
ABSTRACT
The syndrome of pyrexia of unknown origin (PUO) was first defined in 1961 but remains a clinical challenge for many physicians. Different subgroups with PUO have been suggested, each requiring different investigative strategies: classical, nosocomial, neutropenic and HIV-related. This could be expanded to include the elderly as a fifth group. The causes are broadly divided into four groups: infective, inflammatory, neoplastic and miscellaneous. Increasing early use of positron emission tomography–computed tomography (PET-CT) and the development of new molecular and serological tests for infection have improved diagnostic capability, but up to 50% of patients still have no cause found despite adequate investigations. Reassuringly, the cohort of undiagnosed patients has a good prognosis. In this article we review the possible aetiologies of PUO and present a systematic clinical approach to investigation and management of patients, recommending potential second-line investigations when the aetiology is unclear.
Key points
When investigating a patient with pyrexia of unknown origin (PUO), consider possible aetiologies in each of the following four broad categories: infective, inflammatory, neoplastic and miscellaneous. Address each in turn. Pyrexia of unknown origin is a diagnostic challenge and early involvement of specialists is important
The balance of causes of PUO varies over time and across different patient populations
Investigations should be undertaken based on the most likely cause(s). Blanket investigations are not recommended as positive or equivocal tests are difficult to interpret in the absence of a suggestive exposure history and/or clinical syndrome. This can be misleading and potentially cause patient harm
Empirical therapeutic trials are not recommended before a diagnosis is made, unless the patient is believed to have miliary tuberculosis (TB), central nervous system TB, temporal arteritis or infective endocarditis with severe sepsis
The overall outcome of patients with a PUO is good, especially when no cause is found
Introduction
The definition of pyrexia of unknown origin (PUO) dates back to 1961; it was described as a persistent fever above 38.3°C (100°F) that evades diagnosis for at least 3 weeks, including 1 week of investigation in hospital.1 This definition has evolved with faster and more accurate diagnostic techniques and changing models of care, and a week of hospitalisation is no longer considered essential. Different subgroups with PUO have been suggested, each requiring different investigative strategies: classical, nosocomial, neutropenic and HIV-related.2 Pyrexia of unknown origin in the elderly tends to be considered under the classical heading, but the presentation, underlying conditions and subsequent management differ considerably from PUO in a younger adult age group. Pyrexia of unknown origin in the over 65s could be considered a fifth category.3,4
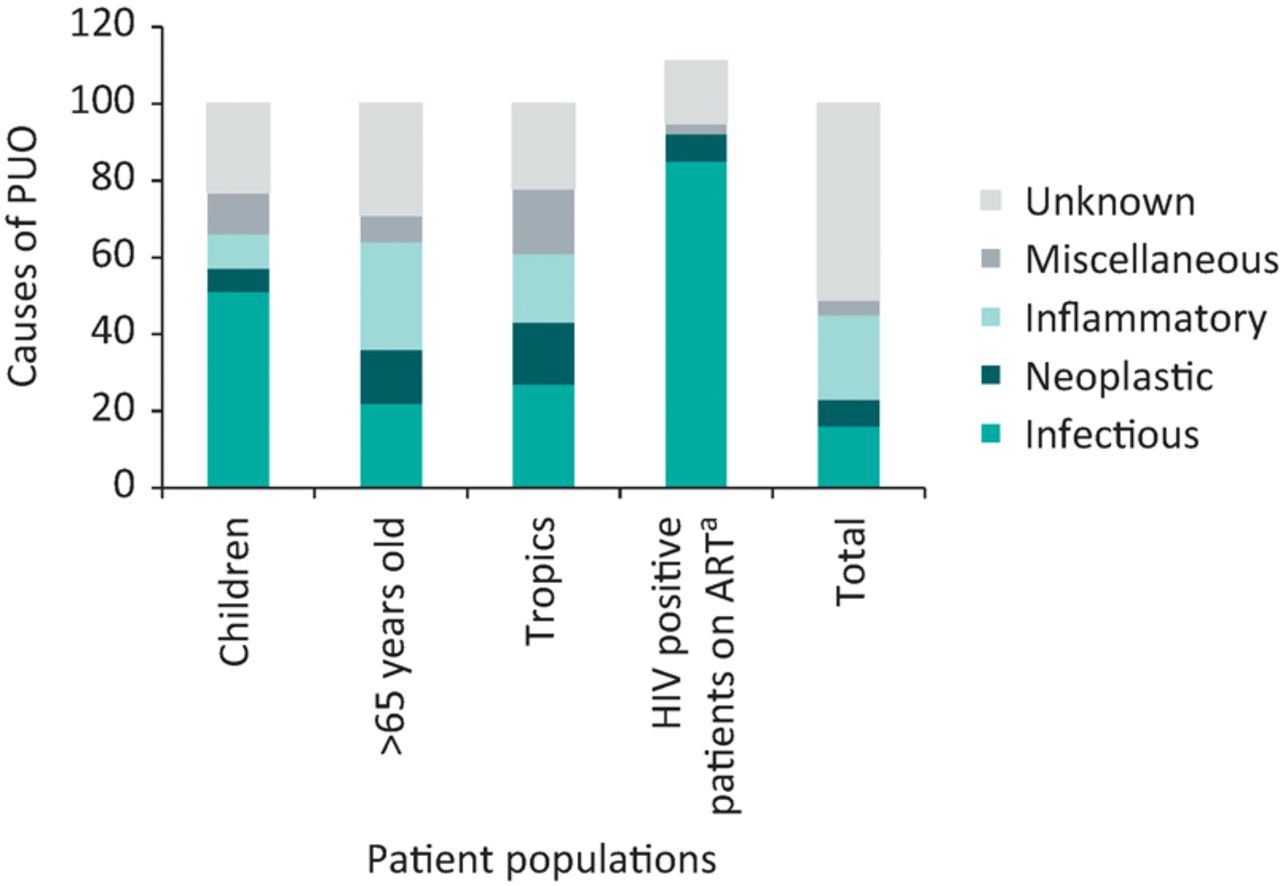
