
ABSTRACT
Drug-induced liver injury (DILI) remains the most common cause of acute liver failure (ALF) in the western world. Excluding paracetamol overdose, nearly all DILI encountered in the clinical setting is idiosyncratic in nature because affected individuals represent only a small proportion of those treated with such drugs. In many cases, the mechanism for idiosyncrasy is immune-mediation and is often identified by genetic risk determined by human leukocyte antigen variants. In the absence of diagnostic tests and/or biomarkers, the diagnosis of DILI requires a high index of suspicion after diligently excluding other causes of abnormal liver tests. Antibiotics are the class of drugs most frequently associated with idiosyncratic DILI, although recent studies indicate that herbal and dietary supplements are an increasingly recognised cause. It is imperative that upon development of DILI the culprit drug be discontinued, especially in the presence of elevated transaminases (aspartate aminotransferase/alanine aminotransferase ratio ≥5 times the upper limit of normal) and/or jaundice. Risk factors for the development ALF include hepatocellular DILI and female gender, the treatment being supportive with some benefit of N-acetylcysteine in the early stages. In view of the poor transplant-free survival in idiosyncratic DILI, early consideration for liver transplant is mandatory.
Introduction
At a regulatory level, drug-induced liver injury (DILI) is the commonest reason for withdrawing drugs from the market and/or issuing warnings and modification of use.1 DILI is classified as either predictable or unpredictable (idiosyncratic).2 The former tends to be dose-related, has a short latency (days), is due to direct toxicity of the drug or its metabolite, and is reproducible in animal models (eg paracetamol overdose).3 The vast majority of DILI, however, is idiosyncratic or unpredictable – it is unexpected based on the pharmacological actions of the drug and in most cases routine animal toxicology fails to identify the risk of subsequent clinical toxicity.4 This review shall largely focus on idiosyncratic DILI.
Epidemiology
Idiosyncratic DILI is an uncommon adverse event when taking prescription or non-prescription medications. It is difficult to assess the true incidence of DILI because of different diagnostic criteria and under reporting.5 However, recent population-based studies estimate the incidence to vary between 13.9–19.1 cases per 100,000 people per year.5,6
Data from prospective DILI registries suggest that antibiotics remain the most common cause of idiosyncratic DILI. The American DILI Network (DILIN) reported antibiotics to be implicated in 45.4% of cases.7 Other common drug classes reported by the American DILIN were herbal and dietary supplements (HDS; 16.1% – a significant increase over the last 10 years), cardiovascular agents (9.8%), central nervous system agents (9.1%), anti-neoplastic agents (5.5%) and analgesics (3.7%).7 Amoxicillin-clavulanate is the most common individual drug implicated in DILI as confirmed by both European and American studies (Table 1).6–10 In some Asian countries, however, HDS are implicated in more than 70% of all DILI.11
