
ABSTRACT
Headaches are a common complaint in HIV positive patients attending emergency services. A thorough understanding of the differential diagnoses, initial investigations and empirical management of this presentation is essential for the assessing physician. We discuss a case of a patient with known advanced HIV infection presenting with headache to the emergency department. Given the range of possible diagnoses, broad-spectrum antimicrobial therapy was initially commenced. This was stopped when magnetic resonance imaging confirmed a diagnosis of venous sinus thrombosis. Anticoagulation therapy was started in accordance with current clinical guidelines after discussing the rationale and options for treatment with the patient. Here, we review the guidelines and supporting evidence for management of venous sinus thrombosis, and consider the challenges and strategies for engaging a patient with previous poor attendance in their ongoing care.
Case presentation
A 31-year-old man with known HIV presented with a 1-month history of global, constant headache. He reported a single episode of collapse with transient loss of consciousness that prompted presentation to the emergency department (ED). Past medical history included HIV with poor adherence to antiretroviral therapy (ARV) – latest blood CD4 count 140 cells/μL (range 500–1500 cells/μL), plasma HIV load 200 copies/mL. He reported no history of previous opportunistic infections. He was allergic to penicillin and took mirtazapine for depression. Originally from the Democratic Republic of Congo, he had not left the UK for the previous 10 years. There was no history of recreational drug use. Systems review was unremarkable.
On examination, the patient was alert and his Glasgow Coma Scale was 15/15. Observations were within normal parameters and he was afebrile. On examination he had mild pain on neck flexion but no true neck stiffness. There was no rash, photophobia or other abnormal findings. Peripheral nervous system and cranial nerve examinations were normal.
Initial blood tests are summarised in Table 1. Imaging comprised a chest radiograph and cranial computerised tomography (CT), which were both reported as normal. A lumbar puncture was performed, revealing a lymphocytic pleocytosis and an elevated opening pressure of 25 cm of water. Cerebrospinal fluid (CSF) samples were sent for microbiology (including rapid mycobacterial and fungal tests) and virology (Table 2).
Blood results
Cerebrospinal fluid results
Differential diagnosis
The differential diagnosis of prolonged headache in an HIV positive patient from a tropical region is broad; with a mild lymphocytic pleocytosis in the CSF, this includes tuberculosis (TB), viral meningoencephalitis, Listeria and cryptococcal meningitis. Space occupying lesions are another cause of headache in HIV. In developed countries, the most common causes are toxoplasmosis and primary CNS lymphoma.1 Infections, such as tuberculomas and aspergillomas, can also present as space-occupying lesions. In patients from developing countries, neurocystericosis should be considered in the differential. Other causes of a persistent headache range from imported infections like malaria, drug-induced headache, and, considering that HIV can be associated with a pro-coagulant state,2 venous sinus thrombosis.
Initial management
In a severely immunocompromised patient presenting with persistent, prolonged headache with a lymphocytic CSF, empirical treatment for likely infectious causes was commenced pending further results. Intravenous aciclovir and high-dose co-trimoxazole to cover Listeria were started in the ED (amoxicillin is first line for suspected Listeria meningitis, with co-trimoxazole used if, as here, there is a clear penicillin allergy). Given the sub-acute onset and history of emigration from a TB-endemic area, it was felt that empiric treatment for tuberculous meningitis using standard quadruple therapy was also indicated.
After 48 hours, the full results of the CSF sample were available (Table 2). CSF culture was negative, as was extended viral polymerase chain reaction (PCR); aciclovir and co-trimoxazole were therefore stopped. Mycobacterial smear and TB PCR were negative, but as these tests are relatively insensitive in the context of TB meningitis (sensitivities reported as 45–80%3), TB treatment was continued pending further imaging and results.
