
Abstract
Virtually all medical specialties are impacted by genetic disease. Enhanced understanding of the role of genetics in human disease, coupled with rapid advancement in sequencing technology, is transforming the speed of diagnosis for patients and providing increasing opportunities to tailor management. As set out in the Annual report of the Chief Medical Officer 2016: Generation Genome1 and the recent NHS England board paper Creating a genomic medicine service to lay the foundations to deliver personalised interventions and treatments,2 the increasing ‘mainstreaming’ of genetic testing into routine practice and plans to embed whole genome sequencing in the NHS mean that the profile and importance of genomics is on the rise for many clinicians. This article provides a brief overview of genomics and its current clinical applications, including its contribution to personalised medicine. Physicians will be signposted to key issues that will allow the successful implementation of genomics for rare disease diagnosis and cancer management.
Key points
Genomic approaches offer the capacity to understand the breadth of rare disease and cancer, including those that are exclusively genetic, common diseases with a Mendelian subset, polygenic complex conditions and somatic mosaic conditions
The applications of personalised medicine are numerous and exciting and are growing, but the evidence base and impact of each intervention requires thorough analysis
Every human genome contains around 3–5 million genetic variants compared with the reference sequence. Caution is therefore required in analysing genomic results and attributing causation for any given variant; expert interpretation, preferably in a multi-disciplinary setting is required