Common drugs implicated in idiosyncratic drug-induced liver injury according to studies from different countries
DILI includes the whole spectrum from asymptomatic elevation in liver tests to acute liver failure (ALF). In fact, DILI remains the most common cause of ALF in the UK12 and USA.13 Specifically, in the UK, paracetamol overdose causes approximately 57% of all ALF with non-paracetamol drugs accounting for a further 11%.12 In idiosyncratic DILI, approximately 4% progress to ALF; risk factors are female gender (70%) and hepatocellular DILI (80%).8 The drugs most commonly implicated in ALF include anti-tuberculosis therapies (ATT), HDS, sulpha-containing drugs, nitrofurantoin, phenytoin, sodium valproate, flutamide and amoxicillin-clavulanate.8,14
Types of DILI
Idiosyncratic DILI can be classified according to the pattern of liver tests observed – hepatocellular, cholestatic, or mixed. This classification was first established by the Council for International Organizations of Medical Sciences (CIOMS)15 and has recently been modified by the US Food and Drug Administration (FDA) Drug Hepatotoxicity Steering Committee.16 Hepatocellular DILI is characterised by an alanine aminotransferase (ALT) ≥3 times the upper limit of normal (ULN) and ALT/alkaline phosphatase (ALP) ratio ≥5 times ULN; cholestatic DILI by an ALP ≥2 times ULN and ALT/ALP ratio of ≤2 times ULN; and mixed DILI with ALT ≥3 times ULN, ALP ≥2 times ULN and ALT/ALP ratio <5 but >2 times ULN. Individual drugs have dispositions toward a characteristic clinical signature; however, exceptions do occur. For example, amoxicillin-clavulanate usually results in a cholestatic injury but less frequently has also been associated with ALF.17,18
Another way to classify idiosyncratic DILI is as immune-mediated (allergic) or non-immune mediated (non-allergic).19 If immune-mediated, the latency is shorter (1–6 weeks) compared with non-immune mediated reactions (1 month to 1 year).1,20 However, exceptions do occur with immune reactions appearing after a very long latency with drugs such as nitrofurantoin21 or even after drug cessation (eg sulfonamides, erythromycin and amoxicillin-clavulanate).20 Immune-mediated idiosyncratic reactions can be characterised by presence of fever, rash, eosinophilia, autoantibodies (such as antinuclear and anti-smooth muscle antibodies) and Stevens-Johnson syndrome. Non-immune mediated reactions lack the aforementioned characteristics and importantly, as described, tend to have a long latency period (1 month to 1 year).1,4,20
Other forms of DILI include steatohepatitis (amiodarone, tamoxifen, methotrexate),22 neoplasms (hepatic adenomas due to androgenic anabolic steroids (AAS)),23 and vascular (nodular regenerating hyperplasia due to azathioprine).24
Risk factors
Multiple factors have been found to be associated with an increased susceptibility to idiosyncratic DILI. The American DILIN found a higher prevalence of DILI in women (59% female versus 41% male),7 although this was not corroborated by the Spanish DILI registry (49% female versus 51% male).8 Potential reasons for increased female susceptibility to DILI include differences in various aspects of drug pharmacokinetics or pharmacodynamics; hormonal effects or interactions with immunomodulating agents or signaling molecules; and differences in the adverse response of the immune system to some drugs, reactive drug metabolites or drug-protein adducts.25 It is consistently observed, however, that women tend to be younger and develop hepatocellular DILI whereas men tend to be older and develop cholestatic DILI.7,26
