
ABSTRACT
We describe a case of a young lady with anti-NMDA (N-methyl-D-aspartate) receptor encephalitis, who initially presented with status epilepticus. Her seizures and orofacial dyskinesia were refractory to four anticonvulsants. She received intravenous immunoglobulin and a left ovarian tumour (an associated feature) was resected. However, her outcome was poor because of delayed treatment, autonomic dysfunction and complications of prolonged hospitalisation. This case highlights the importance of an early recognition of this rare but increasingly recognised disease.
Case presentation
A 21-year-old woman with no past medical history presented to the emergency department with a 5-day history of bitemporal headaches and fever and altered behaviour (she had been talking to herself and forgetful) for the past 3 days. Otherwise, there were no symptoms suggestive of urinary tract infection, upper respiratory tract infection and gastroenteritis. She denied a history of head trauma, febrile seizures or family history of epilepsy. Her physical examination was unremarkable. Her presenting vitals were as follows: blood pressure 120/78 mmHg, heart rate 72 bpm, temperature 37°C and SpO2 98% on room air. However, she developed convulsive status epilepticus the day after admission and was subsequently intubated.
Initial blood results revealed leucocytosis (white cell count 18.9×109), mild hypokalaemia (3.3 mmol/L) and an erythrocyte sedimentation rate of 80 mm/hour. Other investigations, including random blood glucose, haemoglobin, platelet, electrolytes, liver function test and coagulation profile, were normal. She tested negative for pregnancy, syphilis, hepatitis, HIV and drug toxicology. Her electrocardiogram was normal. We proceeded with a lumbar puncture, which had an opening pressure at 27 cmH2O. Her cerebrospinal fluid analysis showed normal cell counts, biochemistry and negative culture results. Her brain computerised tomography (CT) showed no abnormalities. High signal intensity and cortical thickening were detected along the medial aspects of the bilateral temporal lobes on her brain magnetic resonance imaging (MRI) scan (on the day of status epilepticus) (Fig 1). Both her magnetic resonance angiogram and venogram were normal.
