
ABSTRACT
Bilateral diaphragmatic paralysis is a known cause of respiratory failure. Diagnosis can be difficult, particularly in the acute setting. We present the case of a gentleman diagnosed with bilateral diaphragmatic paralysis secondary to phrenic neuropathy in the setting of cervical spondylosis.
Case presentation
A 63-year-old man presented to the emergency department with a 2-day history of orthopnea. He reported lifting heavy iron tables 3 days prior to presentation. Bilateral shoulder and neck discomfort were described 1 day prior to the onset of orthopnea. He reported no chest pain, cough, wheeze, sputum, haemoptysis, fevers or ankle oedema. He was a non-smoker whose past medical history included osteoarthritis, hypercholesterolaemia and hypertension.
Cardiovascular and respiratory examinations were normal. Bilateral tenderness of the trapezius muscles was present, increasing with shoulder abduction. No cervical spinal tenderness was evident and neurological examination was normal. Further examination revealed significant positional orthopnea.
Differential diagnosis
Orthopnea is a common manifestation of pulmonary oedema secondary to left ventricular failure and in those suffering from asthma, neuromuscular disease, sleep apnoea or panic disorders. Given this patient's symptoms of neck and back pain, consideration must be given to neuromuscular pathologies.
Initial management
Inflammatory markers, troponin, d-dimer and N-terminal pro b-type natriuretic peptide were normal. Electrocardiogram revealed left ventricular hypertrophy, documented as long standing. Initial chest X-rays demonstrated a small left pleural effusion, making assessment of the left hemidiaphragm difficult. A transthoracic echocardiogram was normal. A computerised tomography pulmonary angiogram (CTPA) was performed because of the patient's ongoing symptoms. This required two attempts because of the patient's orthopnea. CTPA showed bibasal atelectasis with no evidence of pulmonary embolism. Diazepam was required to allow for completion of the CTPA and consideration was given to a panic disorder. However, the patient demonstrated no other features in keeping with this.
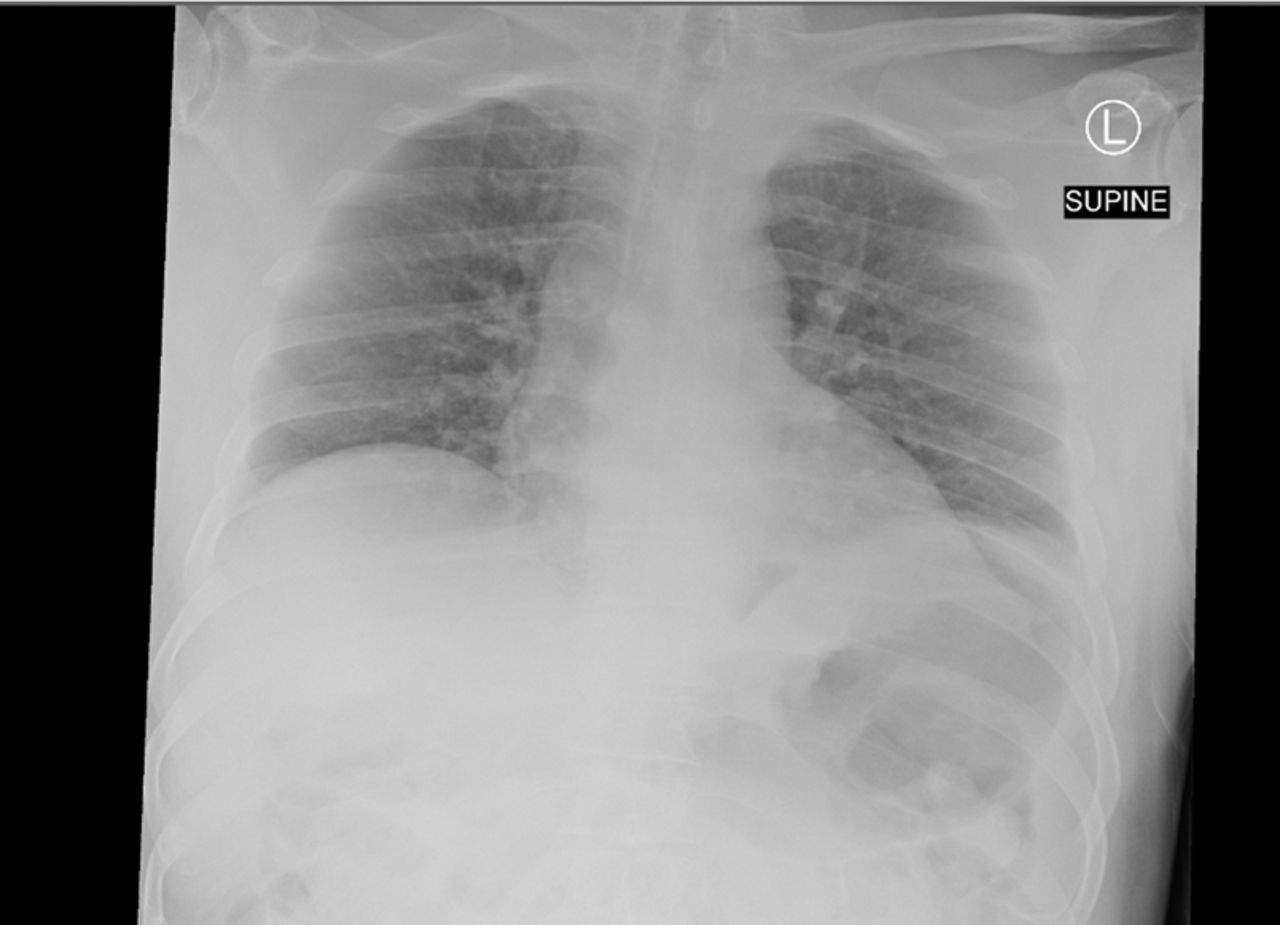
Pulmonary function tests revealed a restrictive pathology with forced expiratory volume at first second (FEV1) of 3.01 L (57% predicted), forced vital capacity (FVC) 3.84 L (60% predicted) and a FEV1/FVC ratio of 78%. Mean inspiratory and expiratory pressures were reduced and a marked decrease in vital capacity was noted with sitting and supine values of 2.13 L and 0.9 L, respectively. Bedside thoracic ultrasonography revealed limited diaphragmatic movement bilaterally. Fluoroscopic sniff test showed reduced maximum inspiratory and expiratory pressures. Chest radiographs completed in both lying (Fig 1) and standing (Fig 2) positions demonstrated elevated bilateral hemidiaphragms while supine.
