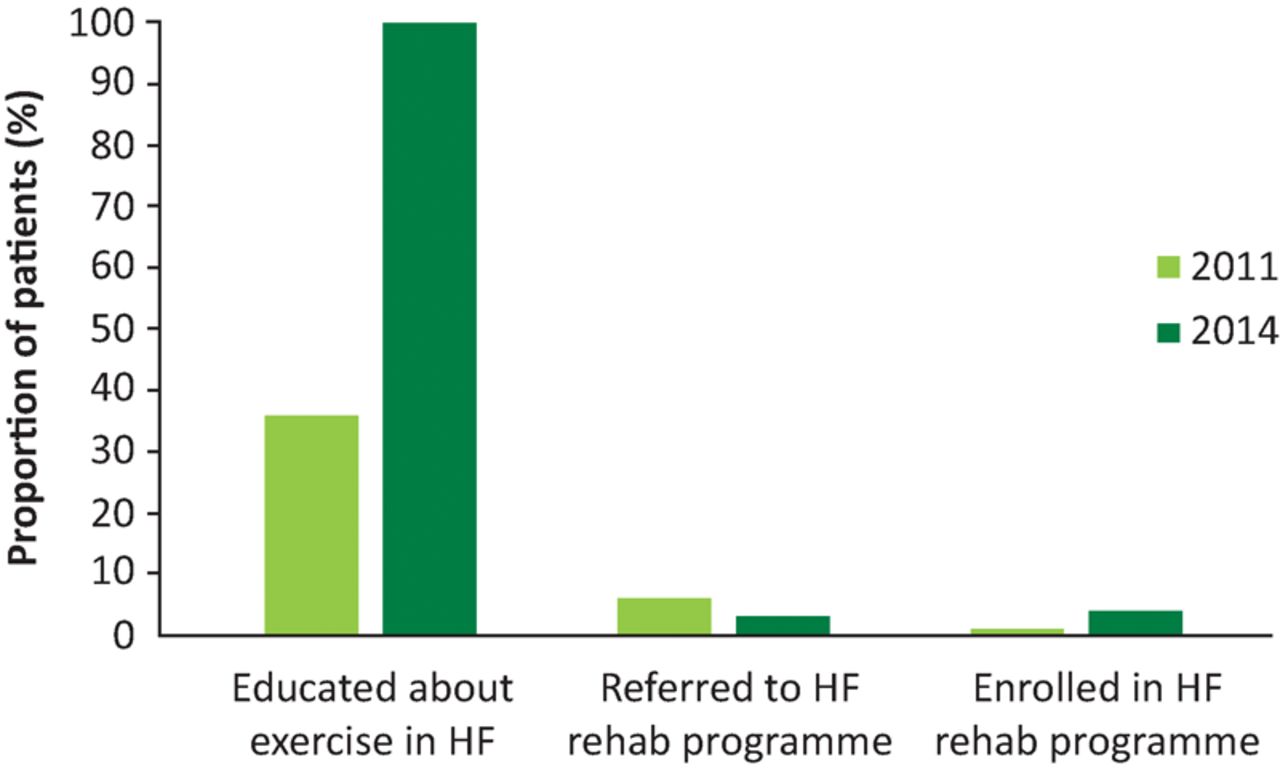
Access to cardiac rehabilitation. The proportion of patients with access to relevant cardiac rehabilitation. HF = heart failure.
Discussion
HF continues to pose serious challenges for healthcare systems and economies. The increasing prevalence of HF allied with prolonged and deadly hospitalisation ensures that it remains a significant and costly problem for global healthcare. Moreover, a significant proportion of hospitalisations that apparently occur as acute HF decompensation, transpire to be an acute-on-chronic decompensation.
The chronic care of patients with HF has been evaluated and summarised within national and international guidance.3,11 By rigorous and dedicated application/implementation, programmes following such guidance should reduce morbidity and mortality within HF populations (with particular attention to those patients with LVSD). Emphasis is placed on lifestyle advice, appropriate usage of pharmacological evidence-based therapies, the selective application of advanced HF therapies (including cardiac resynchronisation therapy, implantable cardioverter defibrillators and assist devices, transplantation), disease monitoring and exercise-based rehabilitation. All of these aspects of care should be embedded within a multidisciplinary programme.
