
ABSTRACT
In this article, we briefly describe some of the challenges in delivering a stroke service in the NHS in England and how we have overcome them. Current issues are considered and research prospects described. We show that providing excellent stroke care is as much about organising services as it is about medical intervention.
Introduction
Stroke care has changed out of all recognition in the last 20 years. From being a marginalised field with little research-based evidence, it has become one of the fastest growing specialties and is now recognised as requiring an acute commitment, dedicated organisation and tight quality control. There is exciting research being carried out and the specialty benefits from its broad multidisciplinary base and mix of acute, rehabilitation and preventative aspects. This article will briefly cover some of the challenges that face stroke services and how we have attempted to deal with them. We have divided these into acute, rehabilitation, prevention and future developments.
Acute
Thrombolysis
Thrombolysis with alteplase is now firmly entrenched as an evidence-based treatment for hyperacute cerebral infarction. Recently, the balance between benefits and risks was called into question.1 During 2015, an expert working group of the UK’s Commission on Human Medicines reviewed the use of alteplase in stroke.2 It provided firm reassurance that it is safe and effective for use up to 4.5 hours after the onset of symptoms. The earlier the treatment is given, the greater the chance of a more favourable outcome. Data from the Royal College of Physicians’ (RCP) Sentinel Stroke National Audit Programme (SSNAP) showed that about one in nine patients in the UK are now being treated, although this varies considerably by centre. Unfortunately, many hospitals in England and Wales are still not delivering this treatment effectively. Over 40% of hospitals had median door-to-needle times of over 1 hour and only 22% had a median within 45 minutes (Fig 1). The national median time has improved by only 6 minutes in 2 years.3
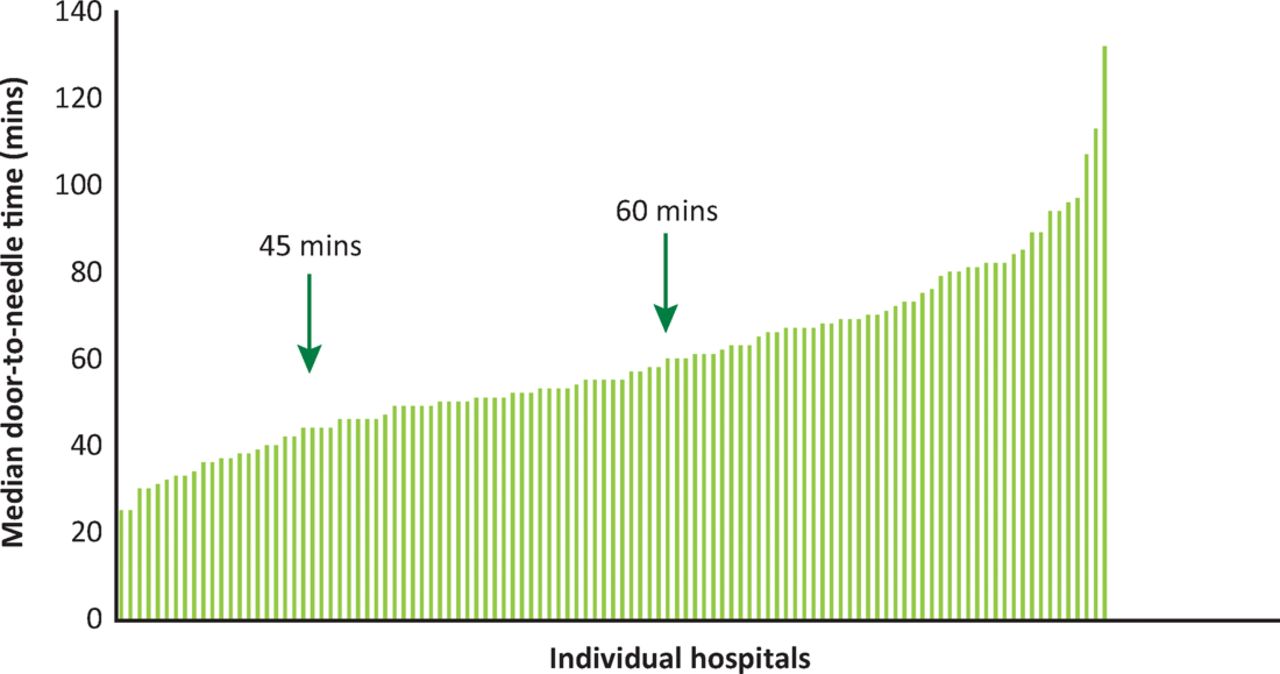
Individual hospitals’ median door-to-needle time for stroke thrombolysis reported to the Royal College of Physicians Sentinel Stroke National Audit Programme (SSNAP) 2015.
