
A 68-year-old woman presented with dyspnoea, having recently been diagnosed with multiple myeloma. She was reviewed in the cardiology clinic and an echocardiogram performed, revealing moderate concentric pseudo hypertrophy with sub endocardial signal hyperechogenicity consistent with infiltration. Although the left ventricular ejection fraction was normal, significant diastolic dysfunction was identified. All these echocardiographic findings are in keeping with cardiac amyloidosis. Brain natriuretic peptide level was 293.8 pg/mL. Troponin I was raised at 0.2 μg/L (normal value <0.04 μg/L). A non-gated, contrast-enhanced venous-phase, computed tomography (CT) scan (undertaken as a myeloma staging scan) showed an extensive low density area in the sub endocardial layer of the left ventricle. This was associated with a small pericardial effusion and bilateral pleural effusions (Fig 1).
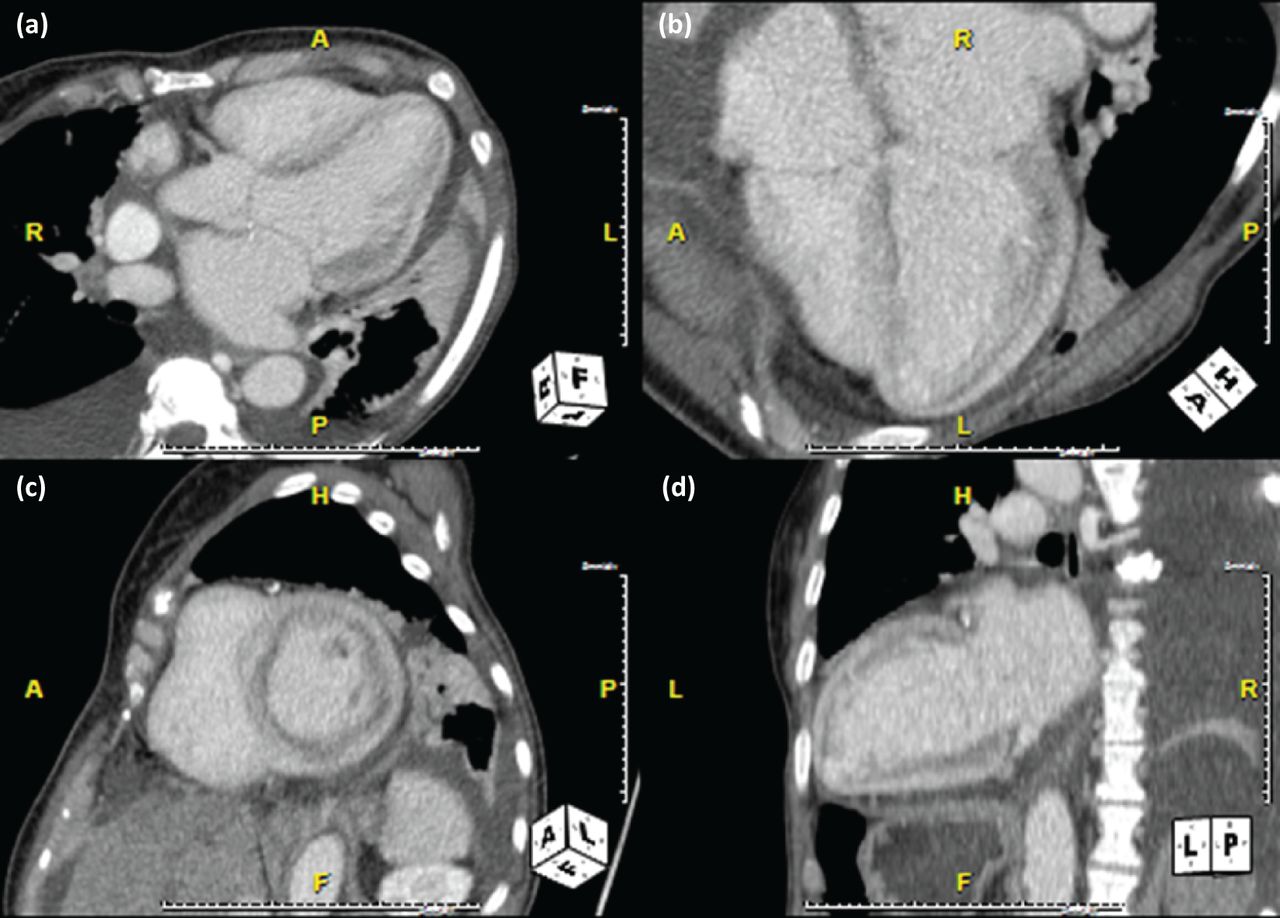
Cross-sectional contrast CT (computed tomography) image showing left ventricular sub-endocardial hypodensity. (a) Axial plane. (b) 4-chamber view. (c) Short-axis view. (d) Long-axis view.
Given the clinical history and echocardiographic features, a diagnosis of cardiac amyloidosis was presumed, and urgent admission was arranged for inpatient chemotherapy. Examination revealed significant features of right-sided heart failure with a raised jugular venous pulse and bilateral pitting oedema to the knees. An electrocardiogram (ECG) on admission showed a ventricular tachycardia which was treated with amiodarone. On the second day of admission, the patient developed a junctional rhythm and then a progressively increasingly broad complex ventricular escape rhythm and a permanent pacemaker was inserted. Unfortunately, post pacemaker insertion she developed a pulseless electrical activity (PEA) cardiac arrest from which she could not be resuscitated. No pericardial effusion or pneumothorax was identified post pacemaker insertion.
Cardiac amyloidosis is associated with significant morbidity and mortality and is the most common cause of restrictive cardiomyopathy.1 Cardiac MRI and transthoracic echocardiography are the modalities of choice for evaluating cardiac amyloidosis.2 A characteristic pattern of diffuse heterogenous subendocardial increased signal is well described in cardiac MRI,3 and ‘late enhancement’ on gated cardiac CT has also been reported.4 However, this similar finding of low-density material in the subendocardial layer on a non-gated CT is a novel finding. Given the widespread use of CT assessment in patients being considered for transcatheter aortic valve insertion (TAVI), this feature may be useful in highlighting potential amyloidosis in this population.
Consent to publish
Consent to publish was obtained from the patient's next of kin.
Acknowledgments
The authors would like to acknowledge the assistance of Dr Niall Moore for his assistance in reporting the original CT scan.
- © Royal College of Physicians 2018. All rights reserved.








{kind=link}
Related Articles
Cited By...
- No citing articles found.