The causes of PUO can be considered in four categories: infective, inflammatory, neoplastic and miscellaneous. The relative prominence of each category has changed over time, with an increasing proportion of patients who remain undiagnosed, which may be up to 51% of cases.5 Infectious causes account for 17–35% of cases, inflammatory causes 24–36%, neoplastic causes 10–20% and miscellaneous causes 3–15%.6 An older multimorbid population, increased global travel, HIV infection, the increase in organ transplantation and immunomodulation for many diseases, evolving diagnostics and changing antimicrobial resistance patterns have all changed the management of patients with PUO (Fig 1).

The relative causes of pyrexia of unknown origin (PUO) in different patient populations expressed as percentages (data from references5,7–11). aMany HIV positive patients have more than one causal diagnosis for PUO and therefore the sum of percentages in this category is >100%. ART = antiretroviral therapy
Clinical approach
The diagnostic approach to a patient with PUO should be methodical. A thorough history is essential and will have to go back months or years to yield clues to potential aetiologies for investigation. The pattern of fever (episodic, consistent etc) and general health of the patient during and between episodes of fever should be ascertained, together with any associated past or current symptoms. Enquiry should include a detailed past medical and surgical history, all medications the patient takes or has taken including over-the-counter drugs, alternative, herbal or ‘traditional’ medications, recreational drug use and vaccinations. A comprehensive travel history is needed together with occupational, environmental, animal and sexual exposures. Illness in contacts and a family history of similar illnesses may be relevant. This history should be revisited at regular intervals, both to highlight clues that were previously missed or initially not considered to be relevant and to review any changes in symptoms.
Patients with a prolonged PUO are often clinically well enough to lead a relatively normal life. However, at every clinical encounter it must be reviewed whether the patient has developed any ‘red flag’ symptoms; these include weight loss, increased lethargy, drenching night sweats, inability to perform activities of daily living, or changes in other symptomatology and physical examination.
A comprehensive examination of the patient follows. The first clinical encounter should include an ‘A, B, C’ approach to ensure the patient is clinically stable. Physical features of a systemic inflammatory response must be elucidated on examination and in the first instance sepsis should be ruled out.
As well as a detailed examination of the respiratory, cardiovascular and alimentary systems one must pay special attention to other important sources of fever. This includes: full examination of the spine and joints; top-to-toe examination of the skin for rashes, ulcers, scars, bites, pressure areas and abnormalities of the hair and nails; review of dentition; temporal arteries; fundoscopy; breast examination, particularly in women; and pelvic or rectal examination including the prostate in men. Any implant is a potential site of infection and must be examined if possible, including prosthetic joints, pacemakers, pacemaker wires, central or peripheral vascular lines, shunts, grafts and meshes.