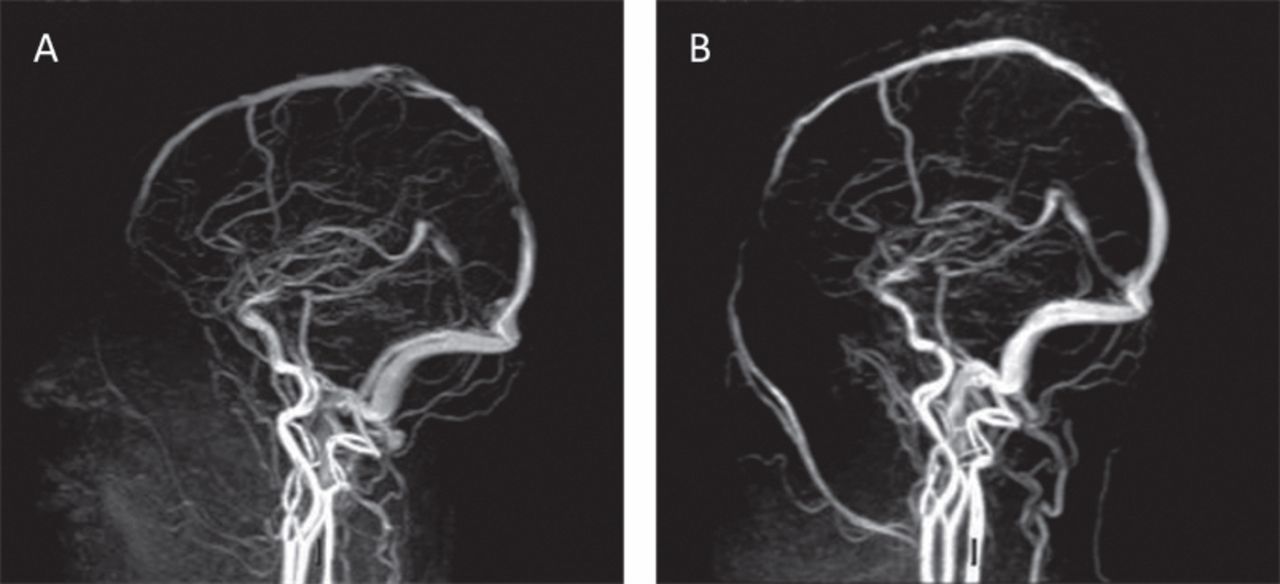
On the third day, MRI of the brain was performed to identify possible meningeal or parenchymal pathology. This demonstrated normal brain parenchyma and meninges. However, an increased superior sagittal sinus diameter, suspicious of a venous sinus thrombosis (Fig 1), was identified. A magnetic resonance venogram confirmed this diagnosis (Fig 2⇓).

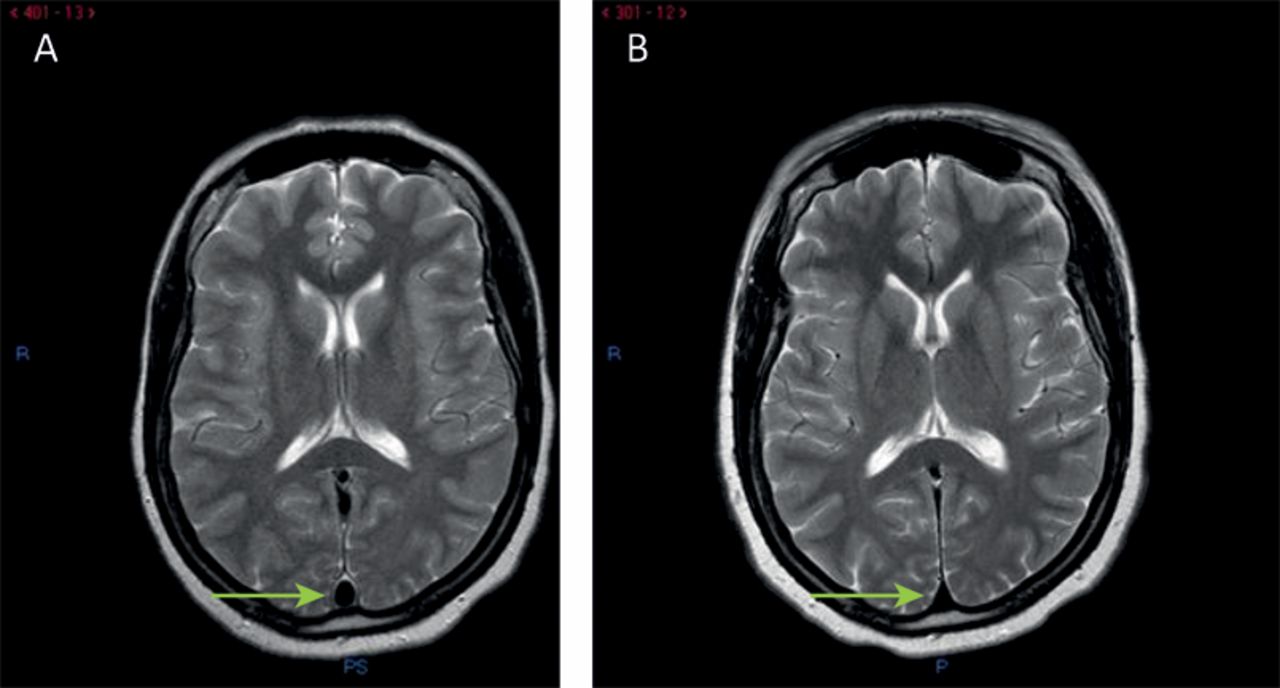
Magnetic resonance image (MRI) of brain. A – axial T2w MRI at time of diagnosis demonstrates ‘round’ appearance of superior sagittal sinus (arrow), suggestive of distal occulusion by thrombus. B – this appearance has resolved on follow-up MRI after successful treatment with anticoagulation, with return to the normal ‘triangular’ shape.
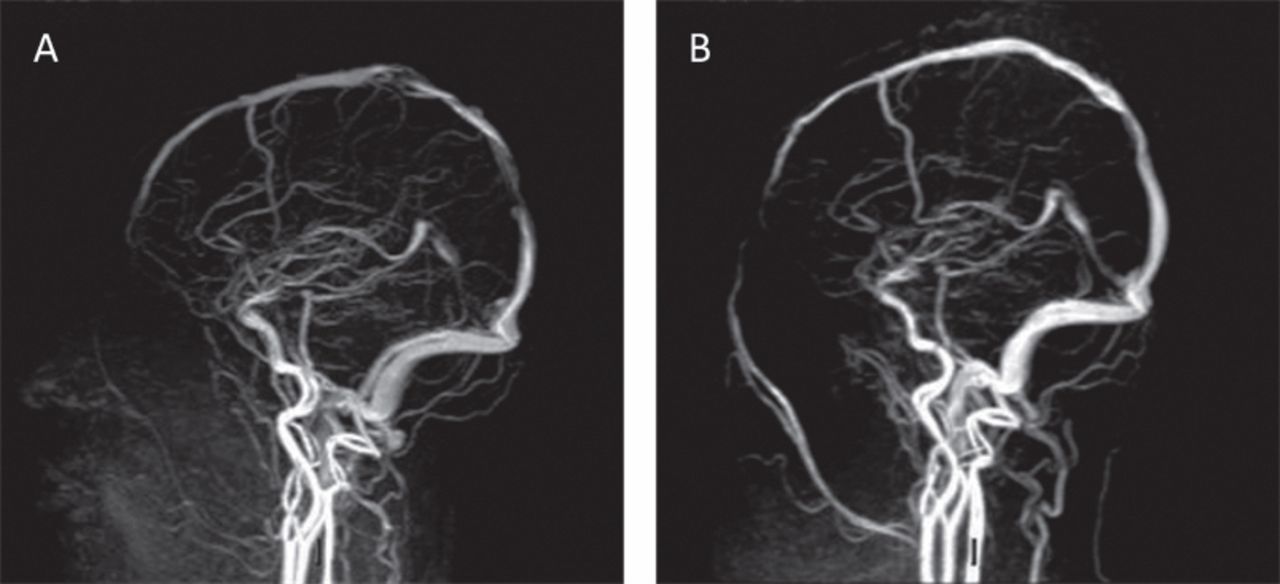
Magnetic resonance venogram. A – nearly complete occlusion of the distal segment of the superior sagittal sinus with thrombus at time of diagnosis. B – following anticoagulation therapy, there is reconstitution of flow within the sinus.
