
A 97-year-old woman presented to our emergency department with nausea, vomiting and abdominal pain for about 2 days. She had a history of ultrasound-guided percutaneous cholecystostomy following chronic cholecystitis with a huge gallstone 1 year earlier (Fig 1). Her physical examination showed hypoactive bowel sound and tympanic abdominal percussion. The abdominal radiograph showed no specific findings, except a distended stomach and dilated proximal small bowel loop. A follow-up abdominal computerised tomography (CT) scan demonstrated a gallstone measuring about 4.6 × 3.3 cm in the proximal jejunum, which caused proximal gas distension of the bowel, consistent with gallstone ileus (Fig 1). The patient underwent urgent enterolithotomy and she had an uneventful recovery.
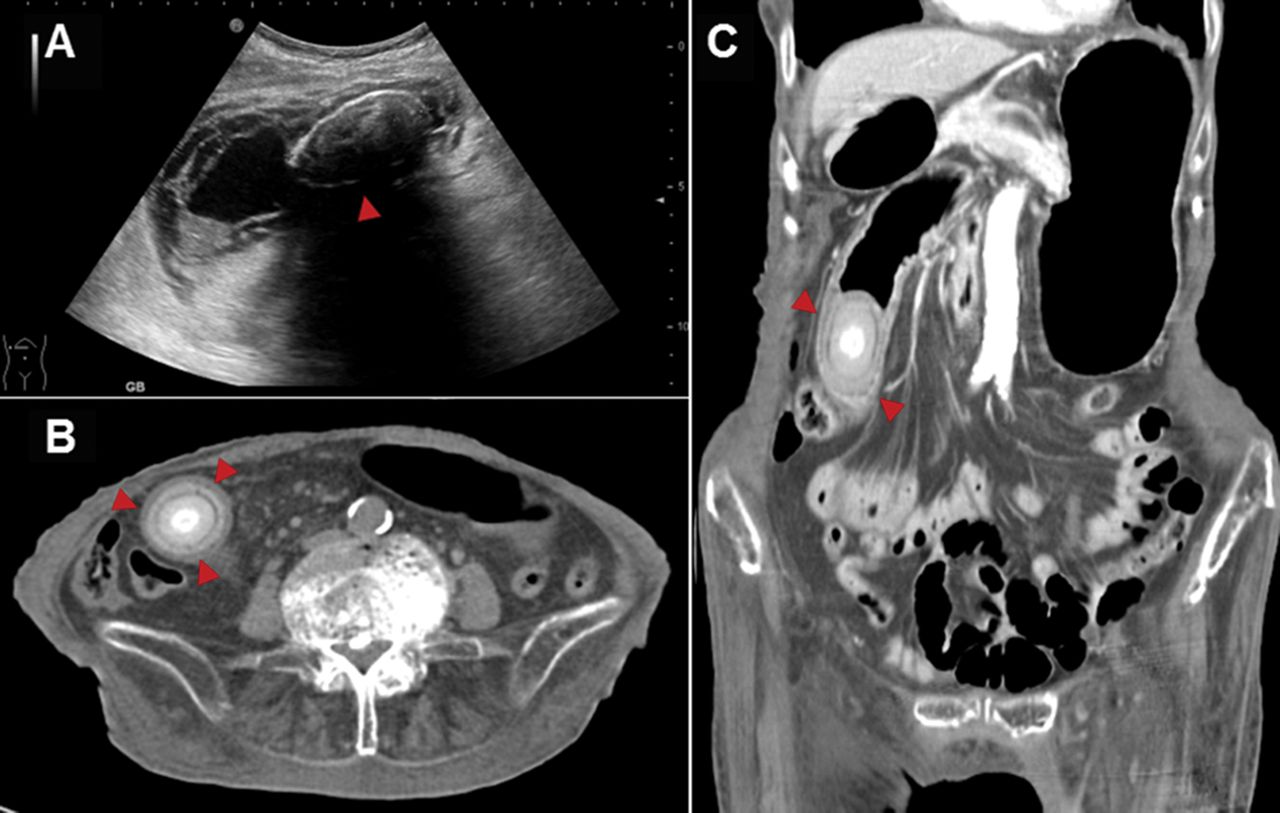
Gallstone image series. A – abdominal ultrasonography showing a huge gallstone within a thick-walled gallbladder (arrowhead); B and C – abdominal computerised tomography scan showing a calcified intra-luminal structure (arrowhead) in the proximal jejunum, which has caused proximal gas distension of the bowel, consistent with gallstone ileus.
Gallstone ileus is a rare bowel obstruction caused by cholelithiasis, which occurs more frequently in older women than men. The main cause of the development of a large gallstone in the intestine is a biliary enteric fistula. More than 70% of cases have cholecystoduodenal fistulas, followed by cholecystocolonic and cholecystogastric fistulas. Most gallstones affect the terminal ileum, which is the narrowest segment of the intestine.1
A preoperative diagnosis of gallstone ileus is challenging. Its nonspecific clinical presentation tends to delay diagnosis and treatment. The Rigler triad is the classic radiologic sign of gallstone ileus and consists of pneumobilia, intestinal obstruction and an ectopic gallstone. However, most gallstones are radiolucent and all three elements of the Rigler triad are present on plain radiographs in only 15% of cases. The Rigler triad is seen in up to 80% of cases when CT is used.2 Ultrasound is purported to have greater than 95% specificity and sensitivity in detecting gallstones within the gallbladder, but it is of limited use in cases of gallstone ileus because of gaseous distension of the bowel.3
Surgical intervention is the mainstay treatment strategy of gallstone ileus. The two-stage procedure (enterolithotomy followed by cholecystectomy and repair of the biliodigestive fistula after 4–6 weeks) is an alternative treatment suggested for patients with recurrent biliary symptoms.4 Nevertheless, a nonsurgical strategy, such as extracorporeal or electrohydraulic lithotripsy and the endoscopic removal of gallstones, has been reported.5n
Conflict of interest
The authors have no conflicts of interest to declare.
Acknowledgements
Written consent was obtained from the patient to publish the clinical details and images in this article.
- © Royal College of Physicians 2017. All rights reserved.








{kind=link}
Related Articles
Cited By...
- No citing articles found.