
ABSTRACT
Physicians responsible for the care of patients with heart failure due to left ventricular systolic dysfunction have access to a broad range of evidence-based treatments that prolong life and reduce symptoms. In spite of the significant progress made over the last four decades, there is an ongoing need for novel therapies to treat a condition that is associated with stubbornly high morbidity and mortality. In this article, we discuss the findings of SERVE-HF, a randomised controlled trial of adaptive servo-ventilation in patients with left ventricular systolic dysfunction, as well as EMPA-REG, a study of the effects of a novel diabetic agent that may be of greater interest to heart failure specialists than diabetologists. We also examine further analyses of the groundbreaking PARADIGM-HF trial, which attempt to answer some of the unresolved questions from the original study of the first combined angiotensin-receptor blocker and neprilysin inhibitor, sacubitril valsartan. The recently published National Institute for Health and Care Excellence guidelines for the management of acute heart failure and plans to introduce best practice tariffs bring into focus the need for well-organised, multidisciplinary care. We discuss the challenges involved in developing and delivering a specialist service that meets the needs of a growing population of patients living with heart failure.
Introduction
Prodigious advances in the treatment of heart failure due to left ventricular (LV) systolic dysfunction have led to one of the major medical success stories of the last 40 years. Medications targeting neurohormonal activation are the cornerstone of treatment, and they are complemented by device therapy and heart rate reduction, among other measures, in selected patients.1–4 The net effect has been an effective doubling of life expectancy, with significant improvements in quality of life, for a condition that once had a very bleak prognosis.5 These successes have been possible through major investment in drug and device development, the conduct of well-designed large scale randomised clinical trials and the development of specialist heart failure teams to initiate and up-titrate therapies in appropriate patients.
In spite of these impressive achievements, the mortality from heart failure remains stubbornly high and a significant proportion of the healthcare budget is spent on unplanned hospital admissions due to decompensated heart failure.6 It is important, therefore, that novel therapeutic targets are identified. We have selected three large scale clinical trials for review that are likely to have a significant and far reaching impact on the management of patients with heart failure. These include the largest trial to date of non-invasive ventilation in chronic heart failure, as well as the first phase III trial of a novel diabetic agent that is associated with improved cardiovascular outcomes, particularly with respect to heart failure. We also summarise a number of re-analyses of the data from the groundbreaking PARADIGM HF trial, which identified a first-in-class treatment for chronic heart failure that is superior to angiotensin-converting enzyme (ACE) inhibitors. We conclude the review with a summary of recent changes to the organisation of heart failure care in the UK.
SERVE-HF
Central sleep apnoea (CSA) is a common finding in patients with heart failure due to LV systolic dysfunction, and it is typically associated with more advanced disease.7 Patients with CSA exhibit increased sympathetic drive during both apnoeic episodes and waking hours and it is an independent risk factor for ventricular arrhythmias and mortality.8 Adaptive servo-ventilation (ASV) provides positive end-expiratory support and variable inspiratory support, which together effectively reduce the frequency of apnoeic/hypopneic (AH) episodes.9 ASV was therefore an attractive potential therapeutic intervention.
SERVE-HF was a multicentre, international, randomised clinical trial that recruited adults with symptomatic chronic heart failure with an LV ejection fraction of less than 45%.10 Central sleep apnoea was defined using polysomnography as more than 15 AH episodes per hour with more than half of them being central events and more than 10 central AH episodes per hour. Patients were asked to use the ASV device for at least 5 hours per night with the aim of reducing the frequency of AH episodes to fewer than 10 per hour.
In total, 1,325 patients were randomised and followed up for a median of 31 months. Adaptive servo-ventilation reduced the frequency of AH episodes, although only 60% in the treatment arm used the device for 3 or more hours per night. There was no difference in the rate of the composite primary endpoint of death from any cause, a life-saving cardiovascular intervention, or hospitalisation for worsening heart failure between the intervention and control arms (54.1% versus 50.8%, p=0.10, Fig 1). However, there was an increase in both all-cause (34.8% versus 29.3% p=0.01) and cardiovascular mortality (29.9 versus 24% p=0.006) in the adaptive servo-ventilation arm compared with control. There was no difference between groups when comparing a number of quality of life measures and there was a greater reduction in 6-minute walk distance over the follow-up period in the intervention arm.
