
A 41-year-old man who had been working in a lead smelting plant for 18 years presented to the clinic with a history of pain, numbness and tingling of his extremities with memory loss and lethargy. There was no other significant past or family history. General examination revealed mild hypertension with systolic pressure of 150 mmHg. Neurological examination revealed diminished vibration and proprioception peripherally in his arms. Computed tomography (CT) showed multifocal curvilinear calcifications in the subcortical white matter of both cerebral and cerebellar hemispheres (Fig 1) with few punctate calcifications in bilateral basal ganglia. Biochemical evaluation revealed elevated serum lead level 98 μg/dL (normal range 0–30 μg/dL), elevated serum creatinine to 2.2 mg/dL (normal range 0.7–1.4 mg/dL) and elevated parathyroid hormone to 292 pg/mL (normal range 10–65 pg/mL). Serum calcium and phosphorus were normal. CT findings of intracranial calcifications were attributed to chronic kidney disease as a result of chronic lead exposure. The patient was advised to change his occupation and treated with chelation therapy by ethylenediaminetetraacetic acid. Serum lead levels showed significant reduction to 40 μg/dL following treatment.
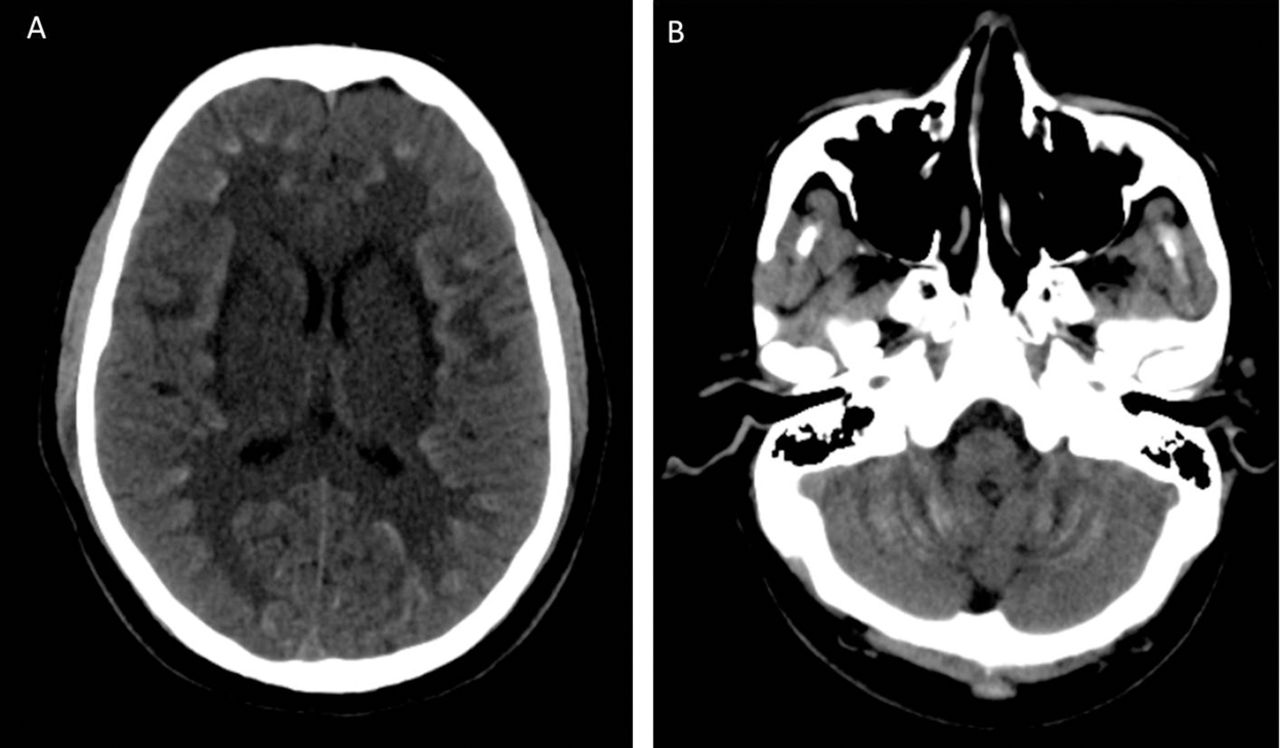
Intracranial calcifications. A – computed tomography (axial view) showed multifocal curvilinear calcifications in subcortical white matter of both cerebral hemispheres. B – computed tomography (axial view) showed multifocal curvilinear calcifications in subcortical white matter of both cerebellar hemispheres.
Conflicts of interest
The authors declare no conflicts of interest.
Acknowledgements
Written informed consent was obtained from the patient to publish the clinical details and images in this article.
- © Royal College of Physicians 2016. All rights reserved.








{kind=link}
Related Articles
Cited By...
- No citing articles found.