
ABSTRACT
Acute care common stem acute medicine (ACCS AM) training was designed to develop competent multi-skilled acute physicians to manage patients with multimorbidity from ‘door to discharge’ in an era of increasing acute hospital admissions. Recent surveys by the Royal College of Physicians have suggested that acute medical specialties are proving less attractive to trainees. However, data on the career pathways taken by trainees completing core acute medical training has been lacking. Using London as a region with a 100% fill rate for its ACCS AM training programme, this study showed only 14% of trainees go on to higher specialty training in acute internal medicine and a further 10% to pursue higher medical specialty training with dual accreditation with internal medicine. 16% of trainees switched from ACCS AM to emergency medicine or anaesthetics during core ACCS training, and intensive care medicine proved to be the most popular career choice for ACCS AM trainees (21%). The ACCS AM training programme therefore does not appear to be providing what it was set out to do and this paper discusses the potential causes and effects.
Introduction
The last decade has seen increasing numbers of acutely ill patients attending hospitals for medical management. Providing appropriate care is a challenge and strategies have concentrated on such patients having access to a ‘competent clinical decision maker at the front line of acute medical services’ and the creation of an appropriate training structure receptive to the acute medical workforce needs.1–4 Acute care common stem (ACCS) training was introduced in 2007 as a ‘core’ training option for trainees after completion of 2 years of foundation training. It aimed to attract trainees interested in the acute aspects of medicine with career aspirations in acute medicine (AM), emergency medicine and anaesthetics.5,6 Trainees enter the pathway on one of these three parent specialties; this parent specialty is then pursued for higher specialist training after completion of the three ‘core’ training years. These consist of rotations through all three specialties as well as intensive care medicine (ICM). Trainees completing ACCS AM training are also eligible to apply to any postgraduate medical specialty training programme.
ACCS AM was designed to develop competent multi-skilled acute physicians for subsequent higher specialty training in acute internal medicine (AIM), which became a recognised specialty in its own right in 2009.6,7 Data from the Royal College of Physicians (RCP) suggest that acute medical specialties, particularly AIM, are proving less attractive to trainees and surveys of trainees in acute medical specialties have demonstrated dissatisfaction, particularly with regard to workload.4,8–10 However, data on the career pathways taken by trainees who have completed core acute medical training is lacking. ACCS AM posts have a mean national ‘fill rate’ of 98.5% and recruitment data have shown the programme to have a 100% ‘fill rate’ in London where the competition ratio for posts has the highest value nationally.11,12 This study aims to establish the career paths chosen by ACCS AM trainees in London since inception of the training programme, focusing on whether or not this training programme is producing a cohort of practising acute medical physicians.
Methods
Data regarding the demographics and career pathway of all ACCS AM trainees who had undertaken training in London from the inception of the programme in 2007 until August 2015 were collected by Health Education England (HEE) London. Data that were not held by HEE London were traced via the Joint Royal College of Physicians Training Board (JRCPTB) e-portfolio system or the General Medical Council (GMC) register. Any trainees untraceable by these methods were contacted personally via email, requesting information on their medical career history. Data was analysed using Microsoft Excel 2013. Ethical approval was deemed unnecessary in view of the study reviewing information in the public domain.