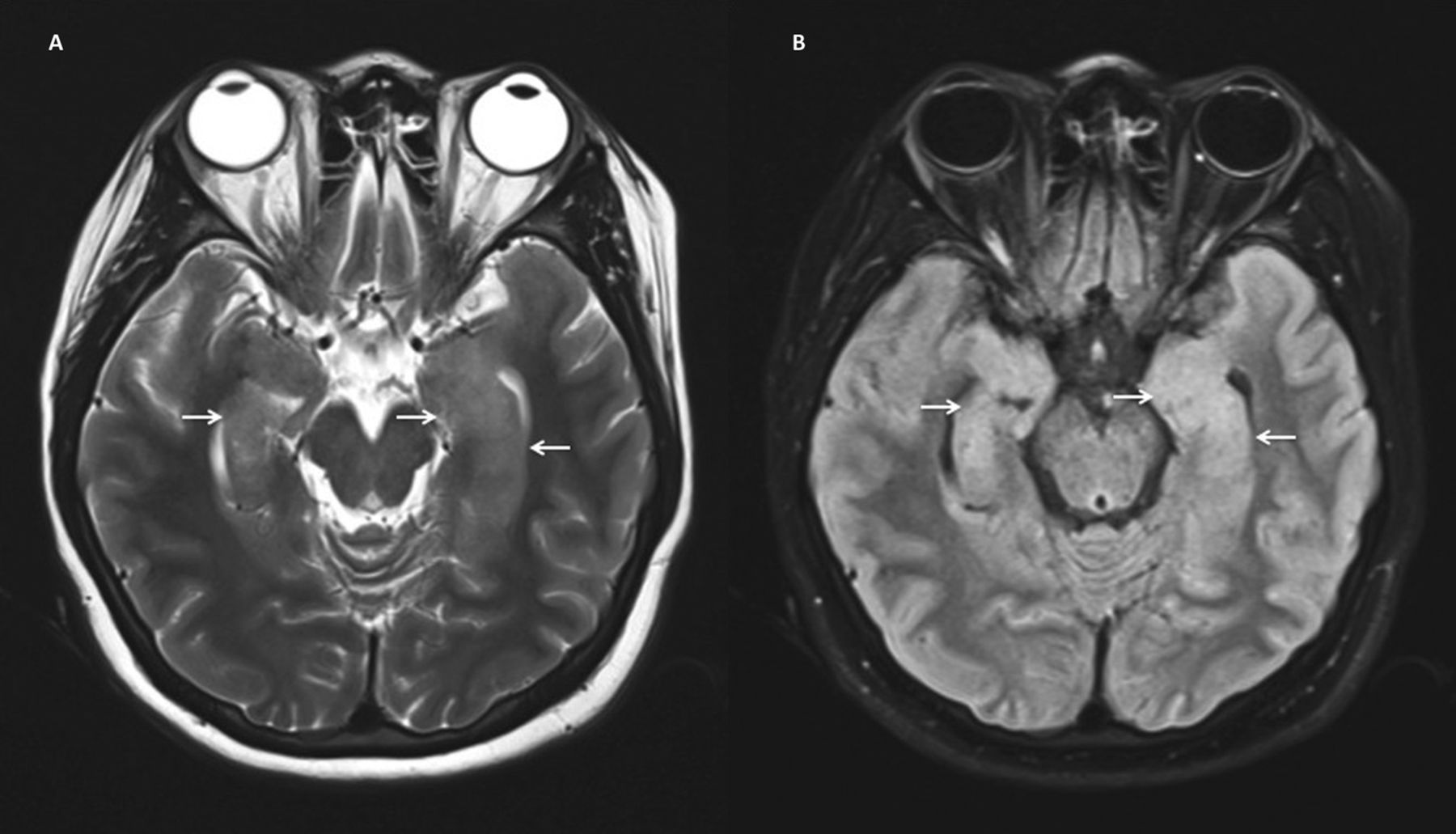
Imaging investigations. A – T2-weighted axial magnetic resonance images demonstrating high signal intensity and cortical thickening along the medial aspect of bilateral temporal lobes; B – fluid-attenuated inversion recovery axial magnetic resonance images demonstrating high signal intensity and cortical thickening along the medial aspect of bilateral temporal lobes.
Diagnosis
At this juncture, a diagnosis of meningoencephalitis was considered because of her clinical manifestations, leucocytosis and the elevated opening pressure of the lumbar puncture. After consultation with the neurologist (from another referral centre), it was agreed that the brain MRI findings were suggestive of an infection. Tuberculous meningitis was unlikely because of her short presenting history and absence of typical brain MRI findings. Central nervous system vasculitis, either primary or secondary to systemic vasculitis such as systemic lupus erythematosus, was considered in the differential diagnosis pending the workup.
Initial management and prognosis
She was treated with intravenous (IV) acyclovir 500 mg q8h and ceftriaxone 2 g q12h in the intensive care unit (ICU). She remained haemodynamically stable and afebrile. Staged approach protocol for status epilepticus was somehow not conformed to in a timely manner. She was initially loaded with IV phenytoin 15 mg/kg followed by IV phenytoin 100 mg three times per day and maintained at an anaesthetic dose of midazolam. IV sodium valproate at 20 mg/kg was added the next day as seizures were still observed. Sodium valproate was escalated to 30 mg/kg the subsequent day. She was administered oral levetiracetam 1 g twice per day (as IV was not available at our centre) as the third anticonvulsant after a few days of ICU admission. Brain CT was repeated in view of persistent seizures; however, there were no new findings.