Older patients have an almost threefold increase in the incidence of DILI as shown in a study from Iceland.6 This was attributed to the increased prescription rate of drugs in older patients.6 In general, higher drug dose and longer duration of therapy have also been implicated in poorer outcomes.26–28 In the Spanish Registry, 77% of patients with idiosyncratic DILI received medications with daily doses of ≥50 mg.26 Ninety percent of patients with serious DILI needing a liver transplant and reported to the Swedish Adverse Drug Reactions Advisory Committee were consuming ≥50 mg/day of the drug.27 A longer duration of drug therapy (135±31 days versus 53±3 days, p<0.0001)has been associated with a higher liver-related morbidity and mortality.29
It remains controversial as to whether pre-existing liver disease increases susceptibility to idiosyncratic DILI. In the American DILIN, 10% of patients with DILI had pre-existing liver disease, mostly due to hepatitis C and non-alcoholic fatty liver disease (NAFLD). This group was characterised by more severe liver injury and higher overall mortality (16% verus 5.2%, p<0.001) although they had similar liver-related mortality (57% versus 46%, p=0.5).7 The higher overall mortality in those with pre-existing liver disease may have been due to significantly higher prevalence of comorbidities, specifically diabetes mellitus (38% versus 23%, p=0.004).7 Additionally, alcohol excess and/or risk factors for NAFLD increase susceptibility to methotrexate toxicity by three- to fourfold.30 Furthermore, some studies have shown that patients with chronic hepatitis B or C could have a threefold increased risk of abnormal liver tests after receiving ATT.31,32 Nonetheless, the interpretation of liver injury in patients with chronic hepatitis B and C receiving ATT remains complex. It could be due to ATT-induced DILI, viral reactivation and/or immune reconstitution.33
Genetic factors also increase susceptibility to DILI. For example, human leukocyte antigen (HLA) B*5701 confers an eightyfold increased risk to flucloxacillin induced DILI, whereas the absence of this genotype has an 88% negative predictive value for flucloxacillin-related DILI.34
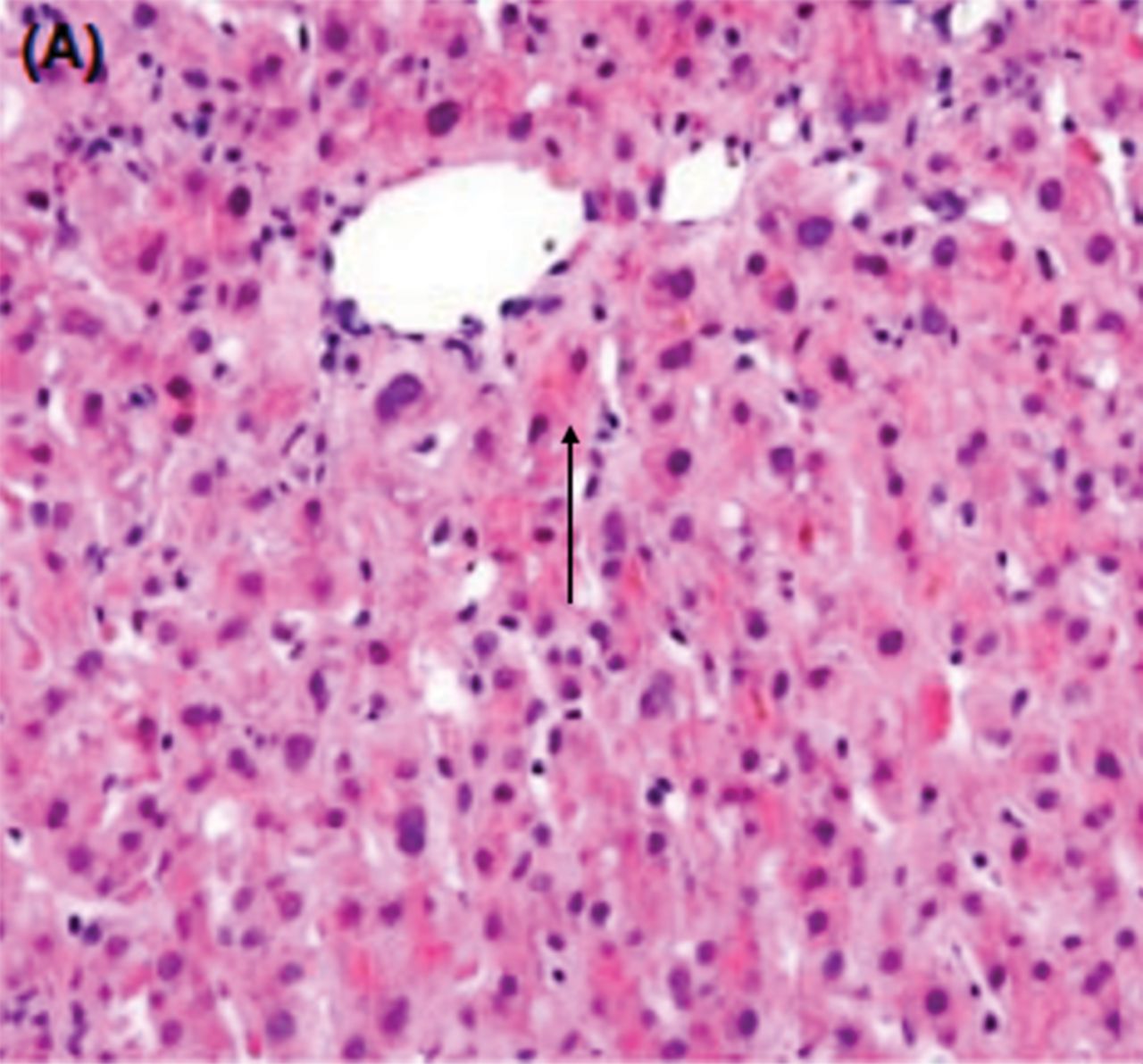
In case 1 (Box 1), we present a patient who could be considered to have flucloxacillin hepatotoxicity. However, unusual features were the young age, short duration of drug use and near normal gamma-glutamyl transferase despite significant hyperbilirubinaemia. A more detailed history revealed the use of the dietary supplement Massdrol (which is an AAS) prior to ingestion of flucloxacillin. A subsequent liver biopsy revealed bland cholestasis characteristic of AAS hepatotoxicity (Fig 1).35 His HLA genotype was B12/B42. HLA B*5701, which confers susceptibility to flucloxacillin-related hepatotoxicity,34 was not identified.
Three cases of drug-induced liver injury – what is the diagnosis and management?

