
ABSTRACT
Ischaemic stroke is a treatable medical emergency. In an era of time-dependent reperfusion techniques, it is crucial that an accurate and prompt diagnosis is made. Approximately 30% of patients admitted to hyperacute stroke units are subsequently found not to have a final diagnosis of acute stroke although some of these patients do have incidental or previously symptomatic cerebrovascular disease. These patients do not benefit from thrombolysis and may require the input of other specialists or treatments. Meanwhile, a proportion of patients with acute stroke have unusual presentations and are sometimes initially admitted to general medical admissions units prior to accessing stroke unit care. It is important that atypical presentations of stroke are recognised so that patients are not denied the benefits of stroke unit care and secondary prevention. This article describes some characteristics of common stroke mimics and chameleons, considers how to avoid diagnostic mistakes and discusses the contributory role of imaging.
Key points
Stroke should be suspected in any patient with sudden onset neurological symptoms, confusion or falls even if the symptoms initially appear to be unusual for stroke
Common stroke mimics include seizure, migraine, sepsis, syncope, and metabolic and functional disorders
Administering thrombolysis to mimics should be avoided although the risk of adverse effects is low
Stroke can present as a chameleon with confusion, reduced conscious level or non-specific symptoms such as vertigo, unsteadiness and reduced conscious level
Negative CT does not exclude stroke; MRI can help in cases of diagnostic uncertainty as diffusion restriction is highly sensitive for acute ischaemia.
Introduction and epidemiology
The term ‘stroke mimic’ is an umbrella term rather than a diagnosis. It is used once acute stroke has been excluded and a more convincing explanation has instead been found for a clinical presentation that was initially felt to reflect acute ischaemic stroke. Conversely, ischaemic stroke can masquerade as an alternative condition: the ‘stroke chameleon’. Rapid diagnostic accuracy is especially important when a patient is eligible for reperfusion therapies. The Face Arm Speech Test (FAST)1 and the ROSIER (Recognition Of Stroke In the Emergency Room)2 scale have been designed for use by ambulance and emergency department staff, respectively, who are the usual first point of contact for these patients. While both these stroke recognition tools aim to facilitate rapid identification of stroke, they are not infallible and false negatives and false positives do occur. A 2015 systematic review demonstrated that FAST had a sensitivity of 79–97% and specificity of 13–88% while the sensitivity of the ROSIER scale was 83–97% with a specificity of 18–93%.3 In the context of pre-hospital recognition of stroke, the ROSIER scale has not been shown to be superior to FAST and therefore FAST remains the most widely used screening test in the UK.4
The incidence of stroke mimic can be as high as 30% but varies depending on the clinical setting and the expertise of those assessing the patient.5 Unsurprisingly, factors associated with the greatest odds of having a stroke mimic include a lack of cardiovascular risk factors such as hypertension, hyperlipidaemia or atrial fibrillation.5 In a study of the bedside clinical assessment of suspected stroke, Hand et al6 showed that an exact time of onset, definite focal symptoms, a high National Institute of Health Stroke Scale (NIHSS) score, being able to lateralise the signs to the right or left side of the brain and being able to determine a clinical stroke syndrome predicted a stroke, while cognitive impairment and abnormal signs in other systems predicted a mimic.6
In a 2016 US single hospital retrospective chart review, 20% of strokes were initially ‘missed’ although these data have limited generalisability to an entire healthcare system such as the NHS in the UK.7 If the diagnosis of acute stroke continues to go unrecognised in patients who are initially admitted to general admissions units, the opportunity for secondary prevention can be lost. These patients can have delayed access to stroke unit care, which conveys an increased likelihood of being alive, home-dwelling and independent at 1 year.8 It has been suggested that this group has higher rates of readmission at 60 days and disability and mortality at 12 months.7,9
Stroke mimics
Seizure, syncope, sepsis, migraine, space-occupying lesions, functional disorders and metabolic conditions are the seven most frequent differential diagnoses of suspected stroke.10 Computerised tomography (CT) imaging can identify some space-occupying lesions and hypoglycaemia is detectable with bedside glucose monitoring. However, not all mimics are readily identifiable.