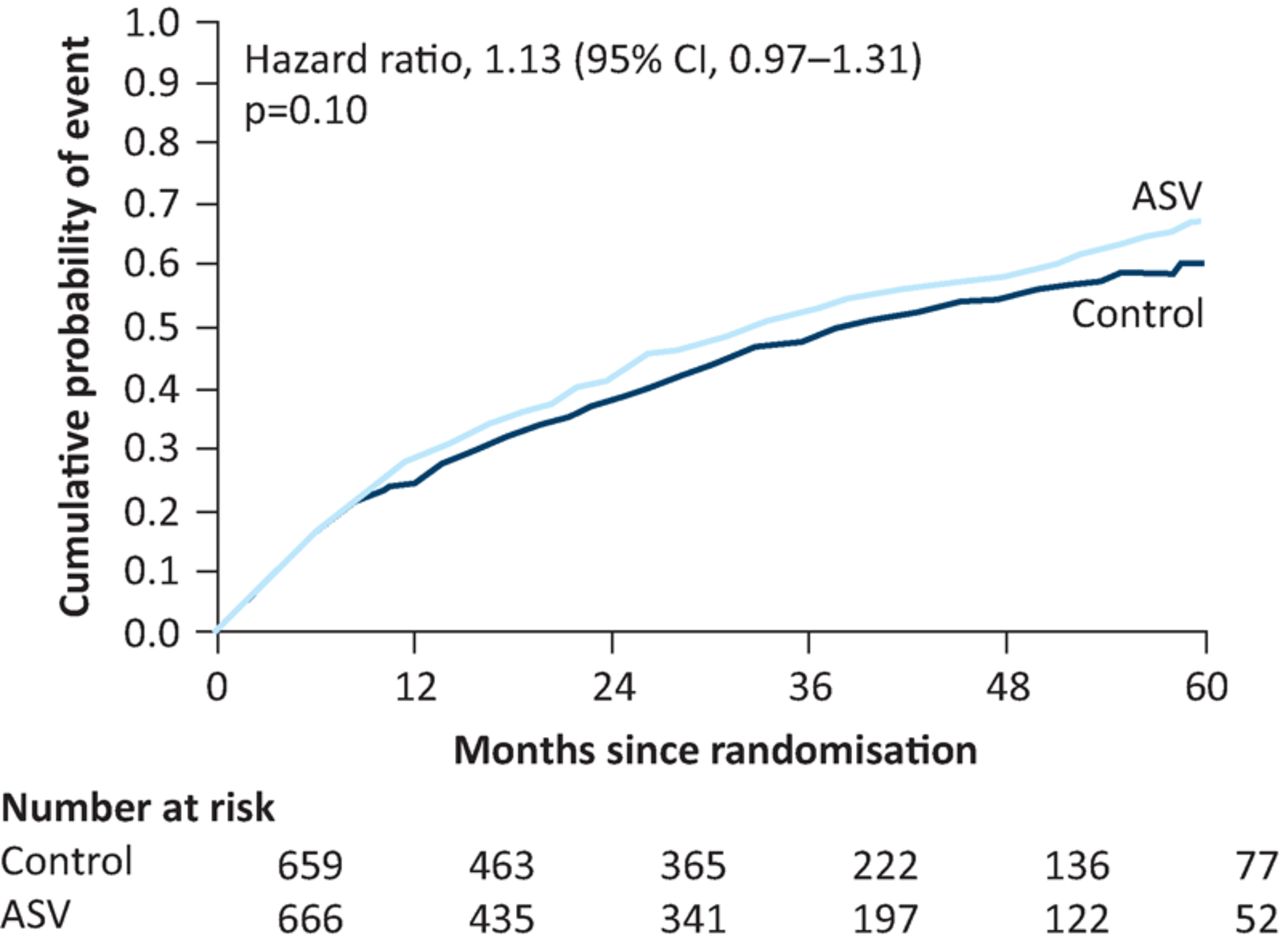
Primary outcome of SERVE-HF trial. The probability of an event (death from any cause, need for life-saving cardiac intervention, hospitalisation due to heart failure) according to treatment with adaptive servo-ventilation (ASV) versus control. Reproduced with permission from Cowie et al.10
The results were a surprise to many. Proposed explanations included concern about the specific pressure algorithms used, hypovolaemia related to excessive mouth breathing, potential adverse effects of ASV in pulmonary hypertension and the risk of hypocapnia induced arrhythmias. These hypotheses were not supported in exploratory analyses.11 One possibility is that CSA might have protective effects in patients with heart failure, which were blunted by the use of ASV. Another possibility is that periodic respiration is often seen during the day in patients with severe heart failure and it might be that treating it at night led to rebound worsening during the day when periodic respiration was not treated. Further work is clearly required to elucidate the true pathophysiological mechanisms.
