
ABSTRACT
In the UK, there are over 80,000 admissions annually with acute coronary syndromes (ACS). Management of ST-elevation myocardial infarction (STEMI) involves primary percutaneous coronary intervention (PCI), which is delivered via dedicated heart attack centres. Non-ST elevation-ACS (NSTE-ACS) accounts for two-thirds of ACS presentations, affecting an older cohort of patients – often with more complex comorbidities. Initial management is with anti-thrombotic therapy with a view to PCI within 24 hours for the most acute cases and within 72 hours for all others. However, varying management pathways and access to specialist cardiology services results in variable times to definitive treatment. Advances in the sensitivity of cardiac biomarkers and the use of risk assessment tools now enable rapid diagnosis within a few hours of symptom onset. Advances in invasive management and drug therapy have resulted in improved clinical outcomes with resultant decline in mortality associated with ACS.
Introduction
Coronary artery disease (CAD) remains the leading cause of death worldwide.1 Clinical manifestations include stable angina, acute coronary syndromes (ACS), heart failure and sudden death. The term ACS encompasses ST-elevation myocardial infarction (STEMI) and non-ST elevation ACS (NSTE-ACS), which encompasses non-ST elevation myocardial infarction (NSTEMI) and unstable angina (UA). Approximately two thirds of ACS presentations are with NSTE-ACS and the remainder are STEMI.2,3 Furthermore, with the advent of high sensitivity troponin assays, many patients previously classified as UA are now being diagnosed with NSTEMI. This has resulted in the incidence of UA to fall while