Results
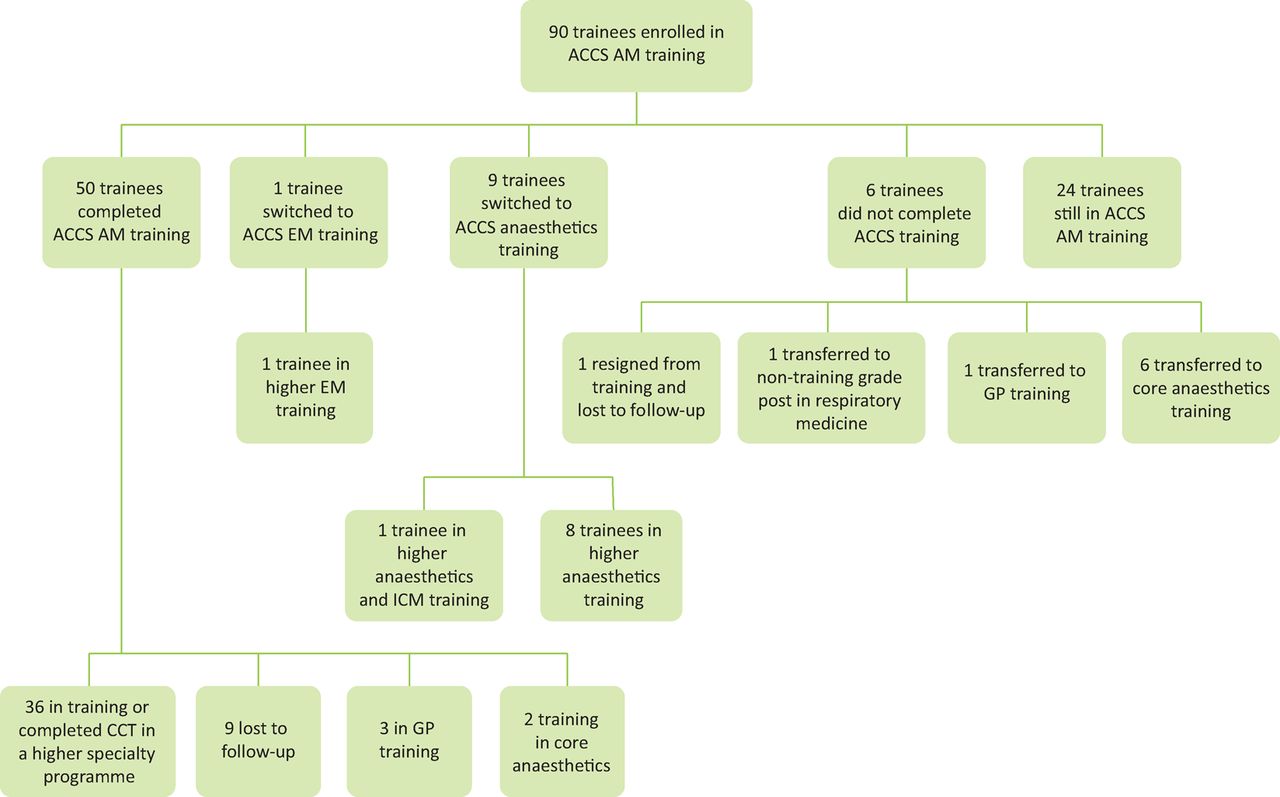
Since its inception in 2007, 90 trainees (55 female; 35 male) have enrolled in the ACCS AM training programme in London, with training numbers ranging between 11 and 13 per year. These are dependent on extraneous factors such as trainees needing to repeat sections of the training, train less than full time and rotational amendments as the programme changed from a 2 to 3-year duration. Ten trainees switched from ACCS AM training to an alternative parent specialty (1 to emergency medicine; 9 to anaesthetics) during their core ACCS AM training and subsequently completed ACCS training in their new parent specialty of choice. All of these trainees then went on to embark on higher specialist training in their new chosen specialty (Fig 1).
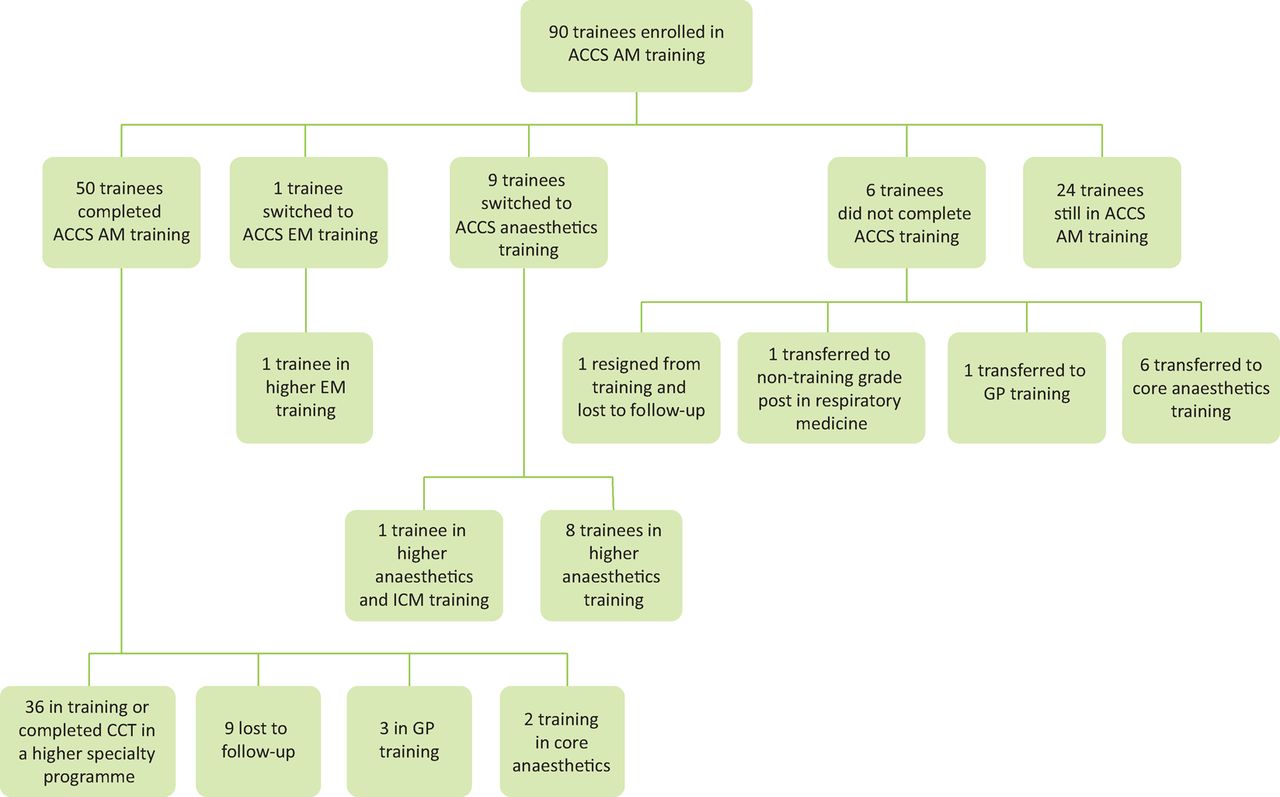
Training trajectories of ACCS AM trainees since inception of training programme. ACCS = acute care common stem; AM = acute medicine; CCT= certificate of completion of training.
In total, 50 trainees completed ACCS AM training, of whom 36 subsequently enrolled in a higher specialty training programme. Nine of these trainees progressed to higher specialty training programmes in AIM, AIM/general internal medicine (GIM) or AIM/GIM/ICM