Detailed clinical information, in terms of phenotype and family structure, remains key in interpreting genetic variation
It is important that patients and clinicians do not see a negative genomic test result as a ‘clean bill of health’
The rise of genomics
Genomic medicine has the capacity to revolutionise the healthcare of an individual with a rare disease or cancer by offering prompt and accurate diagnosis, risk stratification based upon genotype and the capacity for personalised treatments.
Deciphering the genome
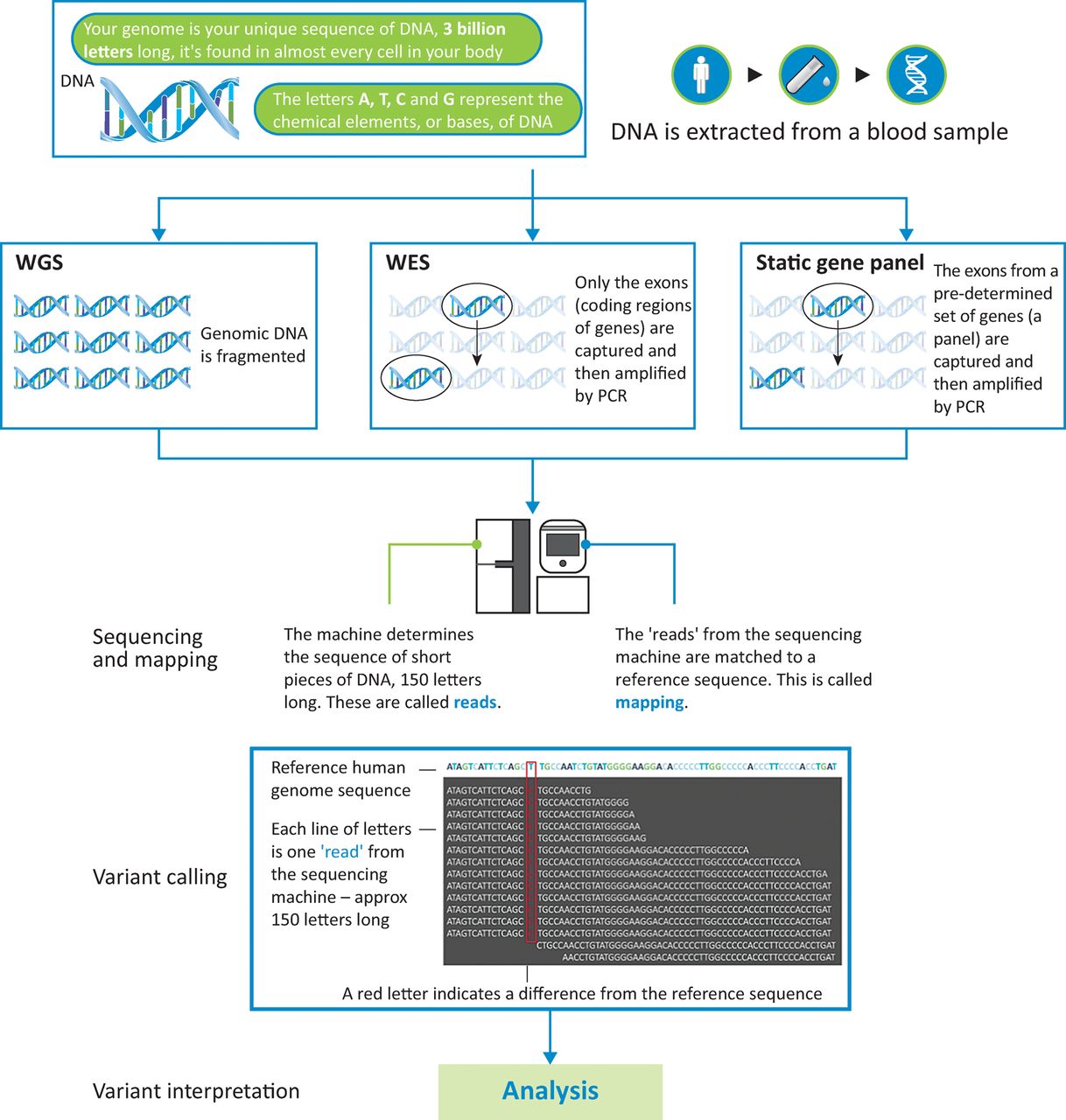
The human genome comprises in excess of 3 billion DNA base pairs.3 It was first mapped through the Human Genome Project, an extensive international collaboration over 13 years.4 Advances in sequencing technology (known as ‘next generation sequencing’) have enabled a genome to be sequenced within hours, at a fraction of the initial cost,5 resulting in widespread application for diagnosis and research. Previously, individual genes were sequenced exon by exon, using capillary electrophoresis (Sanger sequencing). Despite the speed and automation involved in the sequencing itself, considerable input is required in the interpretation of the results, meaning that clinically useful information is typically provided through diagnostic laboratories in 2–12 weeks, depending on clinical urgency. Fig 1 and Table 1 provide an overview and comparison of the approaches using newer sequencing technology: whole genome sequencing (WGS), whole exome sequencing and targeted sequencing of genes via a static ‘panel’.
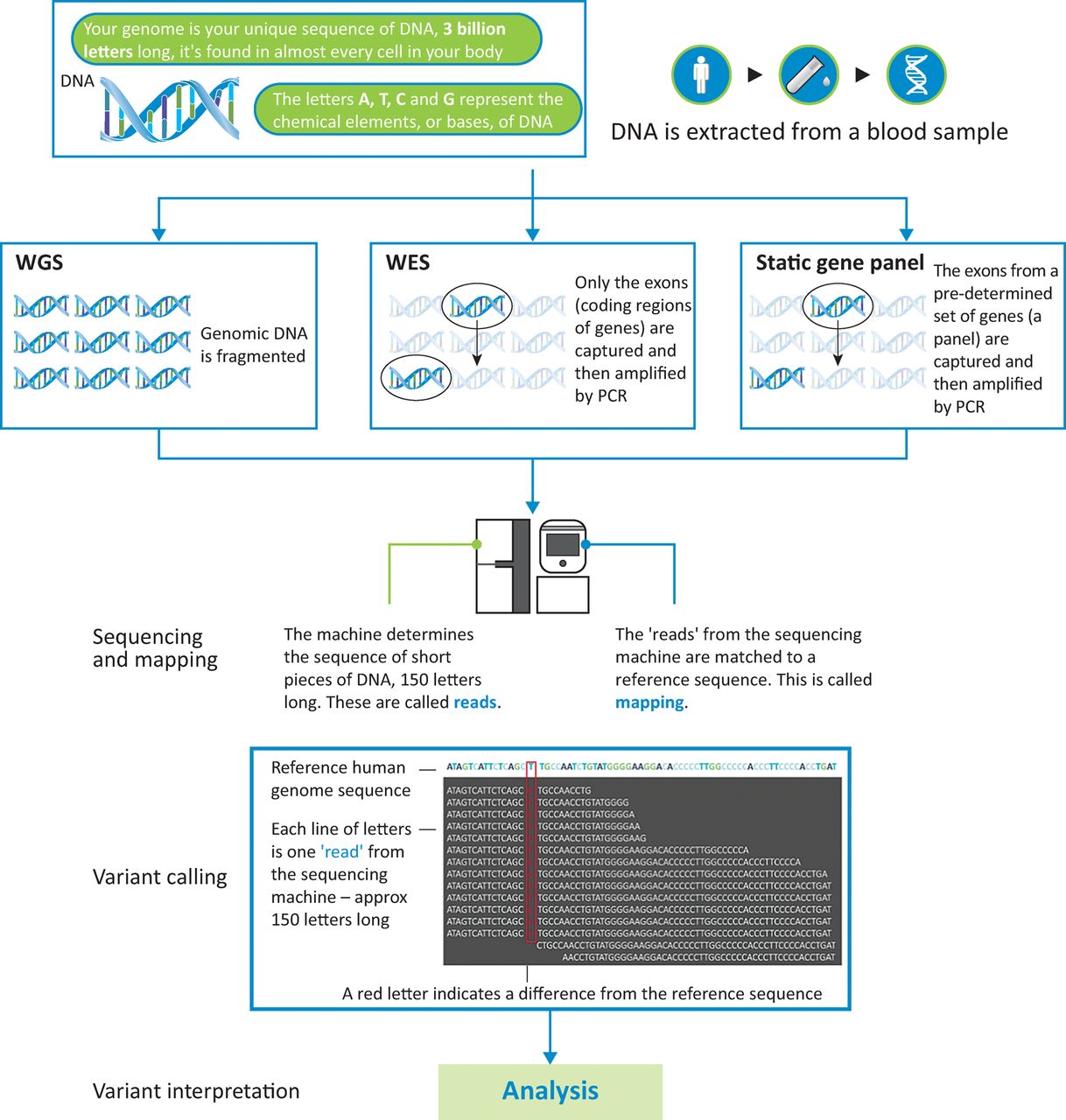