NSTEMI is on the rise.3 While the age- and sex-adjusted incidence of ACS is falling, there remains an associated mortality risk with the condition.2 In the UK, there are over 80,000 hospital admissions with ACS annually.3 Those presenting with STEMI tend to be younger (average age 65 years) compared with patients with NSTE-ACS (average age 71 years),3 who also frequently have multi-vessel coronary disease and more complex comorbidities. In the UK, the 30-day mortality associated with STEMI is 8.1%.3 1-year mortality is higher for patients presenting with NSTE-ACS compared with STEMI (14.3% versus 9.5%) reflecting the fact that while patients presenting with NSTE-ACS appear more stable at presentation, their long-term outcome is worse.4,5
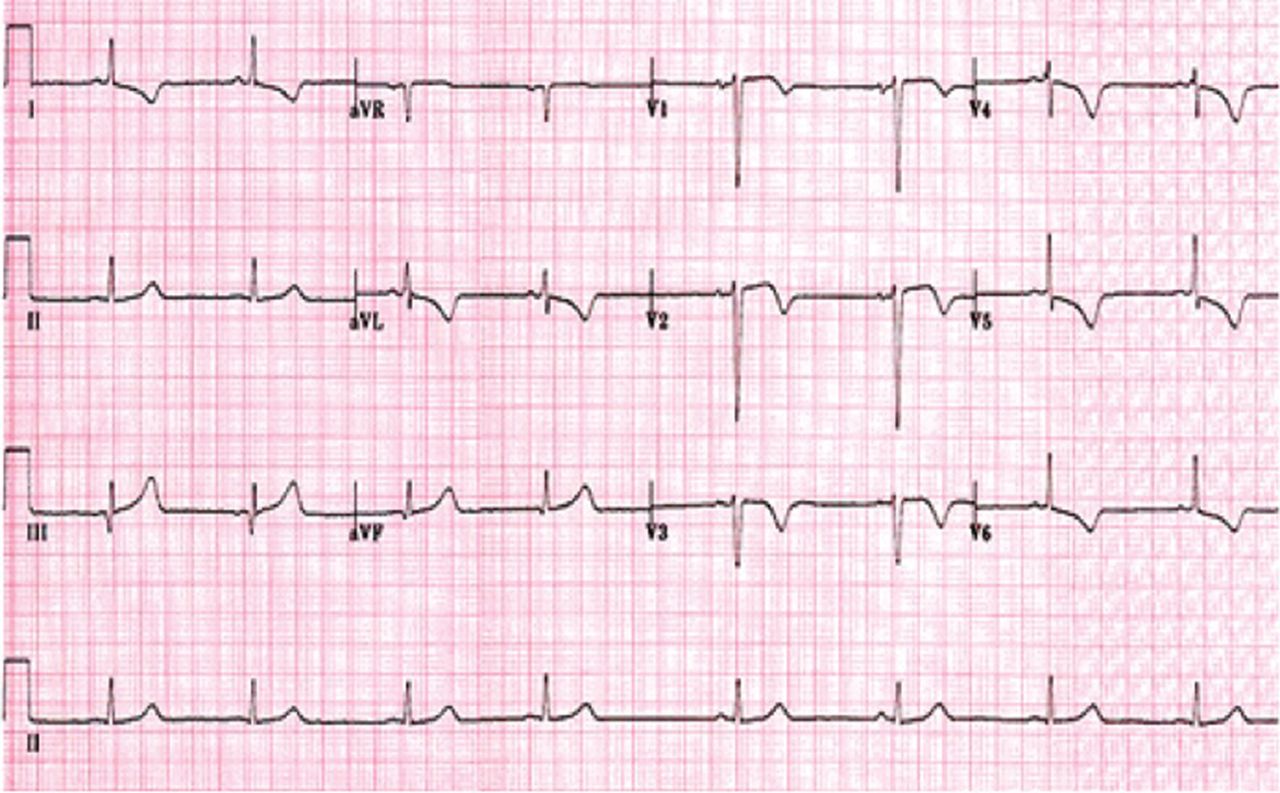
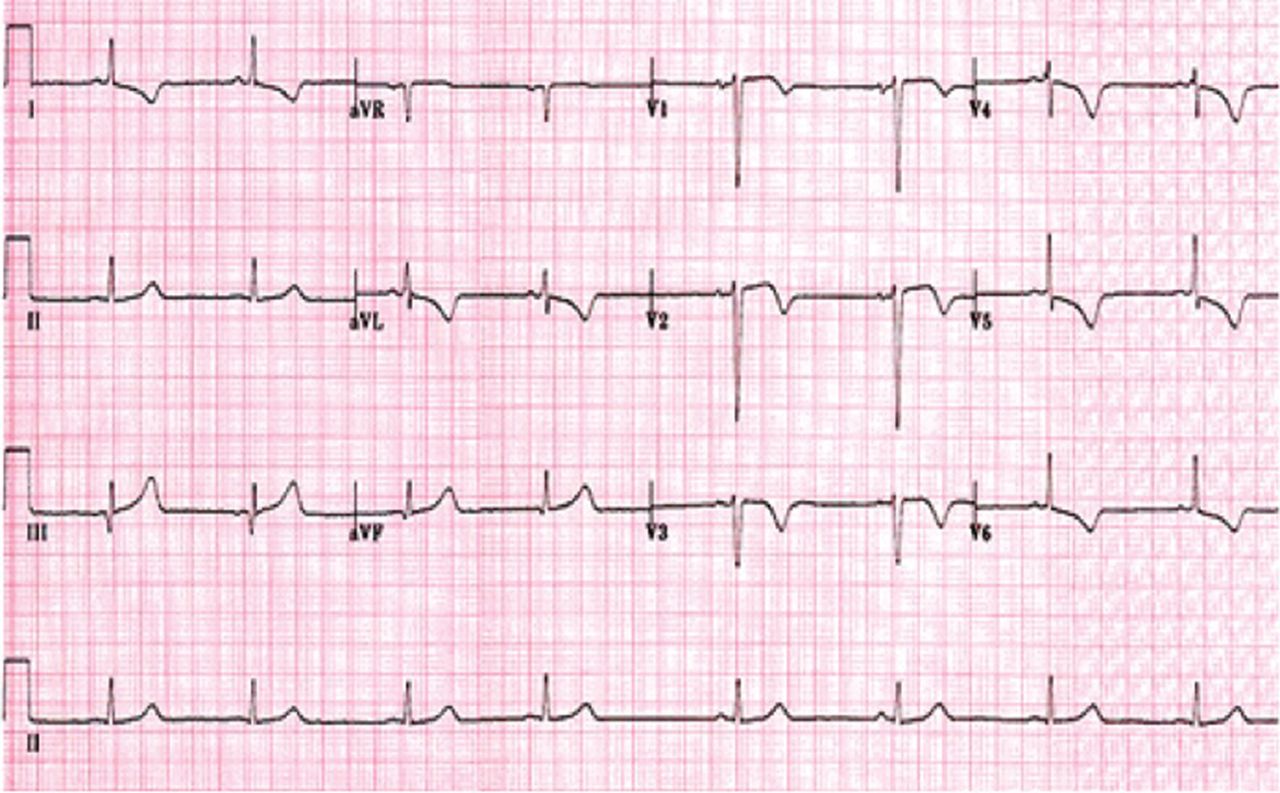
The standard of care for patients presenting with ACS includes early coronary angiography with a view to revascularisation with percutaneous coronary intervention (PCI) or coronary artery bypass surgery (CABG). Patients with STEMI typically present acutely with severe ongoing cardiac chest pain and ST elevation on 12-lead electrocardiogram (ECG) (Fig 1). In the UK, there is an established STEMI pathway, whereby patients are taken by the ambulance service directly to a heart attack centre where they receive immediate PCI (Fig 2). Patients with NSTE-ACS usually present more insidiously and are commonly seen in the local emergency department. This may not be a PCI-capable centre and patients are frequently admitted under the general medical team rather than directly under cardiology. This may introduce delays in care before the patient receives definitive treatment.