Reducing door-to-needle time
For stroke teams to significantly reduce their door-to-needle time, they need to consider every step in the pathway and adopt a ‘lean’ approach to minimise delay. Our protocol at Northwick Park Hospital is that the stroke team – a dedicated band 6 nurse and a junior doctor – respond to a pre-alert by ambulance control of a stroke emergency call by meeting patients at the door of the emergency department. They examine patients and take their history on the ambulance trolley without undressing them more than is absolutely necessary and do not do a textbook neurological examination, an electrocardiogram or connect them to a cardiac monitor. Observations, including blood glucose, done by the ambulance team are not repeated. We have shown by analysis of every stage of the pathway that these activities, while being routine in other medical emergencies, are not necessary for the diagnosis of stroke and add up to 10 minutes to the assessment process.4 All of the equipment for thrombolysis, including a dedicated, portable point-of-care international normalised ratio testing machine, infusion pumps, alteplase, labetalol for blood pressure control and drugs to manage anaphylaxis are kept in a dedicated trolley. A complete duplicate kit is in a rucksack that can be carried to any part of the hospital; this eliminates time spent looking for equipment. We have written telephone scripts, which must be learnt by every team member. The decision-maker, always a consultant, is phoned and information given in a structured way. Because the team are very experienced, the consultant does not usually have to see the patient themselves but often does so, especially in working hours for teaching purposes. The computerised tomography (CT) is also reported locally, which saves the time downloading it to the consultant’s home computer. We have developed escalation protocols to deal with every eventuality we have encountered, such as scanner or consultant unavailability, loss of mobile phone signal or loss of mains power. Our team has rehearsed multiple scenarios of what might go wrong or take extra time. We review all cases monthly with the whole team. At these meetings we analyse: every case with a door-to-needle time outside our 30 minute target; cases with the shortest times, to learn from good practice; and every complication. The names of team members for each case are available. This fosters a spirit of competition but also allows targeted training if required. We audit individual performances continuously at nurse, junior doctor and consultant level. This audit is critical to the process because it can give an early warning if someone on the team needs more training or there is a problem with the pathway. Importantly, analysis of outcomes also confirms the safety of time-saving measures. We have been able to show that thrombolysis without the consultant being present is safe, providing juniors and radiologists are well trained and can spot anything out of the ordinary. We have just invested in clinical decision-making support software,5 which automatically calculates the Alberta Stroke Program Early CT Score (ASPECTS).6 This will reduce reliance on radiologists and enable decision-makers to view scans securely on their mobile phones to save time logging in to the trust intranet for borderline cases.
An internal hospital campaign to reduce door-to-needle time needs the investment of time to train staff, but this is the only way that effective treatment can be given. Once a culture of rapid treatment exists it becomes self-sustaining as team members pass on both expertise and expectations to newcomers. We have now maintained a median door-to-needle time of less than 30 minutes for several years, despite staff changes.
Thrombectomy
Intravenous thrombolysis may not work for patients with a large or proximal vessel occlusion. Thrombectomy using a stent retriever is a possible treatment in these patients. A flurry of trials published in 2015, and reviewed in a meta-analysis,7 demonstrated that thrombectomy works in selected patients. Table 1 provides a very brief summary of these trials and the patients studied.
Patient characteristics in five thrombectomy trials7
Thrombectomy is very resource-intensive. It requires the constant availability of specialists in neurological intervention, an equipped catheter laboratory and anaesthetics support. This is not available in most UK hospitals at the moment and most of those with the appropriate infrastructure can provide a service only during restricted hours.8 Using the eligibility criteria from the trials above, we have estimated that over a 3-month period around 9% of our patients would have been suitable for thrombectomy.9 It is therefore not practical to take every stroke patient to a thrombectomy centre.
The challenge for the stroke community is to build services to provide for stroke patients who may come at any time of the day and to write local protocols setting out exactly which patients are suitable for referral and how to transfer them quickly to a hospital where thrombectomy is available. The NHS will need to consider how to resource this evidence-based treatment and to train and employ the specialists required.
The slow and incomplete implementation of intravenous thrombolysis and the challenge of providing thrombectomy services are two examples of why delivering high-quality stroke care is not just about clinical medicine. It requires doctors to be managers, competent at re-designing and implementing services and learning how to deliver them to all eligible patients.
Stroke unit assessment and rehabilitation
Even among patients ineligible for thrombolysis, admission to a stroke unit is beneficial. Management on a stroke unit reduces mortality10 and allows full assessment by the multidisciplinary team. However, SSNAP audit data also suggest that many hospitals are struggling to admit stroke patients promptly to their stroke unit. Admission should not be disrupted by hospital bed management issues. We find it is beneficial to remind hospital management at chief executive and director level that ensuring stroke patients are admitted directly to a stroke unit is backed by powerful evidence. We take every opportunity to do this and ask them to leave bed managers in no doubt as to their responsibility to ensure this happens.