A number of smaller studies that assessed the use of adaptive servo-ventilation in central sleep apnoea demonstrated improvements in surrogate outcome markers such as B-type natriuretic peptide (BNP) and ejection fraction.13 The study serves to highlight the importance of high-quality, large scale trials that assess ‘hard’ clinical endpoints, particularly for medical devices, which seem to be subject to less stringent regulatory approval processes than pharmacological therapies.
EMPA-REG
It may seem strange to include a trial in patients with diabetes in an article on heart failure, but bear with us. EMPA-REG OUTCOME examined the effect of empagliflozin, a novel diabetic agent, on cardiovascular outcomes.14 The results of the study were published 2 days after Thanksgiving in the USA and diabetologists were undoubtedly grateful for the news that a glucose-lowering agent has a beneficial effect on macrovascular complications.
The ACCORD study demonstrated that intensive glycaemic control is associated with an increased risk of death in diabetics with established cardiovascular disease.15 Furthermore, the widely publicised association between rosiglitazone use and increased risk of heart failure mean that it is imperative that all potential new agents for reducing blood sugar are subject to exhaustive evaluation prior to regulatory approval, particularly with respect to cardiovascular outcomes.16
Empagliflozin is an inhibitor of the sodium-glucose linked transporter 2, found in the proximal tubules of the nephron. It leads to reduced glucose reabsorption from the urinary space, and consequently increases glucose excretion.17
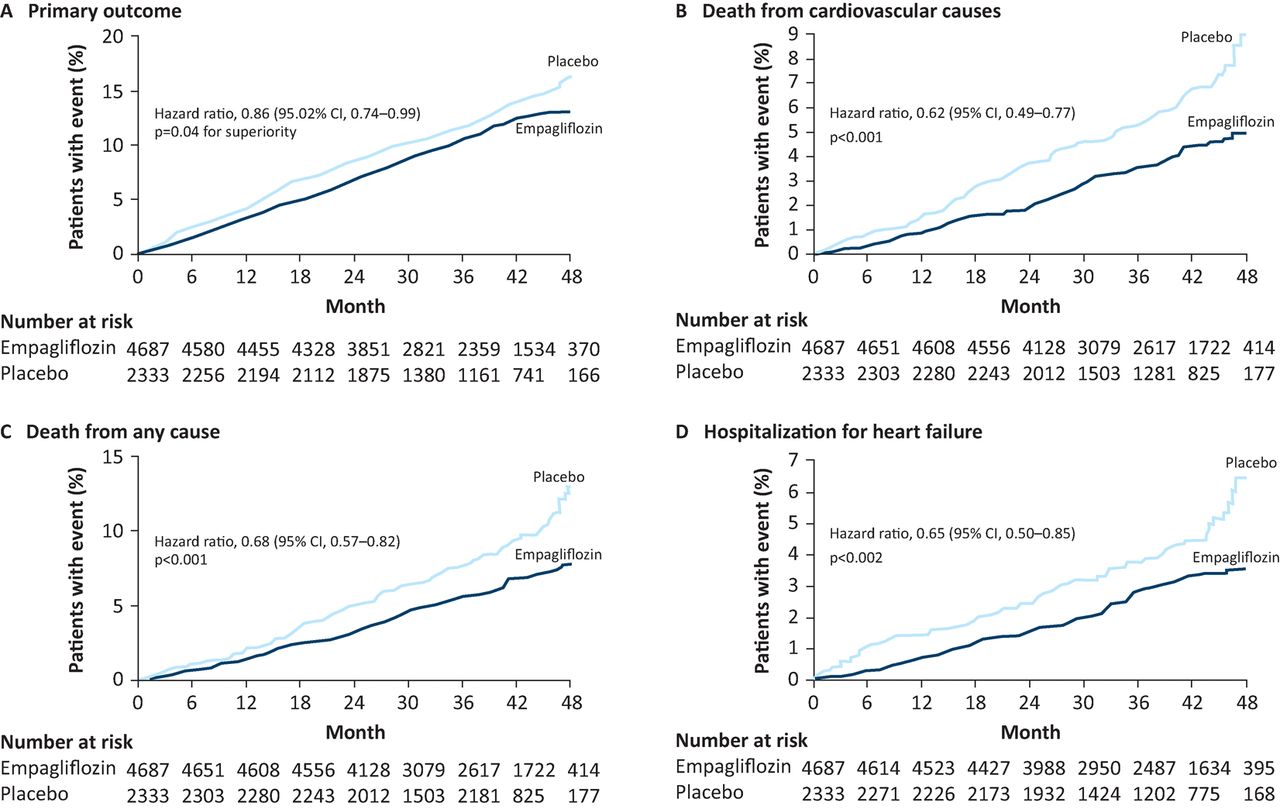
EMPA-REG OUTCOME was a multicentre, blinded, randomised, placebo-controlled trial in patients with type 2 diabetes mellitus (T2DM) and established cardiovascular disease. In total, 7,028 patients were randomised to either 10 mg or 25 mg empagliflozin once daily or placebo for a median of 2.6 years. Although the study was designed as a non-inferiority trial, empagliflozin use was associated with a 14% relative risk reduction in the composite primary outcome of cardiovascular death, non-fatal myocardial infarction and non-fatal stroke compared with placebo (10.5% versus 12.1%, p=0.04 for superiority, Fig 