Example of 12-lead electrocardiogram showing ST-segment elevation in the inferior leads (II, III and aVF) with reciprocal ST-segment depression in leads V1–V4, I and aVL.

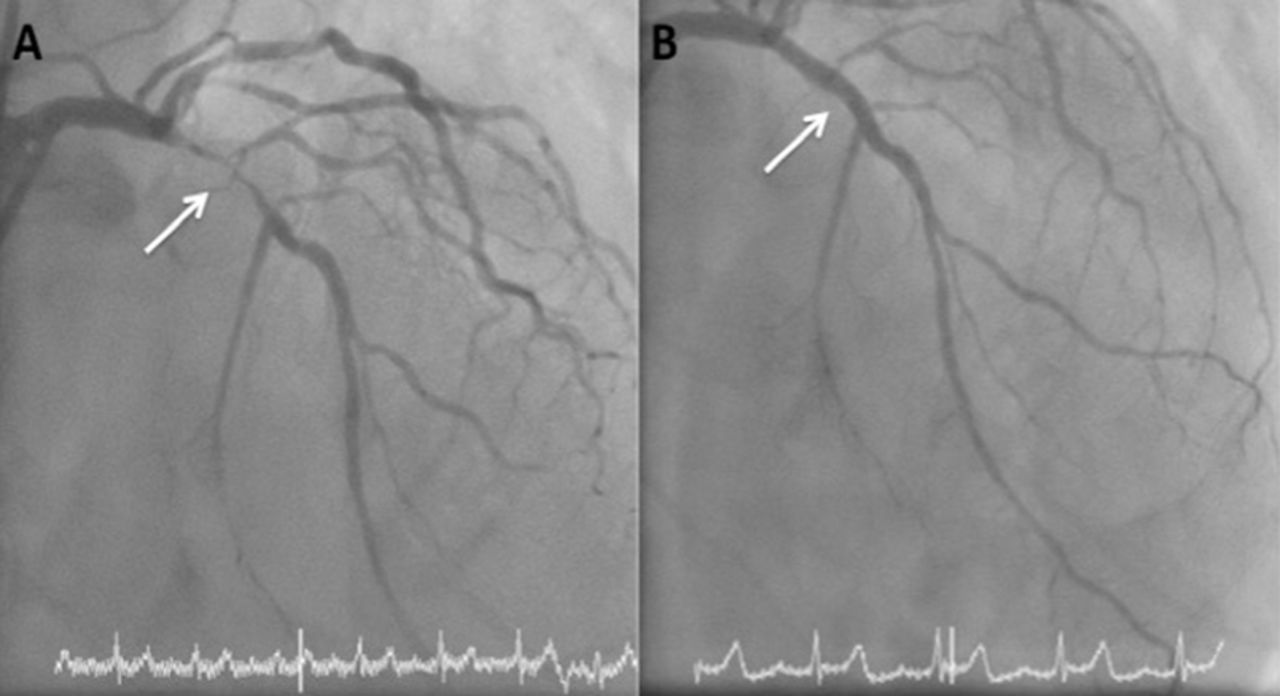
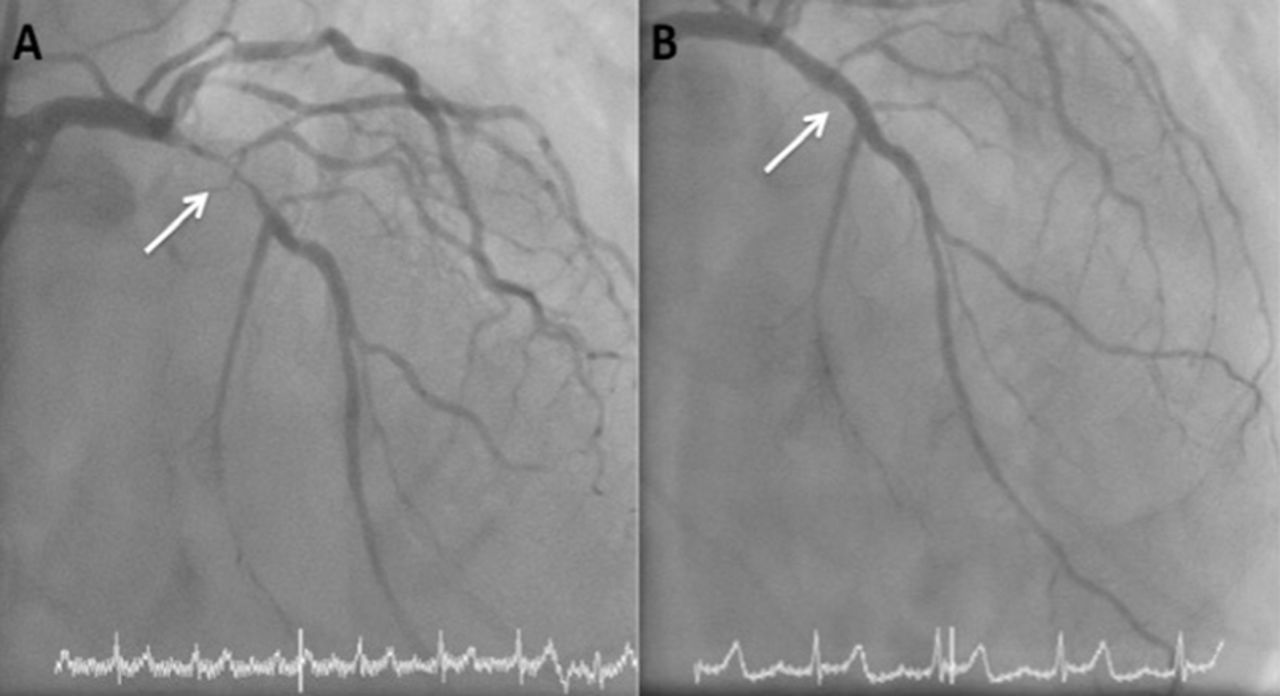
Coronary angiogram of patient presenting with inferior ST-elevation myocardial infarction. A – occluded right coronary artery (arrow); B – successful restoration flow following implantation of a drug-eluted stent.
Universal definition of myocardial infarction
In 2012, the third universal definition of myocardial infarction was published.6 This update reflects the increasing sensitivity of biochemical assays and the additional use of imaging modalities to diagnose myocardial infarction. The term myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting consistent with acute myocardial ischaemia. There should be a rise and/or fall of cardiac biomarker value (preferably cardiac troponin) with at least one of the following:
symptoms of ischaemia
new or presumed new significant ST segment or T wave changes, or new left bundle branch block
development of pathological Q waves on ECG
imaging evidence of new loss of viable myocardium or new regional wall motion abnormality
identification of intracoronary thrombus on angiography or autopsy.
Furthermore, myocardial infarction can be further classified into five subtypes according to underlying aetiology (Box 1). In clinical practice, type 1 (spontaneous myocardial infarction), and type 2 (secondary to ischaemic imbalance) are the most commonly encountered. The use of imaging, such as echocardiography or cardiovascular magnetic resonance, can be useful to differentiate the two as type 2 is not usually associated with loss of viable myocardium or regional wall motion abnormality.