Haematoxylin and eosin stain showing bland cholestasis due to androgenic anabolic steroid use with bile staining of hepatocytes (arrow) and Kupffer cell cytoplasm. Original magnification 200x. Reprinted with permission from El Sherrif et al.35
Pathogenesis
The pathogenesis of idiosyncratic DILI remains unknown but is most likely due to a complex interplay between drug (eg dose, duration of therapy, hepatic metabolism, lipophilicity) and host factors (eg age, gender, genetic polymorphisms). The drug may form a reactive metabolite that triggers DILI or may form covalent adducts with tissue proteins, eliciting an immune response and subsequent DILI.36,37
Natural history of DILI, and Hy’s Law
In the American DILIN, the presentation of DILI was with jaundice in 70% of cases. Most recovered after drug withdrawal; however, 17% progressed to chronic DILI (defined as abnormal liver tests for longer than 6 months) and 10% needed a liver transplant and/or died.7 Mortality increased to 44% in the presence of Stevens-Johnson syndrome.7 Compared with those with cholestatic DILI, those with hepatocellular DILI were more likely to require a liver transplant (6.2% versus 2.9%, p<0.001) and have fatal injury (9% versus 4%, p<0.001).7 Furthermore, use of non-body building HDS was associated with a significantly higher need for liver transplant compared with conventional drugs (13% versus 3%, p<0.05).38 Worryingly, 7% of cases were attributed to HDS during the first 2 years of the American DILI registry compared with 20% 10 years later.38 The American Acute Liver Failure Study Group (ALFSG) also recently reported that the prevalence of DILI-ALF/acute liver injury cases due to HDS increased between 1998–2007 and 2007–2015 (12.4 versus 21.1%, p=0.047). The HDS group had higher transplantation rates (56% versus 32%, p<0.005) and lower transplant-free survival (17% versus 34%, p=0.044) compared with those receiving conventional drugs.39
Specifically in hepatocellular DILI, a serum bilirubin of ≥3 times ULN in the absence of biliary obstruction or Gilbert’s syndrome is associated with a mortality of approximately 10% (range 5–50%).40 This is also known as Hy’s law, in recognition of the pioneering work done by Hyman Zimmerman – an American hepatologist. Hy’s law has now been confirmed by European and American prospective DILI registries.7,8 Hy’s law has also been adopted by the US FDA as a predictor of severe DILI during clinical trials, although in the interest of patient safety the FDA has lowered the hyperbilirubinaemia required to ≥2 times ULN (‘modified Hy’s Law’).40 The US FDA states that ‘finding one Hy’s law case in the clinical trial database is worrisome; finding two is considered highly predictive that the drug has the potential to cause severe DILI when given to a larger population’.40
Predicting those who are likely to develop ALF in idiosyncratic DILI is difficult and even the application of Hy’s law provides a specificity of only 44–67% and sensitivity of 83–90%.8 In an attempt to improve this, the Spanish DILIN developed a composite score to predict ALF: AST ≥17.3 times ULN; total bilirubin ≥6.6 times ULN; and AST:ALT ≥1.5 times ULN. These criteria are able to determine progression to ALF with a specificity of 82% and sensitivity of 80%.8 This composite score, however, needs to be validated in additional prospective studies.
Diagnosis
Since there are no diagnostic tests or biomarkers for idiosyncratic DILI, its diagnosis is made after stringently excluding other causes of liver disease, assessing the temporal association between use of drug and abnormal liver tests, looking for a characteristic clinical drug signature, and assessing improvement in liver tests upon drug withdrawal. Drug re-challenge is rarely indicated and cannot be advocated on ethical grounds. Nonetheless, one situation where a re-challenge may be justifiable is in the treatment of tuberculosis; however, this must only be done after carefully weighing the risks and benefits and in close liaison with a hepatologist.4 Finally, various causality assessment tools exist for DILI, of which the Roussel Uclaf Causality Assessment Method is the most used although it is far from perfect.41
Liver biopsy can be helpful in certain situations, particularly to exclude other causes of liver disease (eg alcohol, NAFLD). It also has a role if ‘drug-induced’ autoimmune hepatitis (AIH) is suspected and needs differentiating from idiosyncratic DILI.42 Portal and intra-acinar plasma cells, rosette formation and emperiopolesis are histological features that favour AIH (p<0.02), whereas portal neutrophils and intracellular (hepatocellular) cholestasis are more prevalent in DILI (p<0.02; Table 2).42 Nonetheless, this differentiation is based on retrospective data and, in the real world, differentiating ‘drug-induced AIH’ from idiosyncratic DILI may be far more difficult.
Comparison of idiosyncratic DILI, ‘drug-induced’ autoimmune hepatitis and idiopathic autoimmune hepatitis46–49
In case 2 (Box 1), a subsequent liver biopsy confirmed cirrhosis with lymphoplasmacytic portal inflammation and interface hepatitis. This was suggestive of AIH. While statins have been associated with DILI, including ‘drug-induced’ AIH,43 it would have been very unusual for the statin to result in cirrhosis, especially within a year.43 This patient most likely had an underlying propensity to develop idiopathic AIH and the statin either unmasked or triggered this, or was an innocent bystander. She was treated with corticosteroids and azathioprine with good response.