and seven trainees were appointed to other higher medical specialties (geriatrics, clinical pharmacology, infectious diseases, respiratory medicine) with dual accreditation with GIM (Fig 2). Ten trainees were appointed to single accreditation higher medical specialties and ten trainees were appointed to ICM programmes (either as single or dual specialty training). Three trainees went on to retrain in general practice (GP) and two trainees went on to retrain in ‘core’ anaesthetics. No career pathway data was available for nine other doctors post ACCS AM training but all were still registered with the GMC.

Higher specialty career pathways of the trainees who have enrolled in ACCS AM in London since 2007. ACCS = acute care common stem; AIM = acute internal medicine; AM = acute medicine; GIM = general internal medicine; ICM = intensive care medicine.
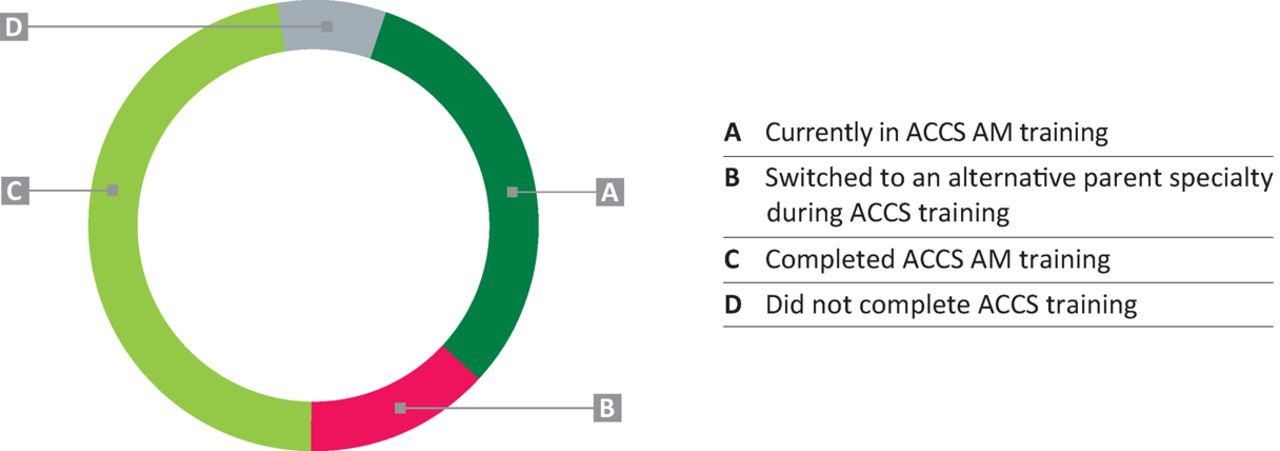
Six trainees did not complete ACCS training: one transferred to GP training, three left to retrain in ‘core’ anaesthetics, one transferred to a non-training grade post in respiratory medicine and one resigned after the first year of training and has been lost to follow-up. At the time of writing, 24 trainees remained in ACCS AM training programmes (Fig 3).