Subtypes of myocardial infarction6
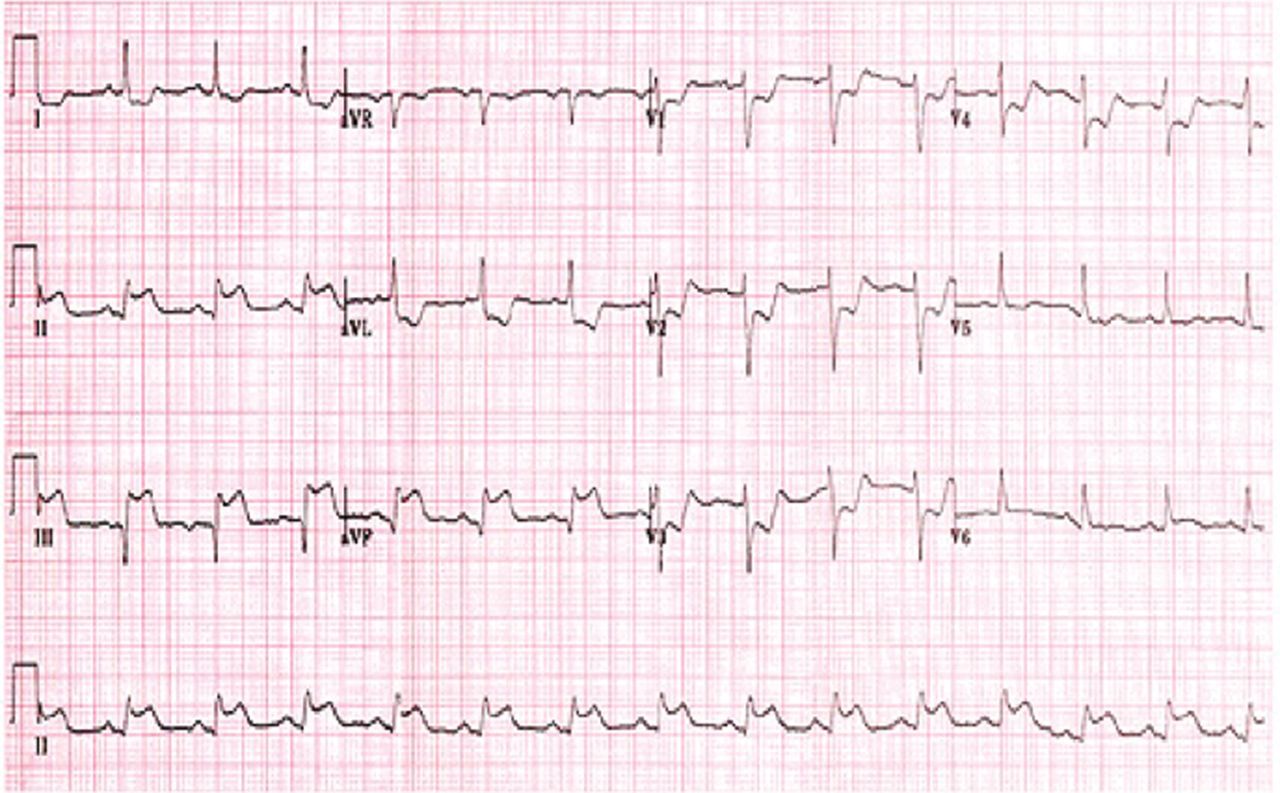
The term ACS encompasses a clinical spectrum of pathophysiology and presentations of symptomatic coronary disease. This is usually due to atherosclerotic plaque rupture, ulceration or erosion that results in intraluminal thrombus formation and compromises myocardial blood flow leading to myocardial necrosis and release of cardiac enzymes. Usually, STEMI is a manifestation of complete vessel occlusion due to acute thrombus formation secondary to a ruptured plaque. If left untreated, this results in transmural infarction and extensive myocardial necrosis. Characteristically, the 12-lead ECG shows ST-segment elevation localised to an epicardial vessel territory. In contrast, NSTE-ACS results from incomplete or transient vessel occlusion. The 12-lead ECG may show ST segment depression, T wave inversion, or be completely normal (Fig 3). NSTEMI is associated with release of cardiac enzymes such as troponin signifying a degree of myocardial necrosis, whereas UA has no enzyme release but the presence of worsening or crescendo symptoms. This differentiation of subtypes of ACS is often used clinically as it allows for diversion of patients to different treatment pathways according to clinical urgency.
Example of 12-lead electrocardiogram showing antero-lateral T wave inversion (leads V2–V6, I and aVL) consistent with non-ST elevation-acute coronary syndrome.
Non-ST elevation acute coronary syndrome
NSTE-ACS may precede STEMI or sudden cardiac death. Despite often relatively short-lived symptoms that respond to medical therapy with nitrates and opioids, the risk of death or STEMI in the first 30 days is up to 10%.7 Up to half of patients will experience recurrent ischaemia despite initiation of medical therapy.8,9 The main determinants of prognosis are extent of myocardial injury, extent of coronary artery disease and instability of disease.