An overview of whole genome sequencing (WGS), whole exome sequencing (WES) and static gene panel techniques. Adapted from graphics provided by Genomics England.
A comparison of whole genome sequencing, whole exome sequencing and static gene panel techniques
The genome and rare disease
There are an estimated 6,000 rare diseases, each defined as affecting less than 1 in 2,000 people.6 In the UK, these cumulatively affect 3.5 million people5 equating to a 1 in 17 lifetime risk. 80% are estimated to have genetic origins.7 These include conditions with a virtually exclusive Mendelian genetic aetiology and rare Mendelian subsets within common disorders (eg familial hypercholesterolaemia). In some disorders, highly targeted genetic testing remains best, for example cystic fibrosis, which is readily identifiable clinically with a single causative gene. In an increasing number of clinical settings, broader-based genetic investigation – such as gene panels, exome sequencing and WGS – is recognised as advantageous, particularly where the phenotype is variable or non-specific and the range of plausibly causative genes is wide. Table 2 gives examples of how patients can benefit from WGS.2 In addition, WGS can detect non-coding variants that disrupt regulatory control of gene expression and potentially uncover novel disease mechanisms.
Cases reported in the NHS England Board paper demonstrating a benefit from WGS
The genome and cancer
Cancer is a genetic disease resulting from an accumulation of mutations in a particular tissue (the soma) causing uncontrolled cell division. Sequencing DNA extracted from a tumour constructs a picture of the mutational events and drivers for oncogenesis. These somatic genomic mutations can direct therapy based on likely tumour response.