Seizures
Seizure accounts for 20% of mimics.10 The development of a focal weakness after seizures was described by Robert Bentley Todd in 1849 and is thought to occur through over-activity and subsequent exhaustion of the primary motor cortex. When other areas of the brain are affected by seizure, other transient deficits can manifest, such as dysphasia, sensory symptoms or visual field deficits. Post-ictal paresis is common, occurring in 13.4% of a selected group of 513 patients undergoing video-electroencephalogram monitoring and lasting up to 22 minutes.11 In clinical experience, the duration is often hours and can infrequently be days. While recurrent stereotyped symptoms or a history of epilepsy is suggestive of Todd's paresis, the presence of a focal neurological deficit in association with a first seizure is more challenging as 1.8–2.9% of patients with ischaemic stroke have seizures at onset or within the first 24 hours.12,13 Seizure remains a relative contraindication to thrombolysis as such patients were excluded from the initial trials to prevent improvements in post-ictal paresis being mistaken for a drug effect.14
Sepsis and syncope
Patients with ‘deconditioning’ of previous stroke or subclinical cerebrovascular disease may mimic acute stroke and can display an exacerbation of previous deficits. Syncope and sepsis are important triggers although the mechanism is not always hypoperfusion. Careful collateral histories obtained from carers or details from previous medical records can differentiate this from recurrent stroke. In the case of sepsis, there are often clues from the history, signs of systemic illness on examination and raised inflammatory markers. However, both sepsis and stroke are common and dual pathology can exist, for example in a patient with stroke and aspiration pneumonia.15 Sepsis can also induce a hypercoagulable state and predispose to cerebral infarction.16 Loss of consciousness is, as a general rule, unusual in stroke.
Migraine
Migraine accounts for 9% of stroke mimics.10 20–30% of migraines are associated with aura; this is often visual but patients can develop transient motor, speech or sensory symptoms. Typically, migraine aura is spreading rather than apoplectic in onset and there may be a prodromal phase prior to developing aura and headache, with patients reporting symptoms such as tiredness, irritability, nausea, yawning and difficulty concentrating.17 However, migraine (particularly