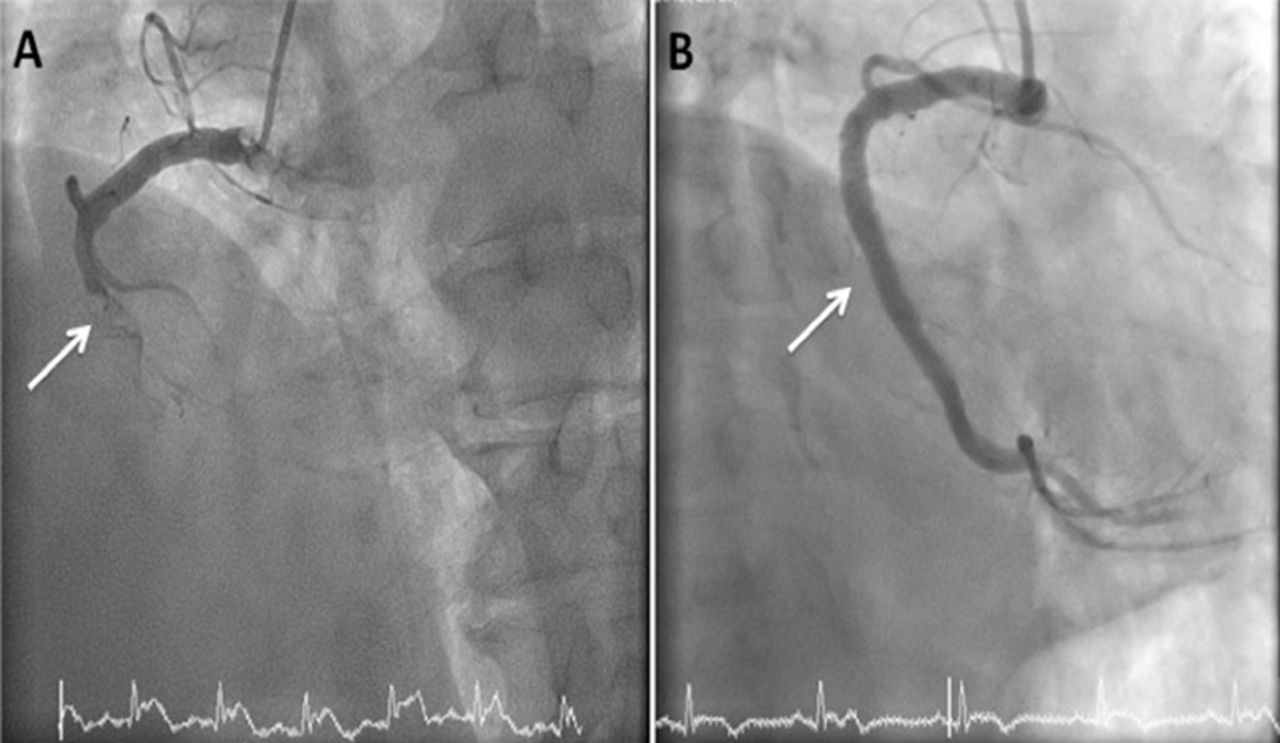
Initial assessment of patients with suspected NSTE-ACS is often performed by emergency department or general medical physicians. It is important that patients at high risk or those with ongoing ischaemia receive urgent cardiology review and definitive treatment with coronary angiography and PCI (Fig 4).
Coronary angiogram of a patient presenting with non-ST elevation-acute coronary syndrome. Electrocardiogram showed anterior T wave inversion. A – critical stenosis in proximal left anterior descending artery (arrow); B – successful restoration of flow following implantation of a drug-eluted stent.
Diagnosis is made from a combination of clinical history, ECG changes and cardiac troponin release. Troponin is a component of the myocardial contractile apparatus that is released from damaged myocytes. It is not detectable in healthy subjects. There are a number of commercially available assays, most of which test for troponin T or troponin I. Normal ranges can vary significantly between assays. Furthermore, some manufacturers also quote different cut-off values for males and females. A number of studies have demonstrated that elevated troponin is associated with increased risk of mortality.7,10 More recently, high sensitivity troponin assays have become available, allowing for early diagnosis and ‘early rule out’ of NSTEMI within 3 hours of onset of chest pain when used appropriately.11,12
While there is often a reliance on cardiac troponin, it is important to remember that a number of patients may have unstable coronary disease without troponin release. It is therefore important that the result is put into clinical context. Additionally, troponin may be falsely elevated in conditions such as renal failure, pulmonary embolism, myocarditis and heart failure. Serial testing at presentation then again after 3 hours is now incorporated in many guidelines. Dynamic rise in troponin (with or without signs and symptoms of myocardial ischaemia) is consistent with a diagnosis of myocardial infarction, whereas no change (even if elevated above upper limit of normal) should prompt investigation for alternative diagnoses.13 For high sensitivity troponin assays, a fivefold increase has greater than 90% positive predictive value for detection of myocardial infarction, whereas a three fold increase has a positive predictive value of only 50–60%.14 The next generation of troponin assays have the potential to diagnose myocardial infarction within 1 hour and are already in use in some centres.15 These are commonly used in conjunction with risk scores and, as long as the sample is collected more than 2 hours after onset of symptoms, may allow for rapid discharge of patients without ACS.