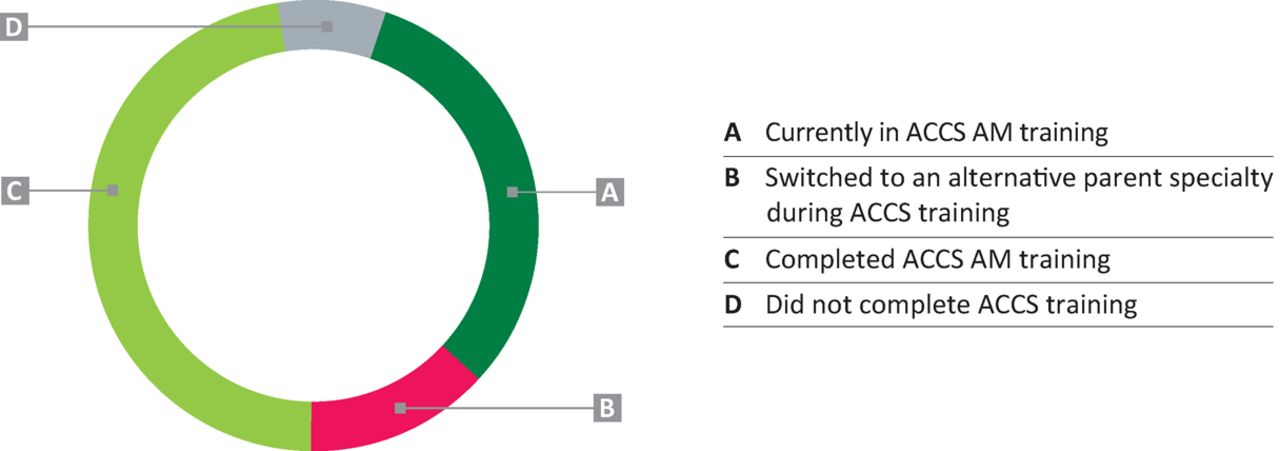
Outcome of those embarking on ACCS AM training in London since 2007. ACCS = acute care common stem; AM = acute medicine.
Discussion
The ACCS AM training programme aimed to create more doctors with a certificate of completion of training (CCT) in AIM or at least with skills and training in GIM alongside another specialty.6,7,13 However, this study, which reviewed the career paths of 90 doctors embarking on ACCS AIM training in London over an 8-year period, identified only nine doctors in AIM higher training and seven training in other higher medical specialties with dual accreditation with GIM. These 16 trainees are a small proportion of the 66 trainees (24%) who should have completed ACCS training by August 2015, far below that desired and required for the future ‘acute medical workforce’.1–4
ACCS AM training programmes have traditionally attracted doctors that are motivated, driven individuals (often with an extended portfolio) and the programmes have had high fill rates.7 Indeed, in London there has been a 100% fill rate of ACCS AM posts every year with high competition ratios (between 5.6 and 7.1 applicants per post). However, the majority of these trainees are not subsequently pursuing higher specialist training careers in acute medicine.12 Recruitment data have shown declining mean fill rates for AIM higher specialty training programmes across the UK (75% in 2014 compared with 56% in 2015); these are much lower than other medical specialties. Indeed, while single accreditation higher medical specialties, such as cardiology and gastroenterology, had 100% fill rates in London in 2015, the AIM fill rate was 75%. Furthermore, Scotland and Wales struggled to fill their AIM posts in 2015 with 0% and 14% fill rates, respectively.7,11 Competition ratios for acute medical training programmes over the last 2 years have fallen, with the national competition ratio for posts in AIM higher specialty training programmes falling from 2.4 to 1.8.11–13 So why has it become so difficult to recruit highly competent trainees who have completed ACCS AM core training to higher specialist training in AIM? It has been suggested that medical registrars are feeling demoralised and undervalued, particularly with regard to providing acute care.10 It is widely felt that the job of the medical registrar is both the busiest and one of the most stressful in the hospital. A survey of core medical trainees in the UK highlighted the lack of attractiveness of acute medicine as a career as a real concern. Their witnessed experience of medical registrars impacted negatively on their decision to apply to specialist training programmes in that field.14 There has also been a perceived increase in the hours worked by trainees and consultants in acute medicine without a commensurate pay increase.15 These issues have a significant impact on ‘work–life’ balance, which is particularly relevant to an increasingly female medical workforce (as in this cohort) that has shown an increased rate of ‘less than full-time’ working as their career progresses compared with their male counterparts.15 A study published in the Journal of the Royal Society of Medicine (2015) looked at the factors affecting junior doctors’ career choices in graduates between 1999 and 2012.16 It found domestic circumstances to be one of the biggest influences on specialty choice and that influence has increased in more recent years.Unless efforts are made to provide greater support to the role of the acute physician and make it more attractive, recruitment into AIM and other specialties that dual train in GIM may remain problematic.10,14
RCP and HEE data have demonstrated a significant expansion of consultant (26%) and registrar posts (16%) in AIM but it still remains one of the most difficult specialties to recruit.12,15 Indeed, a recent RCP census showed that almost 50% of AIM consultant appointments remained unfilled because of a lack of applicants or suitable candidates, and that only 69% of AIM physicians in post expressed job satisfaction.15 These data reinforce the challenges of retaining ACCS AM trainees in their specialty and encouraging them to train in AIM at specialist registrar and consultant level.