migraine with aura) itself is associated with a twofold increase in the relative risk of ischaemic stroke when patients with migraine were compared with non-migraineurs.18 It is also recognised that headache can form part of ischaemic stroke symptomatology with data from an Israeli registry showing that 8.4% of 2001 patients with ischaemic stroke had headache at onset although this proportion was higher at 27% in an Austrian registry.19,20 Differentiating acute stroke from migraine can, therefore, sometimes be difficult and may require time and magnetic resonance imaging (MRI).
Where does this leave the physician assessing the patient in the emergency department? Patients with mimics, particularly seizure and sepsis, may present within the timeframe for decisions about reperfusion therapies.6 Although stroke mimics are common, some reassurance can be obtained from the finding that these patients are infrequently given intravenous thrombolysis and adverse events are rare, with two cohorts of thrombolysed patients demonstrating mimic frequencies of 1.8% and 10% and rates of symptomatic intracranial haemorrhage of only 1% compared with 7.9% in ischaemic stroke.21,22
Missed diagnoses and stroke chameleons
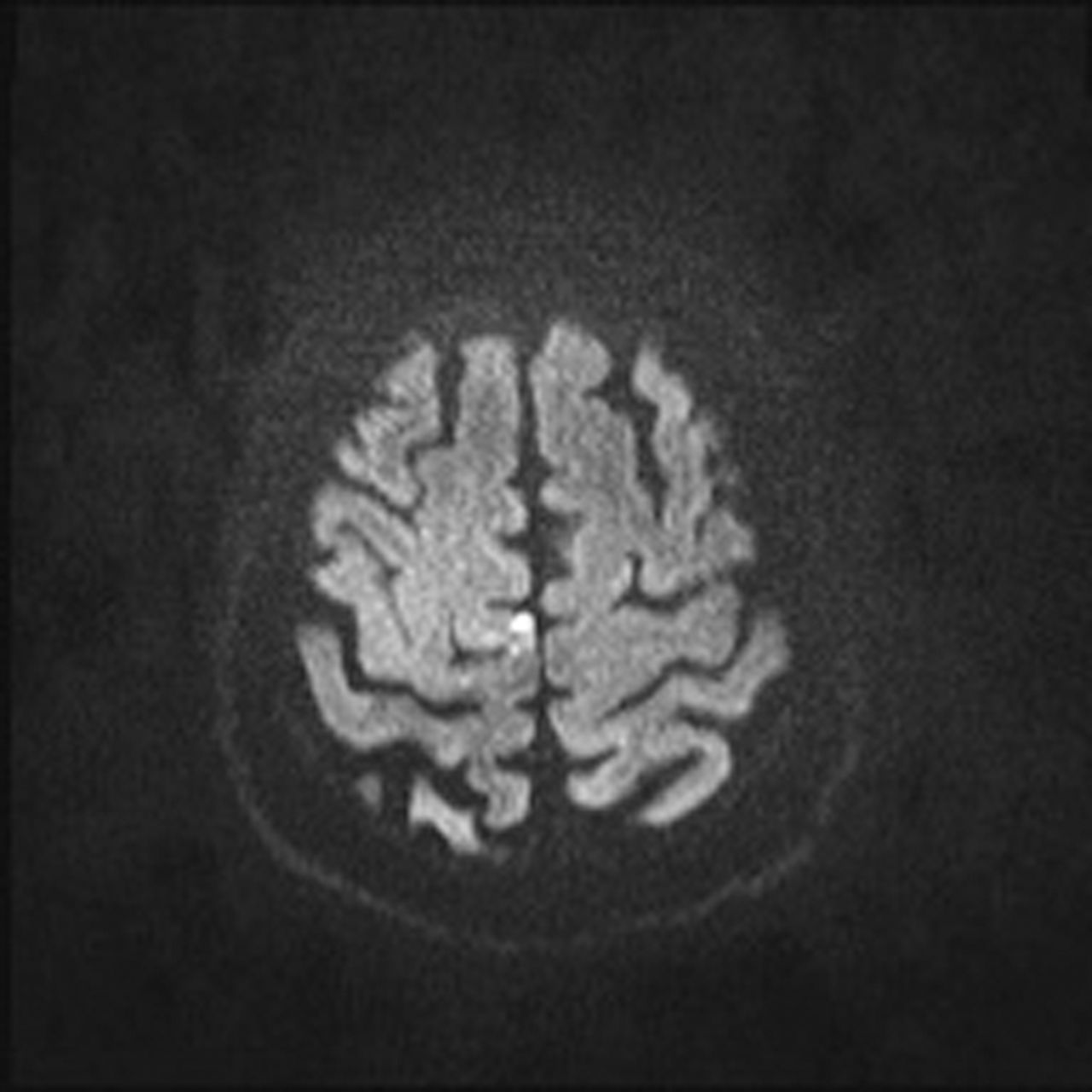
A 72-year-old man presented to the emergency department having woken up with a left foot drop. On examination there was weakness of left dorsiflexion but intact sensation. As he had suffered low back pain in the past it was initially felt that the weakness was consistent with a left L4/L5 radiculopathy but spinal MRI showed only minor degenerative change at this level. Careful re-examination demonstrated several beats of clonus and an up-going Babinski reflex on the left, so brain MRI was arranged. This confirmed a small acute infarction in the right motor strip (Fig 1), corresponding to the area represented by the foot. Stroke can rarely present with very restricted deficits that may superficially resemble mononeuropathy or radiculopathy without skilled history and examination. The clue to the diagnosis in this case was the abrupt onset of symptoms. Stroke should be suspected in all older patients with sudden onset neurological symptoms even if these are atypical for stroke. The cause of small cortical infarction is often a small emboli from a carotid source, in this case a right internal carotid artery dissection (Fig 2).23,24 However, cardioembolism can also be responsible.