Investigations should be conducted to confirm or rule out the most likely diagnosis/diagnoses, based on the history and examination findings. Investigation should proceed through at least two stages of baseline tests followed by more specific tests, after which each abnormal result should be weighed carefully – the more tests that are done, the more false leads will emerge. Early blanket testing for all possible aetiologies is inappropriate. A baseline set of investigations includes full blood count with a differential cell count, renal electrolytes and liver function tests, C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR), clotting screen, creatine kinase, at least two blood cultures (while not receiving antibiotics) and an HIV test. A chest X-ray, ultrasound of the abdomen and a urine dipstick should also be performed.
Potential second-line investigations include microbiological tests, imaging and biopsies as described in Table 1. Each test should only be performed when there is a reasonable pretest probability of the condition being present and this often requires early involvement of other appropriate clinical specialties in the care of patients with PUO. The utility and availability of positron emission tomography–computed tomography (PET-CT) has increased and it is often used early in the list of second-line investigations to identify metabolically active foci of infection, inflammation or cancer as possible causes of PUO.12
Potential second-line investigations for pyrexia of unknown origin
Infective causes
The most common causes of PUO in immunocompetent individuals are infective endocarditis (especially culture negative endocarditis), discitis, osteomyelitis, occult abscesses and infected implanted devices. Patients who have been hospitalised in the last 6 months are at increased risk of haematogenous spread of infections through invasive procedures and intravascular devices. In all cases, a positive microbiological diagnosis should be attempted prior to commencing antimicrobial therapy, often involving a biopsy of the potentially infected tissue or removal of the culprit device. In patients with suspected endocarditis and negative blood cultures, fastidious and slow-growing bacteria are common aetiological agents. In these cases, extended cultures for HACEK organisms (a group of fastidious Haemophilus-like organisms) and serology for Coxiella burnetii (Q fever), Bartonella spp and Brucella spp are recommended.13
Resistant organisms are becoming increasingly common and must be considered in patients with recent (last 6 months) or repeated hospitalisations, who have received repeated courses of antimicrobials, and those who have been travelling abroad, especially if they have had diarrhoea or been hospitalised overseas.
Elderly patients account for an increasing proportion of patients with PUO. It is important to not discount diagnoses such as tuberculosis, HIV or syphilis on the basis of age alone.
Returning travellers
Up to one-quarter of returning travellers cite fever as the chief reason for seeking care on return and are more likely to be hospitalised than those without fever.14,15 The National Travel Health Network and Centre (NaTHNaC) (https://travelhealthpro.org.uk) provides travel information about current outbreaks and potential exposures based on the area of travel.
A travel history should elicit where the patient has returned from (including transits), the length of time spent in each place, the type of accommodation used, use of bed nets, the activities the patient undertook, what type of food and beverages they consumed, and whether they suffered any arthropod or animal bites. Details are needed of business and leisure activities including animal and freshwater contact, sexual history and possible illness in contacts. Vaccinations prior to travel, compliance with malaria and other chemoprophylaxis and the use of antimicrobials abroad are also important. Most patients with falciparum malaria present within 2 months of return, but other species of malaria may have incubation periods of a year or more, so travel history should extend back for at least 2 years.16 Patients visiting friends and relatives abroad are at increased risk of infections such as typhoid and malaria and are also more likely to suffer other serious preventable travel-related illnesses compared to other travellers. Infections that may present months to years after exposure, such as tuberculosis (TB), need to be considered and are more likely in areas with large migrant populations. Systematic approaches to investigating fever in the returning traveller are published in more detail elsewhere.17
It is important to consider less exotic causes for a fever in returning travellers such as urinary tract infections, influenza, pneumonia, meningitis and non-infectious conditions, especially deep venous thrombosis and pulmonary embolism.
Immunosuppressed patients
Immunosuppression can be caused by numerous conditions and related medications including HIV infection, haematological malignancies, organ transplantation, corticosteroids, immunomodulators and chemotherapy agents.