This completed audit focused on three critical areas for implementation highlighted in the NICE 2010 guideline3 and, with an update currently under review, details progress made over the lifetime of this document within a professorial unit at a tertiary hospital in London. The rate of compliance with directives increased generally from 2011 to 2014. The first key priority concerned monitoring, reflecting that care of HF patients mandates diligent follow-up with focus on symptomatic status, physical examination, pulse rate, rhythm, blood pressure and basic haematological and biochemical indices. Our audit demonstrates a clear improvement in the monitoring of all of these components. The current recommendations suggest a monitoring interval of at least 6 months for those with stable chronic HF. Apart from the historical model of conventional healthcare within England and Wales, novel monitoring methods may be useful and may become the clinical norm in the future outpatient setting. This includes telemonitoring and implantable device-based remote monitoring. However, the currently available trial data reports conflicting conclusions, although further larger trials are expected to be reported in the future.12,13
For patients with LVSD, the rates of prescription for all recommended evidence-based pharmacotherapies significantly increased during the 4-year audit period (the second key priority) and now demonstrate high concordance with NICE standards. The prescription data from this audit is comparable to that obtained from large multicentre national and international registries.4,14,15 Ivabradine is a novel sino-atrial node inhibitor, which acts by selective inhibition of sodium channels within the sino-atrial node. This audit documents a rate of 6% usage within the LVSD population (29 patients). This reflects the updated technology appraisal guidance16 released in late 2012, which advocates ivabradine as a treatment option for controlling heart rate in certain HF populations.
The third priority for implementation concerned cardiac rehabilitation; an established part of the therapeutic intervention package in other areas of cardiology, including post myocardial infarction and revascularisation following coronary artery bypass grafting. However, within HF, cardiac rehabilitation has long been relatively neglected despite being recommended as an important part of the multidisciplinary treatment for patients. Rehabilitation-based programmes have previously been shown to improve both morbidity and mortality within such patients.17,18 They have also demonstrated clear benefits in improving rates of smoking cessation and reducing levels of anxiety and depression.19
Although the number of patients who had the benefits of regular cardiovascular exercise explained to them rose from 36% in 2011 to 100% in 2014, the numbers actually referred to and accepted for rehabilitation still remain low. This is corroborated by national and European data, which demonstrate a consistently low level of enrolment of HF patients in rehabilitation programmes.19–21 Potential explanations for the disappointing levels of patient participation include geographical variation, lack of commissioning and financial restrictions. Hence, the current findings are suggestive that there needs to be a renewed and reinvigorated focus on the expansion and provision of rehabilitation services for HF patients, which should be highlighted as a key area for investment. Rather than using a conventional health facility-based rehabilitation programme, one alternative proposed for this group of possibly elderly and comorbid patients is to consider a home-based option instead.22 However, again there is limited evidence for such models in HF, with further exploratory work ongoing.
Limitations
This large audit cohort captures detailed data on the contemporary guideline-based management of chronic HF, although requires interpretation within certain limitations. The retrospective observational data from a single tertiary referral centre is subject to inherent selection bias and the complex multimorbid case mix the centre attracts may not be entirely generalisable. Furthermore, while high levels of data entry in the clinic database were observed, the prospect of some incomplete data influencing the conclusions cannot be entirely excluded. Finally, the audit design did not include standards in relation to compliance with recommendations for advanced device therapies (cardiac resynchronisation therapy and implantable cardiac defibrillators) outlined in the 2006 and 2014 NICE technology appraisals.23,24 The data collection process is being redesigned as a priority to cover this area for future work.
Conclusion
The audit cycle demonstrated an improvement in medical therapeutic prescription and increased adherence to monitoring recommendations achieved through simple agreed action. However, with regards to the provision of cardiac rehabilitation programmes for patients with HF, the available infrastructure still seems to be lacking and suggests that this aspect of care should be reviewed.
Conflict of interest
The authors declare no conflicts of interest.
- © Royal College of Physicians 2016. All rights reserved.
References








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.