Case progression and outcome
Her connective tissue disease workup was negative. The electroencephalogram revealed diffuse slow delta waves in both hemispheres, which suggested diffuse cortical dysfunction. She was later put on thiopental infusion at 3 mg/kg/hour for her persistent seizures and orofacial dyskinesia. After showing the video of orofacial dyskinesia to the neurologist and having a lengthy discussion, autoimmune encephalitis was suspected. Anti-NMDA, Hu, Yo, Ri, Ma, CV2, Amphiphysin, LGI1 antibodies (available in Malaysia) were sent. Her serum was positive for anti-NMDA receptor antibodies. She received a cycle of intravenous immunoglobulin (0.4 g/kg/day) for 5 days. As part of the work-up, a CT scan of the thorax, abdomen and pelvis was carried out to look for underlying malignancy. A left ovarian tumour was found and subsequently resected. Tracheostomy was performed for prolonged ventilation because the patient had developed ventilator-associated pneumonia (VAP). Following this, she had no more seizure attacks. However, she developed hypoxic ischaemic encephalopathy after a few episodes of cardiac arrest as a result of the ongoing autonomic dysfunction and sepsis due to VAP. After several sessions of family conferences, her family members were not keen on the second-line therapy for fear of the potential side effects, such as infections. She had poor neurologic recovery with modified Rankin scale 5/6 upon discharge.
Discussion
Anti-NMDA receptor encephalitis was first described by Dalmau et al in 2007.1 It is a form of autoimmune encephalitis targeted against the NR1 subunit of the NMDA receptor (N-methyl D-aspartate receptor).2 It is the cause of 4% of encephalitis cases.3 According to the largest cohort study, the median age of diagnosis is 21 years. Anti-NMDA receptor encephalitis is more common in females (accounting for 81% of cases).4 It is a condition associated with tumours, mostly teratomas of the ovaries. However, there are substantial cases with no detectable malignancy.
Many patients report prodromal symptoms such as headaches, fever or flu-like illness from days to weeks prior to disease onset. Signs and symptoms include psychosis, reduced consciousness, seizures, memory deficits, dyskinesias, and autonomic and language dysfunction. Diagnosis is confirmed by the detection of antibodies to the NR1 subunit of the NMDA receptor in serum or cerebrospinal fluid. Treatment includes first-line immunotherapy (steroids, immunoglobulin, plasmapheresis), second-line therapy (rituximab, cyclophosphamide) and tumour removal. Remission within 4 weeks is achieved by 53% of the patients following first-line therapy or tumour removal according an observational cohort study.4
Status epilepticus is a condition resulting either from the failure of the mechanisms responsible for seizure termination or from the initiation of mechanisms that lead to abnormally prolonged seizures. It is a condition that can have long-term consequences, including neuronal death, neuronal injury and alteration of neuronal networks, depending on the type and duration of seizures. Twenty percent of status epilepticus patients are refractory. According to a cohort study done by Spatola et al to analyse the aetiology and outcome of status epilepticus, 2.5% of cases (n=570) were autoimmune. Of these, only two cases were a result of anti-NMDA receptor encephalitis.5 Wingfield et al reported six cases of refractory status epilepticus in an analysis of 100 cases of anti-NMDA receptor encephalitis.3
Our patient had anti-NMDA receptor encephalitis as evident by her typical symptoms (prodromal headaches, fever, altered mental state, memory deficits and seizures) and clinical signs (orofacial dyskinesia); this was further confirmed by positive antibodies in her serum. Even though refractory status epilepticus due to anti-NMDA receptor encephalitis is not common, clinicians should have a high index of suspicion. In our case, failure to administer timely aggressive treatment (escalation of anticonvulsants) led to refractory status epilepticus. Diagnosis was delayed because of poor recognition of the disease, which resulted in the patient’s prolonged ICU stay and poor neurological status.
Key learning points
In patients with no previous history of epilepsy, the following causes of status epilepticus must be considered: cerebral causes (such as injury, tumour or infection), drug withdrawal or overdose, hypoglycaemia, alcohol withdrawal, vitamin B12 deficiency, metabolic abnormalities and sepsis.
Escalation of anticonvulsants was inadequate and not timely in this case; this is a common cause of refractory status epilepticus.
Autoimmune encephalitis, although rare, is an increasingly recognised cause of status epilepticus.
A high index of suspicion of autoimmune encephalitis should be given in cases of refractory status epilepticus.
Clinicians should look for underlying paraneoplastic aetiology when diagnosis of autoimmune encephalitis is ascertained.
Conflicts of interest
The authors have no conflicts of interest to declare.
Author contributions
All authors contributed to writing and editing the article.
Acknowledgements
Written consent was obtained to publish the clinical details and images in this article.
- © Royal College of Physicians 2017. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.