2). A reduction in cardiovascular death was the key component driving the composite outcome finding. There was no significant difference in cardiovascular event rates between the two empagliflozin dose arms. Genital infections were more common in the treatment arms but rates of serious complications were low. Rates of discontinuation were similar in all arms.

Outcome data from the EMPA-REG trial, demonstrating the superiority of emagliflozin compared with placebo for the primary composite outcome, and each of the individual components. Reproduced with permission from Zinman et al.14
So why include EMPA-REG OUTCOME in a heart failure article? One of the oddest things about diabetes from the perspective of a specialist in heart failure is how poor the evidence base for treating blood sugar is. The most sanguine interpretation of prior studies examining the effect of glycaemic control on cardiovascular outcomes would conclude that, at best, a relatively modest benefit is seen only after many years of treatment.18 The EMPA-REG study showed a divergence in the Kaplan-Meier curves within the first 4 months, and the study authors themselves acknowledged that the improved glycaemic control seen in the patients taking empagliflozin was unlikely to account for the impressive, early clinical benefits.
Empagliflozin is an osmotic diuretic, so it is perhaps not surprising that there was a 35% relative risk reduction in the rate of hospitalisation for heart failure, a pre-specified secondary endpoint. The patients in EMPA-REG OUTCOME had an early and sustained fall in both weight and blood pressure and an increase in haematocrit, consistent with an osmotic diuresis with a net fluid loss of about 1.5 L.19 The mean systolic and diastolic blood pressure reductions were 5 mmHg and 2.5 mmHg, respectively. Small reductions in blood pressure may substantially improve prognosis in patients with and without T2DM,20 and it may be that diuretics reduce central blood pressure more than peripherally, leading to even more favourable reductions in preload and afterload.21
It is important that these impressive trial results are not interpreted as evidence that HbA1c is an important therapeutic target. Perhaps empagliflozin will be an even better treatment for heart failure than for T2DM.