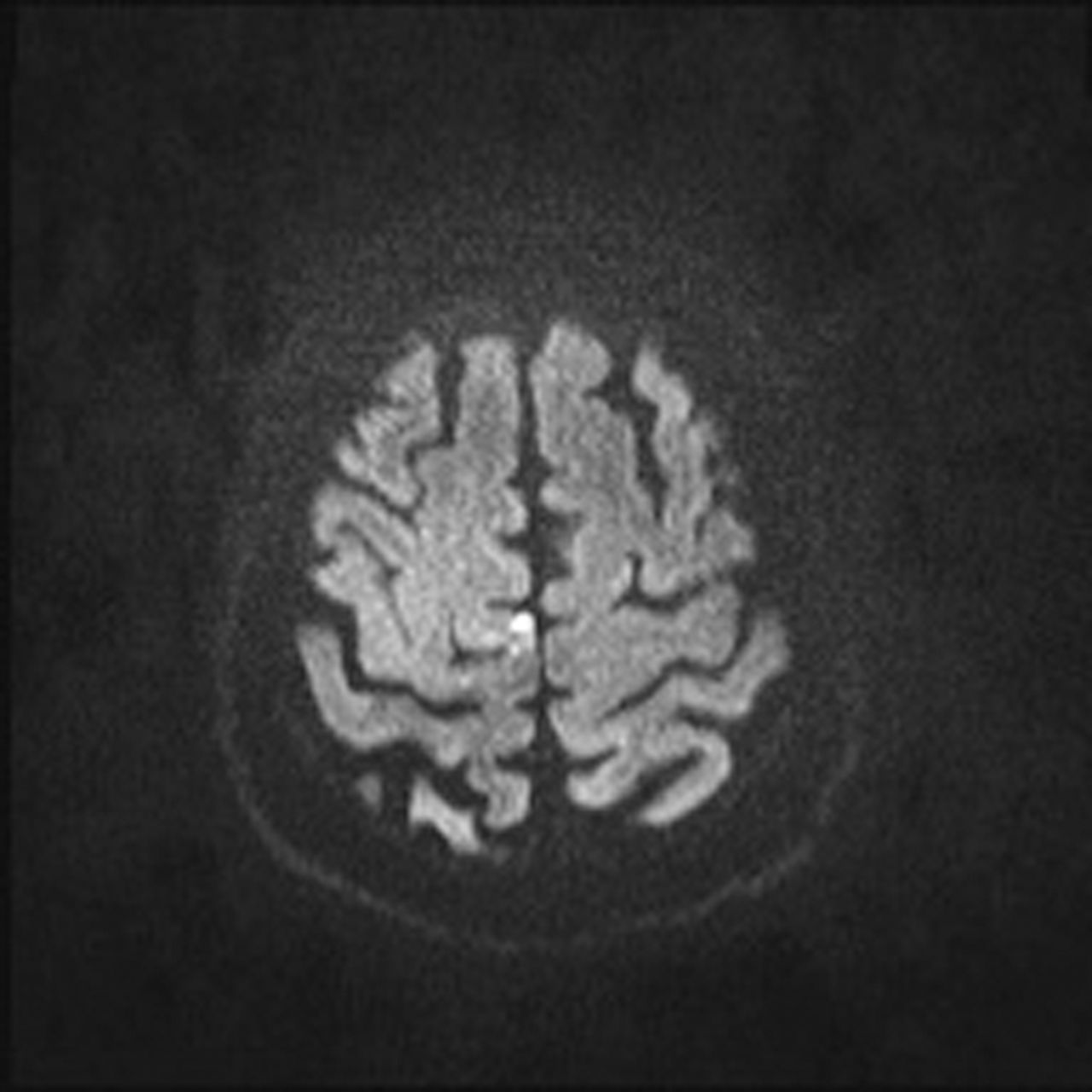
Brain magnetic resonance image demonstrating a small area of restricted diffusion in the right primary motor cortex.

Computerised tomography angiogram demonstrating dissection at the origin of the right internal carotid artery.
