
Article Figures & Data
Figures
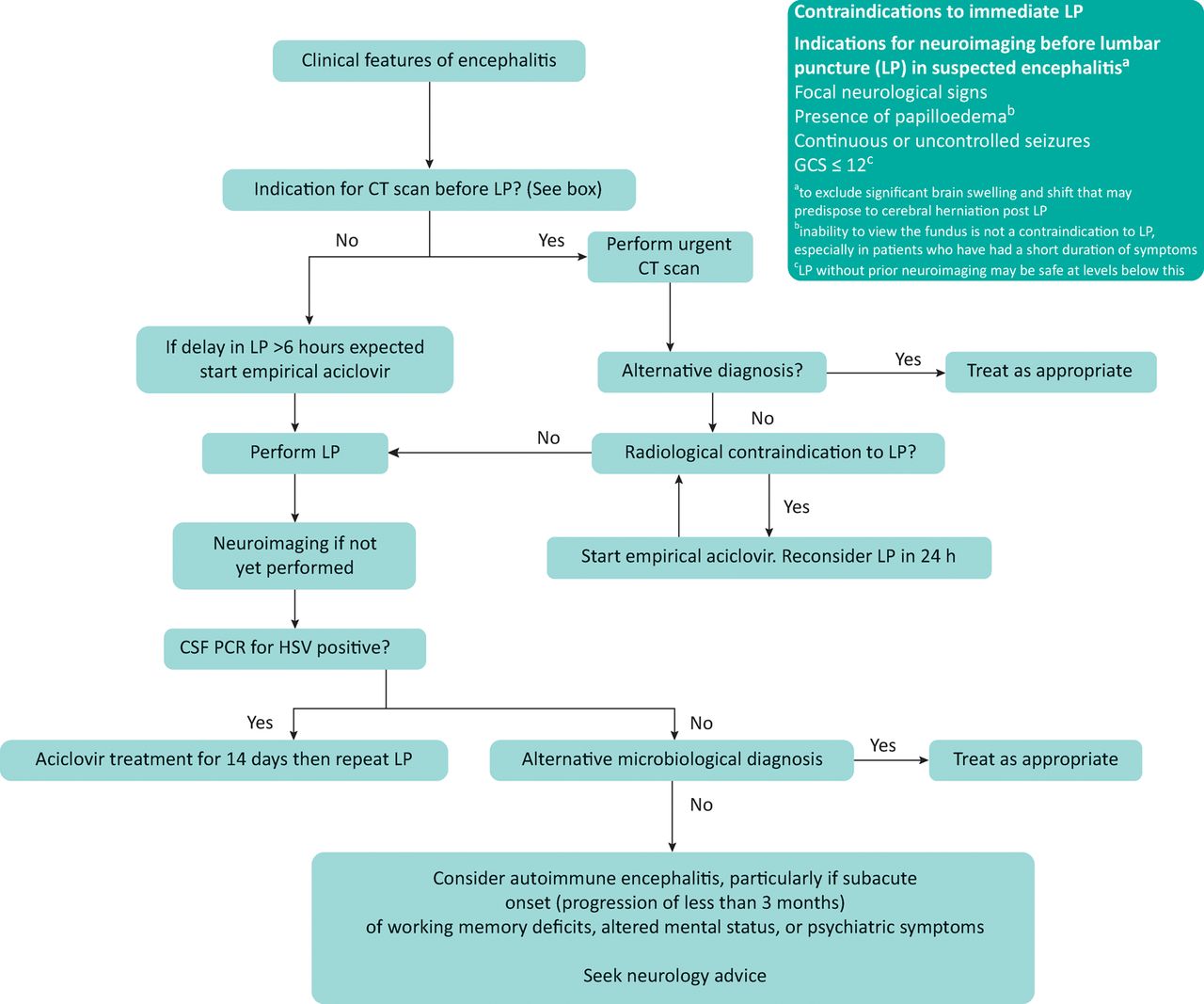
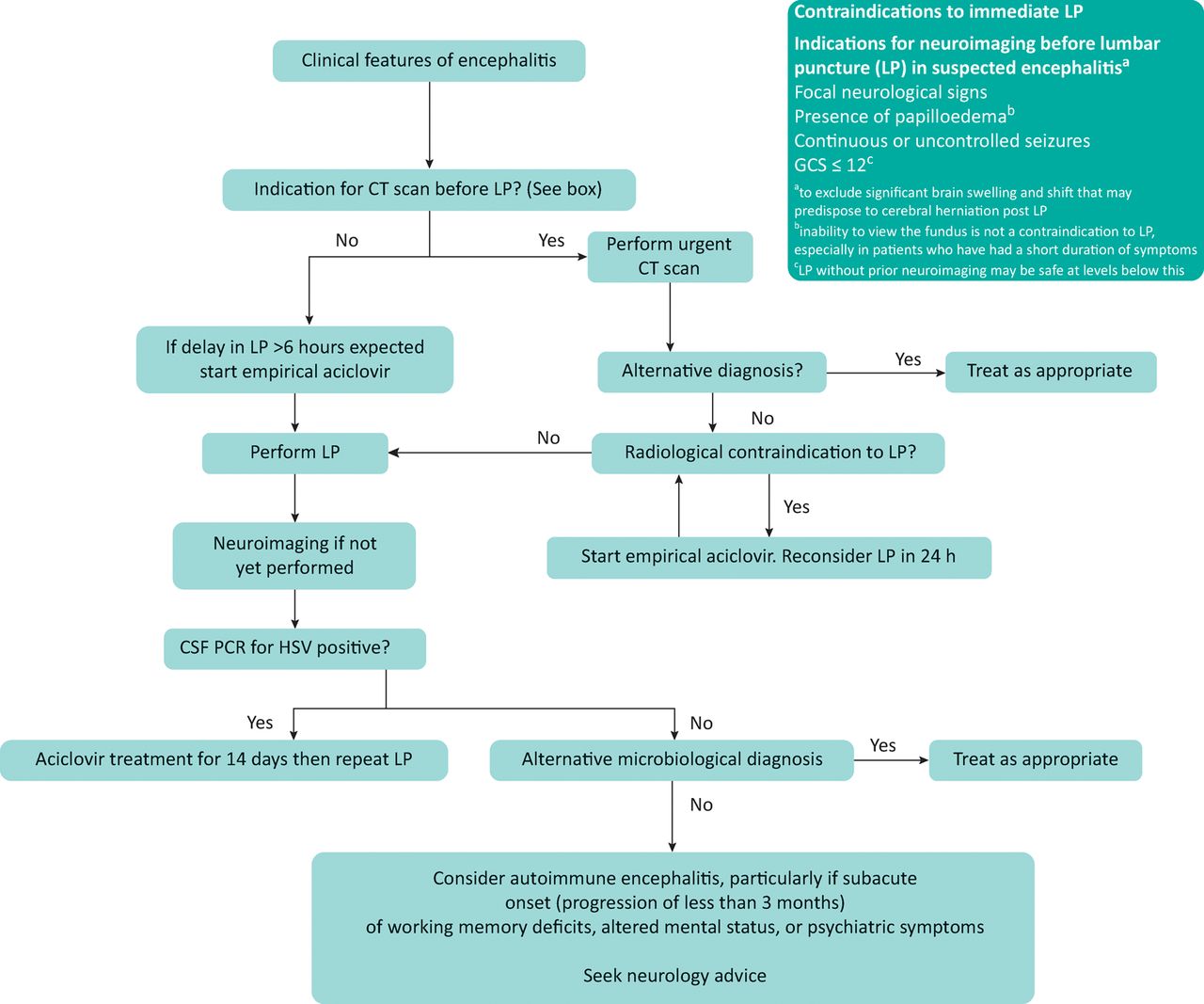
- Fig 1.
Algorithm for basic management of acute encephalitis (based on UK guidelines).6 CSF = cerebrospinal fluid; GCS = Glasgow Coma Scale; HSV = herpes simplex virus; LP = lumbar puncture; VZV = varicella zoster virus
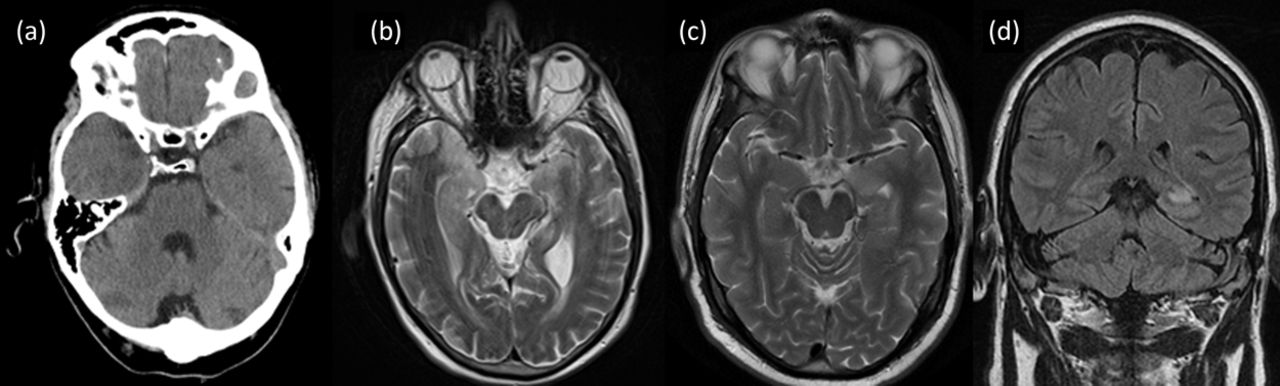
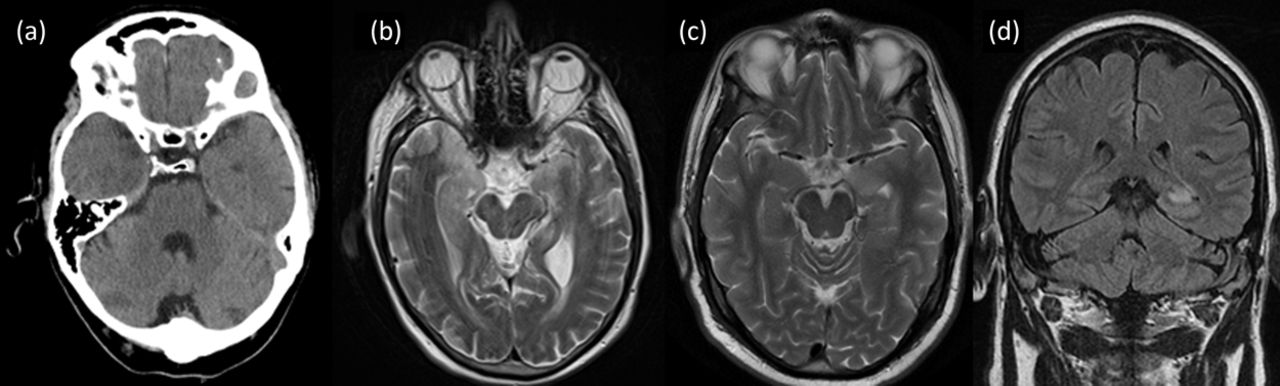
- Fig 2.
Brain imaging in encephalitis. (a) CT scan of 69-year-old male with acute HSV-1 encephalitis showing low intensity area in right temporal lobe. (b) T2 weighted axial MRI from same patient showing bilateral asymmetrical signal abnormality in medial temporal lobes. (c) T2 weighted axial MRI of 55-year-old male with LGI-1 antibody encephalitis showing high signal in the left medial temporal lobe. (d) Coronal T2 FLAIR from same patient showing high signal in left medial temporal lobe. CT = computed tomography; FLAIR = fluid attenuation inversion recovery; HSV = herpes simplex virus; LGI-1 = leucin-rich glioma inactivated 1; MRI = magnetic resonance imaging
Tables