With only 65 trainees nationally, ACCS AM represents a minority specialty in terms of numbers but these trainees have complex educational needs.10 The organisation and administration for these trainees is challenging and it can be difficult to provide them with a cohesive programme. Furthermore, the small number of trainees can lead to them feeling isolated from their peers and lacking in support with regard to educational progression. These issues are borne out by ACCS AM trainees in London having the highest rate of insufficient evidence at annual reviews of competence progression (ARCPs) compared with other medical specialties.
It is interesting to note that this study demonstrated 17% of ACCS AM trainees switched to anaesthetic training programmes. The unique opportunity afforded to ACCS trainees is that they are able to experience training in specialties other than their own parent specialty. The programme provides a breadth of acute medical experience; however, it does allow trainees to identify with other specialties, which may be the reason they choose to ‘jump ship’. It is difficult to speculate whether this was always their intention after being unsuccessful at initial ACCS application or whether they were ‘won over’ by the specialty during the rotation in ACCS AM training. Equally, the trainees may never have intended to pursue AM further than their core training years. It merely provided them with the general medical grounding they deliberately sought before continuing along another path. The trainees that embarked on ACCS AM may also have intended to train in another core training scheme, such as anaesthetic or core medical training, but were unsuccessful in securing training in this. These data were not available to us in this study and career intentions of trainees embarking on ACCS and other core specialties would be an area for further research.
ACCS AM trainees often have a less diverse grounding in general medicine and less exposure to the ‘acute take’ than their core medical training (CMT) counterparts by the end of their core training.5 The relatively short time spent on a medicine rotation can make preparation for the MRCP exam more difficult. However, ACCS AM remains a popular choice, possibly because of the increased exposure to acute and emergency medicine. This can give trainees timely exposure to procedures that they may not otherwise get in CMT.5
The integration into close working teams in the emergency department, operating theatre and intensive care unit can provide invaluable technical and non-technical skills not gained as easily on a general ward. Working in these areas can give the trainee exposure to the medical management of diverse cases that they would not otherwise see on the ‘acute medical take’ and has been suggested to improve job satisfaction.5 With this in mind, it is interesting to note the high proportion of ACCS AM trainees (21%) who went on to pursue a career in ICM. Studies looking at career intentions of junior doctors have shown that particular hospital departments or teachers are more important in influencing the hospital specialty choices. In close-knit departments, such as the intensive treatment unit (ITU) or the operating theatre, trainees may develop closer relationships or mentorship roles with consultants and senior staff. This exposure to more apprenticeship-based training could be perceived as better education and training in these specialties than compared with ward-based AM training and the reason for their change in career choice after ACCS AM.16–18
The ‘shape of training’ review recommends the need for a flexible and adaptable workforce to cope with the changing demands of the population.3 As such, a CCT in AIM or GIM would contribute to providing such a workforce. While 63% of the ‘physicianly’ training workforce currently contribute to the ‘acute unselected take’, only 39% plan to continue ‘acute take’ responsibilities when appointed to a consultant post.15 So the question is, how we can retain these bright and motivated trainees to continue their careers as the acute medical consultants that we so desperately need? With an increasing focus on general medical training there is a move towards enhancing the GIM elements of many of the higher medical specialty curricula.2,3,19 It is likely that we will see more higher specialty registrars contributing to the ‘acute unselected take’ in the future or at least contributing more to the acute management of their specialty patients. Will this additional need for contribution to the ‘acute take’ be a deterrent for future registrars or will a fairer and more balanced workforce take the pressure off the AIM, GIM and other specialties that currently support this service? If the latter workforce planning strategy was employed, a further question is whether a broadening of acute medical responsibilities contradicts or supports the RCP definition of an acute physician (Box 1)?19