Abbosh et al8 outline the potential role in sequencing circulating tumour DNA (ctDNA), which is separate from cellular DNA, to identify tumour recurrence in advance of conventional imaging modalities. This could offer a therapeutic window of opportunity and the potential to identify further mutations within the ctDNA sequence, indicating the development of chemotherapeutic resistance.
Sequencing an individual’s constitutional DNA (their germline) reveals inherited cancer predisposition syndromes, conferring considerable lifetime risk of malignancy. Many of these are heritable as autosomal dominant traits and may therefore direct treatment choices, as well as surveillance, for family members.
The genome and common disease
In time, with access to large genomic datasets, the capacity to understand complex disease predisposition through multiple small-effect genetic variants, coupled with environmental interaction, will evolve. Currently, there are very few clinical settings where testing for such variants alters management.
Communicating genomics and ethical considerations
Genomic test results have potential implications for the sequenced individual, their family and future generations. Although there is currently no single accepted approach, it is increasingly becoming standard practice to consider categorising the potential findings:
pertinent (primary) findings – those related to the original reason for the test, providing a diagnosis.
additional (secondary) findings – genetic alterations that confer the risk of another, unrelated disease. Conditions with an intervention to reduce the risk of an adverse outcome, including cancer predisposition syndromes with effective screening or surgical approaches, can be sought specifically. The American College of Medical Genetics and Genomics (ACMG) have published guidance on this.9 Patients can choose whether to receive these findings.
carrier status – findings of reproductive relevance, where risk of a specific condition is conferred upon future generations.
incidental findings – other types of information, for example identification of misattributed paternity. Management of these findings, and consideration of whether it is appropriate to feedback, should be directed by professionals experienced in genetic counselling, considering the context of the sequencing and clinical impact of any results.
For those who have no clear diagnostic-grade findings from genomic testing, it is important this is not interpreted as a ‘clean bill of health’. The negative predictive value of genomic testing is uncertain in many clinical settings, reflecting the current knowledge base, and would be expected to improve once our understanding of the phenotypic effects of an individual’s genome-wide variation gain precision. Reviewing the phenotype and potential disease mechanisms, and offering research participation, may offer additional opportunities for a genetic diagnosis.
Interpreting genomic data
Understanding variation within the human genome, to differentiate ‘normal’ from disease-causing variants, is challenging. Every human genome contains around 3–5 million genetic variants compared with the reference sequence. The vast majority of rare variants in the genome have no link to a patient’s disorder. Positive evidence needs to be sought as to the pathogenicity for any given variant, accompanied by consideration of the phenotype, family structure and inheritance pattern. Therefore, a multidisciplinary approach including clinical scientists and clinicians is recommended. UK diagnostic genetics laboratories are adopting variant classification guidelines from the ACMG.10 Accuracy is vital given the potential harm – not just for the individual, but also family members and perhaps future generations – if an inaccurate diagnosis is made.
Increasingly, large databases of genomes across different ethnic populations, from sources including GnoMAD11 and the 100,000 genomes project,12 will improve the accuracy of interpretation.
Health Education England provide a range of courses on genomics, from formal qualifications through to continuing personal and professional development modules (www.genomicseducation.hee.nhs.uk/taught-courses).
Personalised medicine
Personalised medicine represents a shift in approach from ‘one-size-fits-all’ to tailored care and targeted therapies.13 The application of new technologies, including genomics, enhances our understanding of disease and its molecular mechanisms, and therefore the capacity for personalised interventions. Increasingly, other testing modalities will contribute, including transcriptomics (RNA-based testing), metabolomics (analysing the metabolites present in an individual) and proteomics (analysing the entire complement of expressed proteins).