Although stroke can be mistaken for a peripheral nerve or root lesion, the most common conditions for which stroke is mistaken are delirium, syncope, hypertensive emergencies or systemic infection.25 The risk of misdiagnosis is higher in younger patients and those with either mild symptoms or coma.9 In a recent analysis, 37% of posterior circulation strokes were initially missed compared with 16% of anterior circulation strokes, probably as patients presented with ‘non-traditional’ symptoms of confusion, altered gait and dizziness rather than conventional lateralising signs.7,26
Acute vertigo
Dizziness, unsteadiness and vertigo are common symptoms in the emergency department and on the medical take. The differential diagnosis includes posterior circulation stroke although most patients have more benign causes for their symptoms. In a US population-based study, Kerber et al27 showed that 3.2% (53/1,666)of patients with symptoms of dizziness, imbalance and vertigo were diagnosed with stroke or transient ischaemic attack. Only 0.7% of the 1,297 patients presenting with isolated dizziness in this study were found to have stroke or transient ischaemic attack.27 It is important to differentiate non-specific, often transient ‘dizziness’ from more persistent acute isolated vertigo with vomiting (acute vestibular syndrome). This group is frequently discharged from accident and emergency with a diagnosis of viral labyrinthitis although as many as 25% may have cerebellar infarction.28 Clearly, making the diagnosis in these patients is a challenge. The three-step bedside oculomotor examination HiNTS (Head impulse, Nystagmus, Test of Skew) can help to some extent here.29 The presence of a negative head impulse test, direction-changing or vertical nystagmus, or skew deviation (vertical ocular misalignment on alternate cover testing) has been shown to have 100% sensitivity and 96% specificity for stroke.29
Decreased level of consciousness
Decreased level of consciousness is common in acutely unwell patients with subclinical subcortical cerebrovascular disease. However, it is important to recognise some of the distinct but rare stroke syndromes that cause abrupt changes in conscious level. The ‘top of the basilar’ syndrome is caused by occlusion of the distal portion of the basilar artery; patients can present with unconsciousness and quadriplegia.30 Abnormalities of the pupils and oculomotor signs provide clues but usually CT or magnetic resonance angiography is required to confirm the diagnosis.30 Impaired consciousness can also occur with bilateral thalamic infarcts, usually in association with vertical gaze palsies, and can be caused by occlusion of the artery of Percheron, a normal variant where the blood supply to both paramedian thalamic territories arises from one posterior cerebral artery.31
Acute confusional state
Strokes affecting the non-dominant inferior parietal lobe, non-dominant temporal gyrus or occipital lobe can present with confusion, agitation or restlessness and can be mistaken for delirium.30 Similarly, vertebrobasilar ischaemia causing thalamic infarcts can lead to sudden onset confusion with memory loss.30 The key to diagnosis here is that few other causes of delirium present so acutely; witnesses may report the patient being asymptomatic one moment and then confused the next.
Severe hypertension
An acute hypertensive response is not unusual in the first 24 hours after stroke. In a large American dataset of 276,734 patients with acute ischaemic stroke, nearly 50% of patients had a systolic or diastolic blood pressure greater than or equal to 160 mmHg or 100 mmHg, respectively.32 The most likely causes of neurological deficits in the context of hypertension are ischaemic or haemorrhagic stroke and, less frequently, hypertensive encephalopathy or posterior reversible encephalopathy syndrome. The latter usually presents in a more sub-acute fashion with varying clinical symptoms, including seizures, encephalopathy, headache and visual disturbance.33
It has been suggested that the direct involvement of neurologists in the emergency department reduces the misdiagnosis rate and is associated with greater use of acute therapies.34 This is not a panacea, however, as Arch et al showed that 35% of missed strokes had neurology involvement.7
The role of neuroimaging
Non-contrast CT brain imaging is the initial imaging modality of choice when stroke is suspected. Early parenchymal ischaemic change, such as reduced grey/white matter differentiation and sulcal effacement, develops within the first few hours of ischaemic insult and can give clues to the diagnosis, as can hyperdensity within the lumen of the vessels – particularly of the middle cerebral artery contralateral to symptoms, or of the basilar artery in posterior circulation stroke syndromes.35 Over the following 24–48 hours, oedema and mass effect can sometimes be seen, particularly in younger patients, while hypodensity and encephalomalacia are hallmarks of established infarction. Table 1 summarises the uses and common pitfalls of CT and more advanced neuroimaging techniques in stroke.35,36
Uses and pitfalls of imaging techniques in acute ischaemic stroke35,36
Conclusions
Ischaemic stroke is a common and treatable medical condition. Stroke recognition tools are designed to fast-track patients through emergency departments but do not replace clinical acumen. Stroke chameleons may present to medical admissions units; a high index of suspicion is required to identify these patients.
Conflicts of interest
The authors have no conflicts of interest to declare.
Acknowledgements
Written consent was obtained from the patient for publication of the clinical details and images in this article.
- © Royal College of Physicians 2017. All rights reserved.








{kind=link}
{kind=link}