7-day working
From inception, the London Stroke Project mandated daily consultant ward rounds on hyperacute stroke units (HASUs). This has limited impact without 7-day therapy services. The national clinical guideline for stroke11 recommends a minimum of 45 minutes of each appropriate therapy that is required, for a minimum of 5 days a week. In practice, it is almost impossible to meet this target without 6- or 7-day services. In 2013, we implemented 7-day services for physio- and occupational therapy and 6-day services for speech therapy and psychology. Although initially resisted by therapists, we found that it significantly reduced their burden of work after weekends and public holidays and gave them a day off in the week. A recent local survey found that most would not choose to return to their previous pattern of work. Implementation does need extra funding if it is not to detract from weekday services. This cost may potentially be recovered by reducing length of stay.
Cognitive impairment
Cognitive impairment is frequently recognised in older people with stroke and is also common in younger people. However, it may be missed in patients who recover mobility and speech rapidly and are discharged from hospital quickly to community services without a full cognitive assessment. Missing such impairment can be costly, not only in personal terms, but also by reducing the patient’s ability to return to work. Standard measures should be used to screen every stroke patient for cognitive problems. If deficits are discovered, this should lead to full assessment by a neuropsychologist. Suitable screening tests include the Montreal Cognitive Assessment12 and the Oxford Cognitive Screen.13
Most cognitive tests have some limitations as they were developed in non-stroke settings. The questions and responses require speech and language skills that are impaired in many stroke patients. The Northwick Park Examination of Cognition14 is designed to overcome these limitations by employing multiple input (verbal, visual) and output (spoken, written, gesture) modalities to ensure accessibility for stroke patients with a range of cognitive deficits and lesion locations. It includes 21 brief subtests in the domains of reasoning, episodic memory, language, perception and attention/executive function. In experienced hands, it takes about 20 minutes to administer.
Prevention: atrial fibrillation
Atrial fibrillation (AF) still poses many unanswered questions for stroke physicians. One current debate is whether to give anticoagulants to people with AF and borderline risk scores.15 However, as so often happens, the biggest problem is getting accepted guidelines into practice. A large Swedish study showed that 5% of a screened general population had untreated AF;16 in another study, only 36% of people aged ≥85 years with AF were appropriately anticoagulated.17 All physicians have a responsibility to question local practice, educate other practitioners and identify patients who have not already been considered for preventative treatment.
For patients with AF who have had a recent stroke, there is little evidence to guide when anticoagulation should be started and which agents should be used. Conventionally, anticoagulation is not started for 2 weeks after an infarct but some physicians start earlier, especially if the infarct is small and the patient ready to go home. A pilot study to see whether anticoagulants should be restarted when a cerebral haemorrhage occurs during treatment for AF has just been approved.18
Future developments
Hyperacute management
Although intravenous thrombolysis and embolectomy are now evidence based, there are many stroke patients who are not suitable or do not respond to these procedures. This has led to some creative projects looking at ways of treating acute stroke.
Stimulation of the sphenopalatine ganglion is known to increase cerebral blood flow on the stimulated side. An innovative way of doing this19 is currently being evaluated. It involves placing an electrode via the mouth, which can then be used to stimulate the ganglion. The system is in worldwide trials.
Another innovative trial looks at ways of enhancing the efficacy of intravenous thrombolysis using magnetic nanoparticles injected at the same time.20 These ‘stir’ the column of static blood at the site of a thrombosis and may help thrombolytic drugs to dissolve larger clots.
Acute hypothermia, used in traumatic brain injury, is being explored in stroke. A pan-European randomised trial, EuroHYP 1,21 is using a variety of systems to induce hypothermia. Recruitment is progressing steadily. The systems can be used outside the conventional intensive care setting and may therefore be suitable for specialist hyperacute stroke units.
Swallowing
Unsafe swallowing is a problem affecting about 15% of stroke patients. Instrumental assessment is becoming more widespread and is leading to changes in what patients can swallow safely. A free water protocol, which allows patients to sip unrestricted water, contributes to wellbeing without any evidence of harm.22 We now have several months of experience using this protocol and are currently assessing its impact on the incidence of chest infections. However, RCP guidelines9 continue to recommend that such patients are kept nil by mouth.
Pharyngeal electrical stimulation is a treatment designed to help the brain develop alternative swallowing pathways when the usual pathways are damaged. There is evidence from magnetic resonance studies that this treatment has potential but the amount, frequency, timing and duration of treatment is not known. A randomised, sham-controlled trial of a novel pharyngeal stimulation device to stimulate swallowing recovery23 was negative but has given useful information to guide future studies and remains an exciting area for further research.
Rehabilitation
In rehabilitation, a trial to evaluate robot assisted training for the upper limb after stroke (RATULS)24 looks at ways of increasing patient participation in upper limb therapy. It has had wide publicity and has recruited over 300 participants at four centres in the UK.
Conclusions
Stroke is an exciting area of medicine. There is scope for those interested in acute care, rehabilitation, the organisation of services and prevention. There are many research studies using technical innovations and the horizons are broad. The field is still wide open for enterprising physicians to make a difference.
Conflicts of interest
The authors have no conflicts of interest to declare.
- © Royal College of Physicians 2016. All rights reserved.
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.