Case progression
Based on current Royal College of Physicians’ guidelines,4 anticoagulation therapy was started. The guidelines suggest warfarin; although in a patient with known variable adherence, decisions on anticoagulation must reflect their wishes and the need to optimise concordance. With previous poor attendance, at follow up, warfarin – with the requirement for regular monitoring – would be a high-risk strategy without proper safeguards in place. Although low molecular weight heparin injections would have alleviated the need for monitoring and could be administered in the community by a district nurse to ensure treatment was received, the patient declined long-term injections. A novel anticoagulant with oral administration and no need for regular monitoring would have been a simple solution but the potential interaction with ARVs precluded this.
Following discussion with the patient, inpatient warfarin loading, with the need for regular INR (International Normalised Ratio) monitoring clearly explained, was identified as a possible solution. The patient left hospital when the INR reached a therapeutic level. With text and telephone reminders, the patient attended for all scheduled appointments and completed the 6-month treatment course.
Discussion
Headaches are a common presenting complaint in HIV positive patients, and may be initially encountered by general physicians on the acute medical take. The differential diagnosis of headache, particularly with travel to a tropical region, is broad and the clinician will need to consider everything from the common causes of chronic headache in the immunocompetent to opportunistic disease occurring in advanced HIV. The clinical presentation, the blood CD4 count, and travel history and previous place of residence are all relevant and should be taken into account.
Although there is no specific guidance regarding the assessment of headache in an HIV positive patient, the British HIV Association guidelines outline the investigation of fever of unknown origin with neurological symptoms.4 Baseline investigations for any HIV patient presenting acutely should include a blood CD4 count (if not done within the last 3 months), full blood count, kidney and liver function and C-reactive protein, bacterial and fungal blood cultures, chest X-ray and electrocardiogram. If neurological symptoms are present, cryptococcal antigen should be checked and a CT head and/or MRI head (depending on test availability and local practice) should be performed. CSF should be obtained for analysis. In our centre, we perform microscopy and culture, mycobacterial smear and TB PCR, India ink microscopy for fungus, cryptococcal antigen, syphilis serology and viral PCR. It is recommended that, if possible, a total of 10 mL of CSF is obtained, with at least 7 mL being sent for mycobacterial culture. Flow cytometry for intracranial haematological malignancies can also be performed.
Although infectious or malignant causes of headache must be excluded as a priority, it is important to consider non-infectious causes of headache. A study of 200 patients with HIV found 53% reported headache symptoms, with 95% of these attributable to a primary headache syndrome (migraine or tension headache).5 A detailed history, careful examination and thorough initial investigation, with a high index of suspicion for rare but serious causes are therefore essential for the assessment of a HIV positive patient presenting with headache.
A 2012 Cochrane review6 of venous sinus thrombosis management concluded that anticoagulation was safe and could potentially reduce the risk of death or dependency. This is in line with the most recent American Stroke Association statement and current Royal College of Physicians guidelines,7 which suggest treatment with warfarin and low molecular weight heparin bridging unless contraindicated.
As with any treatment, it is vital that all possible steps are taken to optimise concordance. Without this engagement, the chance of long-term success is limited. As in the case presented, strategies to achieve this should be an integral part of the patient-centred, therapeutic approach.
Key learning points
The differential diagnosis of headache in HIV is broad. Infective and non-infective causes should be considered, with previous residence, travel history and degree of immunosuppression taken into account.
Where there is suspicion of intracranial infection, antimicrobial therapy should be promptly commenced with cover for viral, mycobacterial and fungal organisms as appropriate.
HIV is a risk factor for thrombosis. In an HIV positive patient with long-standing headache, venous sinus thrombosis should be included in the differential. An MRI brain can offer a diagnostic clue.
Current guidelines for the treatment of venous sinus thrombosis suggest anticoagulation with warfarin. Risks and benefits should be discussed with the patient and strategies to facilitate compliance put in place.
Conflicts of interests
The authors have no conflicts of interest to declare.
Acknowledgements
Written consent was obtained from the patient to publish the clinical details and images in this article.
- © Royal College of Physicians 2016. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.