A number of risk scoring systems have been developed to highlight those at highest risk and in need of urgent intervention. The two most commonly used are GRACE (Global Registry of Acute Coronary Events) and TIMI (Thrombolysis in Myocardial Infarction). GRACE is based on a multinational registry of over 70,000 patients admitted with ACS.16 The primary endpoint was all-cause mortality at 6 months. From this, nine predictors of mortality were derived (Box 2). Points are allocated to each of the predictors to give an overall score, which correlates to an in-hospital and 6-month mortality risk. A GRACE score above 140 is defined as high risk and associated with more than 2.8% risk of in-hospital death.16 An early invasive strategy with coronary angiography within 24 hours has been shown to be better than a delayed strategy (more than 36 hours) for patients within this group.17
Predictors of 6-month mortality following ACS16
Current UK and European guidelines recommend inpatient coronary angiography for patients presenting with NSTE-ACS. Timing is based on assessment of risk (Box 3). National Institute for Health and Care Excellence (NICE) guidelines recommend urgent coronary angiography within 24 hours for patients who are clinically unstable, for example those with ongoing chest pain, and within 72 hours for all other patients.18 European Society of Cardiology guidelines recommend urgent coronary angiography within 2 hours for patients with refractory angina, associated heart failure, ventricular arrhythmia or haemodynamic instability, an early invasive strategy (within 24 hours) for those with a GRACE score greater than 140, and coronary angiography within 72 hours for those with low to intermediate risk.13
Recommendations for timing of coronary angiography NSTE-ACS according to clinical risk
Contemporary UK data suggest there is room for improvement in timely access to coronary angiography. In 2014, only 54% of patients presenting with NSTEMI underwent coronary angiography within 72 hours and 67% within 96 hours.3 These figures are likely to be as a consequence of many patients being admitted to hospitals without coronary intervention facilities and with lack of access to early cardiology specialist input. Centres have introduced novel pathways to expedite access to coronary angiography. Examples include
direct referral of selected patients from the emergency department in district general hospitals to the cardiology team at the closest heart attack centre with a 24-hour PCI service
direct access for the ambulance service to the heart attack centre for patients with high-risk NSTE-ACS.19
ST-elevation myocardial infarction
Primary PCI is now established as the optimal revascularisation method for STEMI in the UK. This is as a result of data showing improved mortality, non-fatal myocardial infarction and stroke compared with fibrinolysis.20 This is based on the ability to deliver primary PCI in a timely manner. Where primary PCI cannot be reliably delivered within 120 minutes, fibrinolysis may still be considered as an option. Heart attack centres have been set up to rapidly mobilise staff and deliver immediate treatment upon arrival of the patient. Every minute treatment is delayed results in myocardial damage and consequent increased risk of mortality. A door-to-balloon time of 30 minutes is associated with 3% in-hospital mortality compared with 6% mortality at 120 minutes and 9% at 180 minutes.21 In the UK, more than 90% of patients receive primary PCI within 90 minutes of admission to a heart attack centre.3 Door-to-balloon (and call-to-balloon) times can be reduced by ambulance crews delivering patients directly to the cardiac catheterisation laboratory rather than admitting via the emergency department.22
The majority of routine and primary PCI in the UK is now undertaken via the radial rather than femoral route. This has been shown to reduce mortality and complications such as major bleeding.23,24 It also allows for early mobilisation and discharge, and is generally preferred by patients.
Antiplatelet therapy
A key pathological feature of acute coronary syndrome is platelet activation, which results in thrombin generation, activation of the coagulation cascade and release of inflammatory mediators.25 Anti-thrombotic pharmacotherapy is therefore an important adjunct to PCI and an integral part of secondary prevention.