PARADIGM HF
The PARADIGM HF trial announced the emergence of a new drug class for the treatment of systolic heart failure in impressive fashion.22 The study findings, published in 2014, were viewed as one of the most important breakthroughs in heart failure management for over two decades. Subsequent re-analyses of the trial data have attempted to answer a number of outstanding questions.
Original study
The new agent under investigation was a combination of sacubitril (a neprilysin inhibitor) and valsartan (an angiotensin receptor blocker (ARB)), prosaically designated LCZ696. Neprilysin is a neutral endopeptidase chiefly produced in the kidneys, which degrades vasoactive peptides such as A- and B-type naturetic peptides (ANP, BNP), substance P and adrenomedullin. Inhibiting the breakdown of naturetic peptides leads to vasodilation, naturesis and diuresis. However, blocking neprilysin alone also blocks the breakdown of angiotensin II, and so combining sacubitril with valsartan is vital to get the full effect of potentiation of natriuretic peptides.
The trial investigators bravely compared this new agent to enalapril, the grande dame of heart failure treatment. They enrolled adults with an LV ejection fraction of less than 35%, New York Heart Association (NYHA) class 2–4 symptoms, an elevated BNP and/or recent hospitalisation, and established on stable heart failure therapy, which included either an ACE inhibitor or ARB. During a 6–8 week run-in period, patients were switched to enalapril 10 mg twice daily for 2 weeks, then sacubitril valsartan for a further 4–6 weeks (with dose uptitration to 200 mg twice daily). Only if both agents were tolerated were patients randomised to either enalapril or sacubitril valsartan.
The trial randomised 8,442 patients to one of the two treatment arms; 997 patients withdrew during the run-in period. The trial was stopped early because of evidence of an overwhelming benefit in the sacubitril valsartan arm in respect of the primary outcome, a composite of cardiovascular death and hospitalisation for heart failure (Fig 3). There was a 20% reduction in the rate of cardiovascular death and 21% reduction in the rate of heart failure hospitalisation in patients receiving sacubitril valsartan compared with enalapril. The number needed to treat to prevent one of the primary outcomes was 21. Although the rate of symptomatic hypotension was higher with sacubitril valsartan, the discontinuation rate due to adverse events was higher in the enalapril arm.