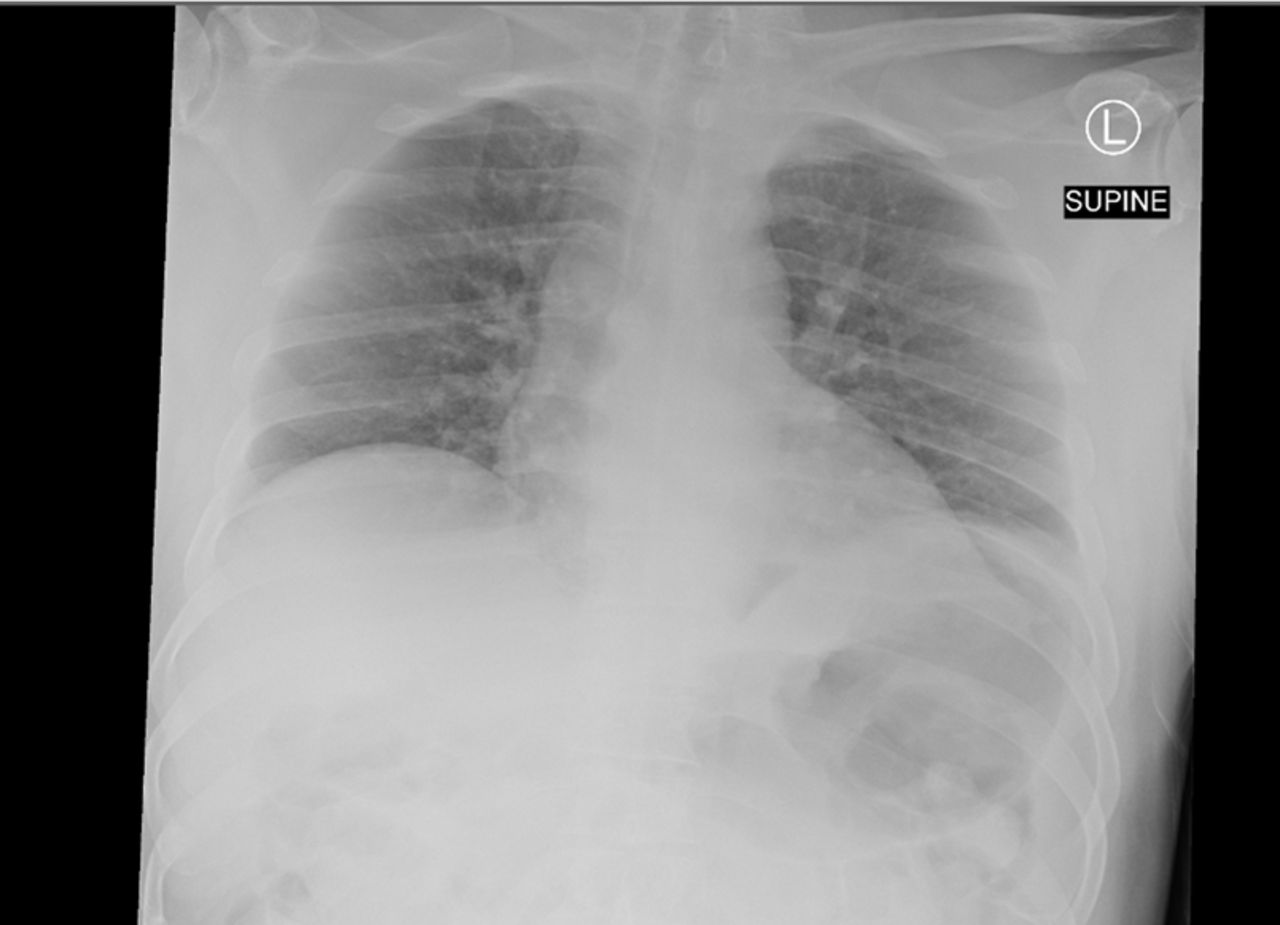
Supine chest radiograph

Erect chest radiograph.
Diagnosis
A presumptive diagnosis of diaphragmatic paralysis was considered and a magnetic resonance image (MRI) of the cervical spine was requested. This demonstrated bilateral neural foraminal narrowing at C3–C5 and posterior discophytic bulging at the level of C4–C6. Spinal cord impingement was noted at C5–C6 with irritation of the nerve roots (Fig 3). Consequently, a formal diagnosis of phrenic nerve neuropathy secondary to cervical spondylosis was made.

Magnetic resonance image of cervical spine.
Discussion
Diaphragmatic paralysis is a known cause of acute respiratory failure, orthopnea and restrictive defects on pulmonary function testing. Diagnosis can be challenging and, consequently, diaphragmatic paralysis may be missed or diagnosed late. In this report, we present the unusual case of a previously well male patient who presented with this disorder after lifting heavy tables. Diagnosis of bilateral diaphragmatic paralysis involves the exclusion of other cardiopulmonary pathologies and the identification of the precipitating neuromuscular pathology.