Management of DILI
Prompt cessation of the culprit drug as soon as DILI is suspected is of paramount importance. There are also therapies for specific causes of DILI; for example, N-acetylcysteine (NAC) for paracetamol overdose44 and L-carnitine for valproic acid overdose.45
Corticosteroid therapy in DILI has a limited role and is reserved for those with immune-mediated DILI or ‘drug-induced’ AIH. The former may only need a short course of steroids, whereas the latter, which is often indistinguishable from idiopathic AIH, often requires prolonged courses of steroids and/or additional immunosuppression.46–49 As already stated, differentiating DILI from ‘drug-induced’ AIH can often be difficult and in such situations, after careful assessment of risks and benefits, a trial of corticosteroids may be warranted. Although ursodeoxycholic acid is often used in cholestatic DILI, its use remains non-evidence based.50
Acute liver failure
Case 3 (Box 1) presents a patient who has developed ALF. Pegylated interferon alpha use has not been associated with ALF. Hepatitis B and C flares were excluded by negative polymerase chain reaction; therefore, the most likely cause was clarithromycin-induced ALF. Clarithromycin has been associated with cholestatic DILI, particularly in older patients, and ALF has been reported.51 This patient was urgently listed for a liver transplant but unfortunately developed progressive cerebral oedema and died before he could receive a transplant.
Spontaneous survival with ALF secondary to idiosyncratic DILI (non-paracetamol) is poor with only 27.1% of patients alive at 3 weeks,14 in contrast to paracetamol-induced ALF where spontaneous survival is 64–66%.52 Therefore, it is crucial that, especially in idiosyncratic DILI, early discussion with a tertiary liver centre takes place at the first hint of ALF (worsening jaundice, coagulopathy (international normalised ratio >1.5) or development of hepatic encephalopathy (HE)). With transplantation the overall survival increases to 66.2%, which demonstrates the necessity to rapidly identify those with ALF due to idiosyncratic DILI.8 The King’s College criteria are most commonly used to prioritise patients with paracetamol and idiosyncratic DILI for liver transplant.53,54
Two earlier randomised controlled trials (RCTs) showed no benefit of corticosteroids in ALF and even demonstrated a poorer outcome in those with DILI.55,56 A more recent study from the ALFSG corroborated this, showing no improvement in overall survival in drug-induced, indeterminate or autoimmune ALF (61% versus 66%, p=0.41).57 In fact, lower survival was observed in those patients with the highest model for end stage liver disease scores (>40) after corticosteroid therapy (30% versus 57%, p=0.03).57
NAC has a well-established role in paracetamol-induced ALF44 although it is now also recommended in selected cases of non-paracetamol ALF. A 2009 RCT in patients with non-paracetamol ALF demonstrated similar 3-week survival for patients given NAC versus placebo (70% versus 66%, p=0.283).58 However, transplant-free survival was significantly better for patients who received NAC compared with placebo (40% versus 27%, p=0.043), but this was confined to those with early HE (52% versus 30%, p=0.010); whereas those with grade 3–4 HE had no benefit with NAC (9% versus 22%, p=0.912).58 DILI was the most prevalent aetiology of ALF within this study.
Conclusion
DILI includes the whole spectrum from asymptomatic and transient elevation in liver tests to ALF. DILI due to paracetamol overdose and idiosyncratic drug reactions remain the most common causes of ALF in the western world. DILI is a diagnosis of exclusion and there is an urgent need to develop diagnostic biomarkers. Antimicrobials remain the most common cause of idiosyncratic DILI although recent studies show a significant increase in DILI due to herbal and dietary supplements. Hepatocellular DILI is more likely to progress to ALF compared with cholestatic or mixed DILI. The management of DILI is symptomatic with prompt cessation of the culprit drug and early referral for liver transplant upon the development of ALF, especially in those with idiosyncratic DILI.
Conflicts of interest
The authors declare no conflicts of interest related to this manuscript.
- © Royal College of Physicians 2016. All rights reserved.
References








{kind=link}
Jump to section
Related Articles
Cited By...
- Severe azathioprine-induced liver injury 22 months after initiation of treatment
- Development of a novel in silico classification model to assess reactive metabolite formation in the cysteine trapping assay and investigation of important substructures
- Severe azathioprine-induced liver injury 22 months after initiation of treatment
- Risk of Abemaciclib-induced Liver Injury in Hormone Receptor-positive, HER2-negative Metastatic Breast Cancer: A Retrospective Analysis
- dialogi: Utilising NLP with chemical and disease similarities to drive the identification of Drug-Induced Liver Injury literature