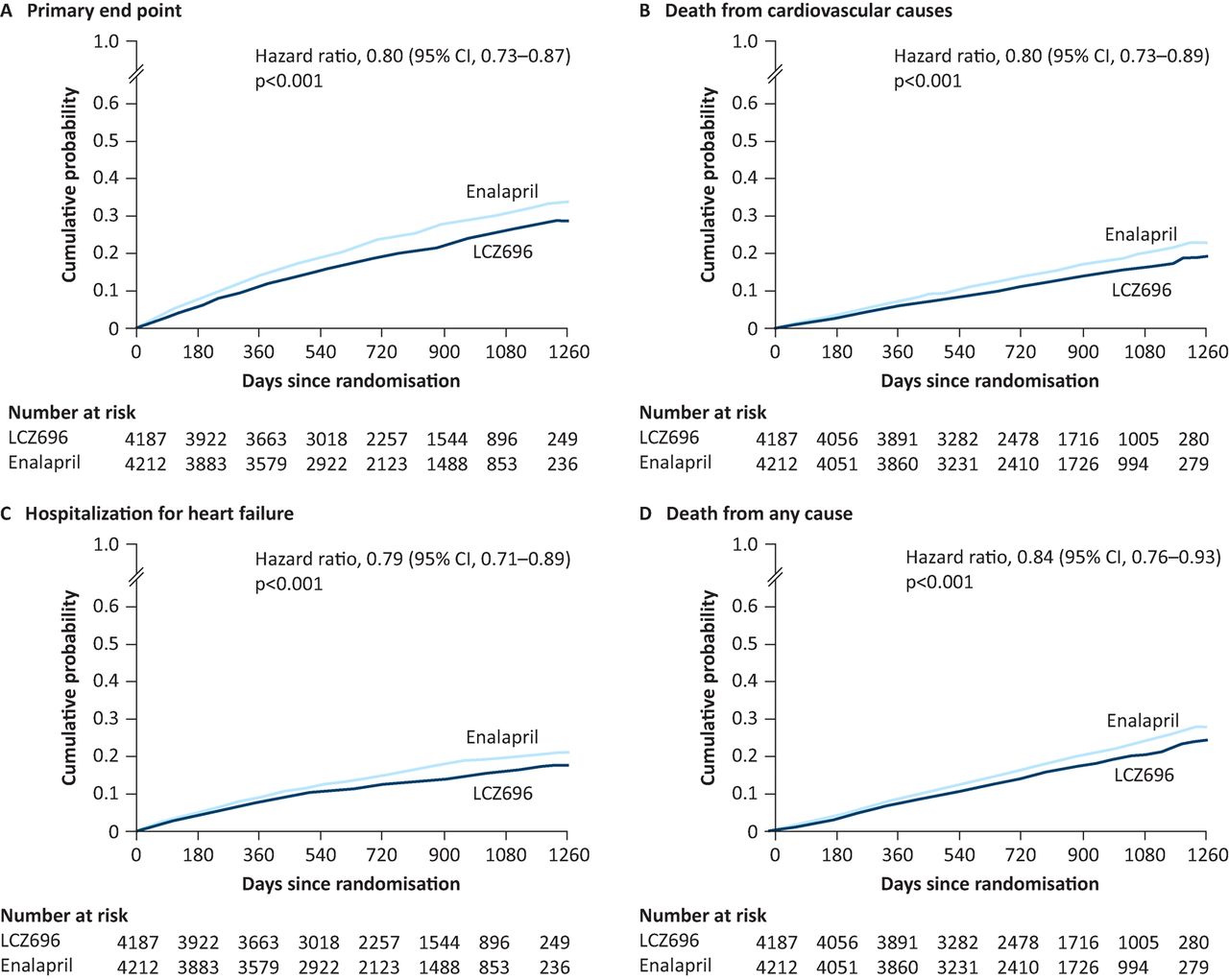
Outcome data from the original PARADIGM-HF trial, demonstrating the superiority of sacubitril-valsartan compared with enalapril for the primary composite outcome, and each of the individual components. Reproduced with permission from McMurray et al.22
The superiority of sacubitril valsartan over enalapril in patients with chronic systolic heart failure was conclusively demonstrated. Furthermore, the dose of enalapril used in this study was higher than that used in the CONSENSUS and SOLVD trials that established its efficacy.2,23
Effect of age on treatment efficacy and safety
There is some persisting concern regarding the efficacy and tolerability of sacubitril valsartan in older patients. The mean age of patients enrolled into PARADIGM HF was 63.8 years, whereas the mean age of patients included in the latest UK National Heart Failure Audit was 76 years for men and 78 years for women.24 The discrepancy is partly explained by the lower age at presentation of patients who live in South America and Asia, but exclusion due to comorbidities, cognitive impairment and physician referral bias are also factors that often limit enrolment of older patients.25
Jhund et al26 examined the efficacy of sacubitril valsartan according to age. Patients were categorised into four age groups; 1,563 (18.6%) of all patients randomised were age 75 years or older.26 This group had more comorbidities, higher BNP levels and were more likely to be in a higher NYHA class, but the magnitude of treatment effect with sacubitril valsartan was consistent across the age ranges for each of the primary outcome measures. Furthermore, the effect that sacubitril valsartan demonstrated on slowing the rate of symptom progression was similar in all age groups. This may be of particular importance to older patients for whom quality of life is often the greater concern. The rates of symptomatic hypotension were higher in older patients, but very few were forced to discontinue treatment as a result.
A very small proportion of randomised patients were aged over 80 years, which limits the generalisability of these findings to the very elderly that make up a substantial part of many cardiologists’ clinical workload. PARADIGM-HF enrolled patients from a broader age range than any previous trial; it therefore represents a step forward in the move towards more inclusive and representative trial design and recruitment.