Encephalopathy = (altered consciousness persisting for longer than 24 h, including lethargy, irritability or a change in personality or behaviour) Encephalitis = encephalopathy AND evidence of CNS inflammation, demonstrated by at least two of: fever
seizures or focal neurological findings attributable to the brain parenchyma
CSF pleocytosis (more than 4 white cells per μL)
EEG findings suggestive of encephalitis
neuroimaging findings suggestive of encephalitis.
CNS = central nervous system; CSF = cerebrospinal fluid; EEG = electroencephalography
Causes: Viral: Herpes simplex virus types 1 and 2, varicella zoster virus, enteroviruses, adenovirus, parechovirus, measles virus, HIV Autoimmune (main tumour associations in brackets): Antibodies against neuronal surface antigens: NMDAR antibody encephalitis (ovarian teratoma), LGI-1 antibody encephalitis (thymoma), antibodies against intracellular antigens: anti-Hu (small cell lung tumour), anti-Ma (testicular tumours), anti-GAD, acute disseminated encephalomyelitis, Bickerstaff's encephalitis Mimics: Infective: Systemic sepsis with encephalopathy, bacterial meningitis, TB, opportunistic infections in immunocompromised patients (eg crytococcus, toxoplasma, cytomegalovirus) Inflammatory: Vasculitis, systemic lupus erythematosus with CNS involvement, Behçet's disease, neurosarcoidosis Metabolic: Hypoglycaemia, hyponatraemia, hepatic encephalopathy, toxins (drugs, alcohol) Neoplastic: Primary brain tumour (particularly low grade glioma mimicking CNS inflammation), metastases Others: Status epilepticus from other causes, haemorrhagic or ischaemic stroke, psychiatric disease CNS = central nervous system; GAD = glutamic acid decarboxylase; LGI-1 = leucin-rich glioma inactivated 1; NMDAR = N-methyl D-aspartate receptor; TB = tuberculosis








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Unpacking the CNS Manifestations of Epstein-Barr Virus: An Imaging Perspective
- Diagnosis of delirium: a practical approach
- Diagnosis of delirium: a practical approach
- Encephalitis: diagnosis, management and recent advances in the field of encephalitides
- COVID-19 encephalopathy: an unusual presentation with new-onset seizure causing convulsive status epilepticus
- Diagnosis and analysis of unexplained cases of childhood encephalitis in Australia using metagenomic next-generation sequencing
- Comment on CME Infectious diseases