Prediction and prevention of disease
An important example in prediction and prevention of disease is familial hypercholesterolaemia, where heterozygous gene mutations are expected in 1:500 of the population.14 This confers a high risk of cardiovascular disease and is inherited in an autosomal dominant manner. Risk-reducing treatments have been recommended by the National Institute for Health and Care Excellence (NICE) since 2007 (Table 3). Molecular diagnosis and familial cascade testing by genotype identify those who warrant aggressive lipid-lowering therapy, representing an exciting step towards primary prevention. More families with familial hypercholesterolaemia will be identified through analysis of secondary findings from genomic tests for unrelated conditions.
Personalised interventions recommended by the National Institute for Health and Care Excellence (NICE) on the basis of genotype
Targeted therapy based on efficacy
There are long-standing examples of germline findings, such as BRCA1 and BRCA2 mutations, used in the oncological setting to predict the natural history of disease and enable individualised choice regarding risk-reduction. Increasingly, these results also direct therapeutic strategies.
The cancer, or somatic, genome can predict therapeutic response through an understanding of the molecular implications of certain mutations. For example, in malignant melanoma, the BRAF V600E mutation is common and results in constitutive activation of downstream signalling pathways,15 leading to cellular proliferation. Vemurafenib, an inhibitor of mutated BRAF, has been shown to improve overall survival and progression-free survival compared with standard therapy,15 leading to its recommendation by NICE. Table 3 summarises all NICE approvals by genotype (germline and somatic).
Development of new targeted therapies
A number of conditions have progressed through the cycle of gene discovery, pathogenesis research and development of a novel treatment, leading to clinical trials. One such example is the delineation of FGFR3 signalling pathways and mechanism of reduced bone formation in achondroplasia. This has led to phase III clinical trials for BMN11116 after promising pre-clinical and earlier phase studies,17 which suggest this treatment improves bone growth.
Pharmacogenetics to minimise the risk of adverse events
Genetic variation is already used to predict treatment response or adverse effects across a number of clinical areas. An example of this isabacavir treatment in HIV, where genotype can predict the risk of a severe adverse reaction.18 Selection of an alternative anti-retroviral drug in those at risk has been shown to be an effective strategy.
For effective application of pharmacogenetic testing, the likelihood and severity of the predicted adverse outcome must be balanced against the risk of avoiding use of an effective drug. In many cases further research is required to inform these decisions. The Clinical Pharmacogenomics Implementation Consortium19 (CPIC) are collating and curating such evidence, in a standardised format to assist with this.
Health economics impact
Individual benefits are clear regarding many of the applications described in this article. However, there are cost implications in identifying and testing the at-risk individual or population. Therefore, another essential component in the required evidence base is health economic analysis. This varies by condition, intervention and outcome; Peters et al provide an overview of the considerations in the case of monogenic diabetes.19
Conclusions
Technological advances and the dramatically reduced costs of DNA sequencing have resulted in increasing ‘mainstreaming’ of genetic testing into routine practice and the prospect of WGS becoming part of NHS diagnostics. Clinicians need to understand the role of genomic medicine in their specialty, in offering prompt and precise diagnosis for patients and in directing management decisions. Detailed clinical information and multidisciplinary input remains vital for variant interpretation.
The knowledge gained from genomics and personalised medical approaches is exciting. A number of applications are in current practice and these are likely to increase exponentially as WGS becomes embedded in routine patient care. Analysis of the evidence, from a clinical and health economic perspective, is pivotal to the ongoing success of the genomics era.
Conflicts of interest
All authors are currently working for Genomics England as part of the 100,000 Genomes Project.
Acknowledgments
The authors would like to thank Genomics England for providing a graphic regarding whole genome sequencing that was used to produce Fig 1.
- © Royal College of Physicians 2017. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- Genome-Wide Exploration of the Opportunistic Providencia stuartii Unveils the Novel Genetic Interactions with the Virulence Gene of Diarrheal Pathogens
- PhenoScore: AI-based phenomics to quantify rare disease and genetic variation
- Can we know if donor trust expires? About trust relationships and time in the context of open consent for future data use