The mainstay of acute and long-term management includes aspirin and a P2Y12 inhibitor, such as clopidogrel or ticagrelor. Clopidogrel is a thienopyridine drug that results in irreversible platelet inhibition. It is a pro-drug with an onset of action of 2–4 hours and duration of effect of up to 10 days. Ticagrelor is a new P2Y12 inhibitor that does not require metabolism to an active metabolite. It causes reversible platelet inhibition and has a rapid onset of action (approximately 30 minutes). This is theoretically advantageous in the acute phase where rapid platelet inhibition is required. The duration of effect is 3–4 days. The CURE (Clopidogrel in Unstable angina to prevent Recurrent Events) study initially showed benefit for clopidogrel in addition to aspirin in reducing cardiovascular death, myocardial infarction and stroke for patients with ACS.26 More recently, the PLATO (PLATelet inhibition and patient Outcomes) study showed benefit for ticagrelor over clopidogrel for the same endpoints without a significant increase in major bleeding.27 However, there was an increase in non-major bleeding with ticagrelor. Cangrelor is a new intravenous reversible antiplatelet agent. It has a rapid onset within a few minutes and duration of effect of 1–2 hours. While not currently used in routine practice in the UK, it has shown potential in the acute phase of STEMI where rapid platelet inhibition is required.28
Current guidelines recommend dual antiplatelet therapy for 1 year following ACS.13 This was partly based on the risk of stent thrombosis with early generation drug eluting stents. However, there is now a move towards tailored antiplatelet therapy according to the clinical need and bleeding risk of the individual patient. The recent DAPT (Dual Antiplatelet Therapy) study showed that dual antiplatelet therapy beyond 1 year (compared with aspirin alone) after implantation of a drug eluting stent significantly reduced the risk of stent thrombosis and major adverse cardiovascular and cerebrovascular events but with an associated increase in risk of bleeding.29 This bleeding risk is highest in older patients, those with existing coagulation defects and those with comorbidities, including liver and renal failure. With the introduction of new generation drug eluting stents, there is emerging evidence for the safety of shortening dual antiplatelet therapy to as little as 1 month.30 Therefore, selected patients with high cardiovascular risk or recurrent events may benefit from prolonged antiplatelet therapy beyond 1 year whereas those with lower cardiovascular risk and/or high bleeding risk may be treated with a shorter course of dual antiplatelet therapy.
Anticoagulant therapy
In addition to antiplatelet therapy, low molecular weight heparins are recommended in the acute phase of NSTE-ACS prior to angiography. Commonly used agents include enoxaparin, dalteparin and tinzaparin. The factor Xa inhibitor fondaparinux is now preferred in many centres as it has been shown to be non-inferior to enoxaparin with 50% reduced bleeding risk.31 Anticoagulation is not routinely prescribed long term following ACS. However, there is evidence that novel anticoagulants (NOAC), such as rivaroxaban, improve outcomes following ACS; this is at the expense of increased bleeding.32 NICE currently recommends the addition of rivaroxaban in selected high-risk patients.33
A subset of patients presenting with ACS may have another indication for long-term anticoagulation, such as atrial fibrillation. Triple therapy with aspirin, clopidogrel and warfarin (or NOAC) is associated with a significantly increased bleeding risk compared with dual antiplatelet therapy.34 However, effective platelet inhibition is essential in the early phase following PCI to reduce the risk of early stent thrombosis. It is therefore suggested that patients with low bleeding risk are treated with triple therapy for 6 months following PCI, followed by dual therapy with warfarin (or NOAC) plus aspirin or clopidogrel for another 6 months.13 Patients with high bleeding risk should be treated with triple therapy for 1 month, followed by warfarin (or NOAC) plus aspirin or clopidogrel for the remainder of the year.13 After 1 year, treatment with warfarin (or NOAC) alone is recommended.
Conclusions
ACS is a common presentation to acute services. There is a clearly defined treatment pathway for STEMI with direct admission to heart attack centres with a view to emergency PCI. NSTE-ACS is a more common presentation of ACS, affecting an older cohort of patients – often with more complex comorbidities. Management pathways vary, resulting in variable times to cardiology review and definitive treatment. Initial management is with anti-thrombotic therapy with a view to PCI in a timely manner. Advances in the sensitivity of cardiac biomarkers and risk assessment tools now enable rapid diagnosis within a few hours of symptoms onset. Advances in invasive management and drug therapy have resulted in improved short-term and long-term clinical outcomes.
Conflicts of interest
The authors have no conflicts of interest to declare.
- © Royal College of Physicians 2016. All rights reserved.
References








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.