It is worth considering if training for 3 years in ACCS AM is necessary. If the ACCS AM posts are not producing doctors that apply for specialist registrar and subsequent AIM consultant posts, it could be argued that they are not being used effectively. CMT is a 2-year programme and plans are ongoing to allow trainees more exposure to acute and critical care.20 Therefore, if the ACCS AM training stem is discontinued and its posts absorbed into CMT, it would release more training opportunities in acute and critical care medicine for CMT trainees. Recent recommendations from the JRCPTB suggest that CMT trainees should all undertake at least a 2-week placement in the intensive care unit; this could be a way of providing such training.20,21
This study has closely reviewed eight consecutive cohorts of ACCS AM trainees in the most competitive area of the country since inception of the programme. As such, this may suggest that the most competitive and driven trainees applying for ACCS AM were followed, with complete career pathway data from almost 90% of trainees. It is also the first study to provide prospective career trajectories of trainees who enrolled in ACCS AM training over a number of consecutive years, thus providing quantitative evaluation of whether or not this training programme produces practising acute medical physicians. Limitations include the small sample size of 90 trainees and a single region of the country being studied. However, there are only 65 ACCS AM trainees nationally and London is a region with the highest level of applicant to post ratio at ACCS AM application and a consistent 100% fill rate.
Royal College of Physicians Acute Medicine Task Force definition of the acute physician.16
Conclusions
We have demonstrated that very few trainees in ACCS AM are going on to become acute physicians with only 9 out of 66 trainees (14%), who should have completed ACCS AM training in London by August 2015, pursuing a career in AIM. The training programme is therefore not providing what it was set out to do as the vast majority (76%) are not going on to train in a higher specialty programme that supports the ‘acute unselected take’. The most popular career pathway of trainees enrolling in ACCS AM is ICM, attracting 21% of trainees. A number of trainees also switched to emergency medicine or anaesthetics (16%) during ACCS training. We suggest that the short fall in acute medical practitioners may be due to the demoralisation that doctors considering training in the general ‘physicianly’ specialties are experiencing. As well as this, the perceived job plan and satisfaction for a consultant in AIM is not attractive.
Further work needs to be undertaken to understand why this cohort of trainees are leaving the path of acute medicine in favour of other specialties. If the ‘shape of training’ reforms are introduced, more physicians will be expected to contribute to the ‘acute unselected take’. Decisions will need to be taken regarding the ACCS AM stem being abandoned to release more training opportunities in ICM and AM to the wider core medical workforce or, in contrast, the attractiveness of structured acute medical training programmes should be improved considerably. Trusts are under constant siege from acute admissions, many with extremely complex needs, and, despite efforts to curtail this, it shows no sign of abating. Latest figures show total admissions to hospitals in England have increased by 10,400 per day since 2005 and 1,200 per day since 2014.22 Every effort should be made to train a workforce that is able to meet the needs of this population. The changing demographic demands the expansion of more general and acute physicians within the workforce so we must find a way to attract and retain them.
Conflicts of interests
The authors declare no conflicts of interests.
Author contributions
The authors JB, KLB and CB are involved in the commissioning of ACCS and AIM training posts in London as well as supervising these training doctors locally in their trusts. EG and JB wrote the first draft of the paper. All authors contributed to subsequent drafts and review of the final version.
- © Royal College of Physicians 2016. All rights reserved.








{kind=link}
{kind=link}
{kind=link}