Diaphragmatic paralysis may be unilateral or bilateral. Unilateral phrenic neuropathies are typically asymptomatic. On the contrary, bilateral diaphragmatic paralysis is associated with profound dyspnoea, particularly in the supine position. This is due to the paralysed diaphragm being unable to contract during inspiration resulting in reduced intrathoracic volumes and decreased inspiratory pressure gradients. Consequently, bilateral pathology is associated with higher levels of morbidity.
Hemidiaphragmatic paralysis and basal atelectasis are typical findings on chest radiograph. Notably, an elevated hemidiaphragm is more sensitive when diagnosing unilateral diaphragmatic paralysis given the tendency for bilateral diaphragmatic paralysis to be misinterpreted as ‘poor inspiratory effort’. Pulmonary function tests are typically normal in those with unilateral phrenic neuropathies while bilateral diaphragmatic involvement is associated with restrictive defects and reduced lung volumes. Decrements of 30–50% in FVC between supine and sitting positions are considered to be sensitive for bilateral diaphragmatic paralysis.1 The absence of such decrements have a high negative predictive value and, therefore, should form part of a patient's routine work-up.
Maximal expiratory and inspiratory pressures reflect respiratory muscle strength and reductions in maximal inspiratory pressure should prompt consideration of bilateral diaphragmatic dysfunction. Fluoroscopic sniff testing can be used to aid diagnosis and is considered positive if paradoxical elevation of the paralysed hemidiaphragm occurs after a vigorous, short-lived inspiration. However, this investigation has high false negative rates in bilateral diaphragmatic pathology and has proven more accurate in the investigation of unilateral phrenic nerve palsies. Ultrasonography may be utilised to evaluate diaphragmatic movement with potential ultrasound findings, including paradoxical displacement of the hemidiaphragm.
Numerous aetiologies are associated with diaphragmatic paralysis, including pneumonia, compressive mediastinal tumours, myelopathies, neuropathies and myopathies. Moreover, iatrogenic damage of the phrenic nerve during central venous cannulation or as a consequence of head and neck surgery has been reported. Unfortunately, the aetiology of diaphragmatic weakness remains unidentified in two thirds of cases.2
Cervical disc pathologies are considered to be rare causes of diaphragmatic weakness. To the authors’ knowledge, there are only eight previously reported cases of phrenic nerve palsy secondary to cervical spondylosis, thus demonstrating the unusual nature of our case. 3–5 Seven cases report phrenic nerve palsy with myelopathy and one in the context of C5 radiculopathy. Our patient had no other discernible cause of diaphragmatic paralysis and the rationale for cervical spondylosis is compelling given the patient's cervical pathology at C3–C5, the origin of the phrenic nerve.
Treatment
Our patient received physiotherapy to strengthen his diaphragmatic muscles. Discussion with neurosurgery favoured a non-surgical management approach as no frank cord compression was evident. Unfortunately, our patient remained symptomatic and had difficulty sleeping. Consequently, consideration is being given to nocturnal bilevel positive airway pressure ventilation (BiPAP). BiPAP has reported benefit in patients with bilateral diaphragmatic paralysis by improving inspiratory muscle capacity and gaseous exchange.6 Additionally, fewer instances of failure are reported when compared with continuous positive airway pressure ventilation.7
In conclusion, neuromuscular pathology should be considered in those patients presenting with acute-onset dyspnea of unclear aetiology, particularly if symptoms are positional. Moreover, cervical spondylosis in association with heavy lifting should be considered as a cause of phrenic nerve injury and diaphragmatic paralysis.
Conflicts of interest
The authors have no conflicts of interest to declare.
Author contributions
All authors were involved in the drafting of the piece and in the acquisition, analysis and interpretation of data for the work. Reflecting workload and contribution to the review of the existing literature, EK is listed as the primary author.
Acknowledgements
Written informed consent was obtained from the patient to publish the clinical details and images in this article.
- © Royal College of Physicians 2017. All rights reserved.








{kind=link}
{kind=link}
{kind=link}