The effect of treatment according to baseline risk
Recognising that clinical outcomes often correlate poorly with individual factors such as NYHA class and LV ejection fraction, Simpson et al27 sought to examine whether more comprehensive risk scoring systems could identify patients that are most likely to benefit from treatment with sacubitril valsartan over conventional therapy. The Meta-analysis Global Group in Chronic Heart Failure (MAGGIC) risk score at baseline was calculated for all patients with sufficient data,28 and the EMPHASIS-HF (Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure) score was calculated for those with milder symptoms (NYHA 1 and 2).29
There was very good correlation between risk score and risk of an adverse event in the PARADIGM-HF cohort. The magnitude of treatment benefit with sacubitril valsartan was similar across all risk scores with respect to the primary composite endpoint. The absolute risk reduction for rates of HF hospitalisation was greater in those at highest risk, although there was a consistent treatment benefit seen across the spectrum. The study nicely illustrates the large variability in risk among patients with relatively mild symptoms. Although the scoring tools might help pick out which patients require more frequent follow-up, neither incorporates natriuretic peptide level measurements, which are the single most powerful predictors of outcome.
Effect of sacubitril valsartan on risk of clinical progression
The journey of a patient diagnosed with heart failure is typically characterised by a progressive decline in functional capacity, punctuated by acute episodes of decompensation that frequently lead to hospitalisation. Packer et al30 assessed the effect of sacubitril valsartan on a broad range of indicators of clinical deterioration. Sacubitril valsartan reduced the risk of worsening heart failure that required outpatient intensification of therapy, reduced the chance of an increase in NYHA class, led to fewer visits to the emergency department, hospitalisations because of heart failure or for any reason and admissions to intensive care, and reduced the need for inotropic support. These benefits will be of great interest to those responsible for funding care at both primary and secondary care level, particularly in the current era of NHS funding cuts and seemingly insurmountable pressures on acute hospital services.
The National Institute for Health and Care Excellence (NICE) has recommended sacubitril valsartan, marketed as Entresto (Novartis), as a treatment option instead of an ACE inhibitor or ARB for patients with NYHA class 2–4 symptoms and an LV ejection fraction of 35% or less, who are already taking a stable dose of ACE inhibitors or an ARB.31
Organisation of care
The prevalence of heart failure in the UK is rising, principally as a result of an aging population, lower mortality following acute myocardial infarction and improved use of evidence-based heart failure therapies.32 It is imperative that robust systems are in place to ensure access to specialist care. The multidisciplinary team should include cardiologists, specialist nurses, GPs and elderly care physicians with an interest in heart failure and close links to palliative care services, cardiac rehabilitation and advanced heart failure units.
The National Heart Failure Audit has consistently demonstrated that patients who receive specialist inpatient care during hospitalisation with acute heart failure have lower mortality and readmission rates, even after adjustment for baseline factors.23 These findings have undoubtedly influenced the recently published NICE acute heart failure guidelines, which recommend that all patients admitted with suspected heart failure should have early and continuing access to specialist services.33 The recommendations that all patients with heart failure are seen by the heart failure specialist team within 24 hours of admission to hospital, and within 2 weeks of discharge following admission, will be extremely challenging for many trusts. It’s likely that the initiation and up-titration of sacubitril valsartan will be performed in secondary care, placing even greater strains on the current services.
The National Heart Failure Audit data and NICE recommendations provide valuable material with which to build business cases for additional resources, personnel and training. This can often feel like a Sisyphean task, but it may well be that the likely introduction of a best practice tariff for heart failure (which will include as measures both access to specialist care and entry of patients into the national audit) will focus managerial minds. It is vital that heart failure specialists persevere in their drive to develop a high-quality, sustainable service that provides equitable access to state-of-the-art heart failure care.
Conflicts of interest
ALC has received payments from Novartis for attendance at advisory boards and to support his department. PDC has no conflicts of interest.
Note
This article was originally published in the 2016 Clinical Medicine supplement Horizons in Medicine 28. All articles in this supplement are available at www.clinmed.rcpjournal.org/content//16/Suppl_6
- © Royal College of Physicians 2017. All rights reserved.








{kind=link}
{kind=link}
{kind=link}