Pyrexia of unknown origin in patients with HIV infection can be caused by HIV seroconversion, opportunistic infections at low CD4 cell count levels (especially <200x106 cells/L), malignancies at all CD4 count levels, and immune reconstitution inflammatory syndrome (IRIS) after commencing antiretroviral therapy. Patients living with HIV often have a high epidemiological risk for infections such as TB, invasive non-typhoidal salmonellosis and malaria, which can occur at any CD4 count but may present atypically in these patients.
The risk of immunosuppression in transplant recipients is determined by the underlying medical condition which necessitated transplant, the duration and type of drug-induced immunosuppression pre- and post-transplant, and their comorbidities. Acute and chronic transplant rejection can also cause fever, the management of which may necessitate further immunosuppression.
Infections in immunosuppressed patients present atypically, with altered incubation periods, attenuated or more severe clinical signs and symptoms, and differing yields from diagnostic tests. It is not uncommon for immunosuppressed patients to have more than one life-threatening infection.
Immunosuppressed patients have an increased incidence of the infections which may present as PUO, especially:
bacterial: pulmonary and extrapulmonary TB, other mycobacterial infections, non-typhoidal salmonellosis, melioidosis, and syphilis
viral: arboviruses, Coxsackie virus, cytomegalovirus (CMV), Epstein–Barr virus (EBV), and parvovirus
fungal: aspergillosis, candidiasis, cryptococcosis, endemic mycoses, and histoplasmosis
parasitic: visceral leishmaniasis.
Non-infective causes
The non-infectious causes of PUO can be broadly categorised as inflammatory disorders, solid tumours, haematological malignancies and miscellaneous (Table 2⇓). As the relative incidence of infective causes of PUO decreases, non-infective causes are becoming more prevalent and can account for up to one-third of PUO cases.5,7
Non-infective causes of pyrexia of unknown origin
Numerous inflammatory disorders can cause fever, such as systemic rheumatic diseases (eg polymyositis), vasculitic processes (eg temporal arteritis), autoinflammatory disorders (eg Still's disease) or granulomatous processes (eg sarcoidosis). These are often multisystem conditions requiring multiple confirmatory investigations and a multidisciplinary approach to management.
Fever associated with malignancy may be due to the malignant process itself or an associated paraneoplastic process, as well as opportunistic infections. Criteria for diagnosis of malignancy related PUO, including a selective response to naproxen, have been summarised elsewhere.18
Drug fever is an under-recognised cause of PUO, particularly in the elderly. It usually commences 7–10 days after starting a medication but can occur at any time, including months later. If fever persists for more than 96 hours after its discontinuation, the suspected drug is unlikely to be the cause.4 Many classes of medications can cause fever through different mechanisms including antibiotics, anticholinergics, non-steroidals, allopurinol, anticonvulsants, anti-hypertensives, antiarrhythmics, and antidepressants.
There are many rare conditions in the miscellaneous causes of PUO, some of the most common of which are listed in Table 2. It is essential to consider factitious (self-induced) fever, especially in patients with good medical knowledge and apparently good health despite wide-swinging fever patterns.19
Management
The management of PUO should be supportive until the cause has been determined. Therapeutic trials of antimicrobials or steroids are not recommended because they can mask symptoms and signs of the underlying disease process. The overall mortality of PUO is low, particularly in those well enough to be investigated as outpatients.20 Box 1 lists good practice points in the management of patients with PUO.
Good practice points in the management of pyrexia of unknown origin
There are three occasions when empirical treatment is appropriate: antituberculous therapy for suspected miliary or CNS TB, antimicrobials for patients with suspected infective endocarditis and signs of sepsis, and steroid treatment for possible temporal arteritis. Empirical treatment for TB should always be discussed with a specialist, as the risk of drug resistance needs to be evaluated for each patient, together with the need for early adjunctive steroid therapy for CNS and pericardial TB (at differing dosing regimens).
One of the most important aspects of management is to address the patient's expectations of diagnosis and treatment. It is important to warn them about the need for a methodical stepwise approach to investigation, which can be frustrating for both the patient and physician and which may not lead to a firm diagnosis. Undiagnosed patients may be reassured that their prognosis is likely to be good, despite possible continuation of symptoms.
Acknowledgment
NJB is partially supported by the National Institute of Health Research Health Protection Unit in Emerging and Zoonotic Infections, a collaboration between the University of Liverpool, Liverpool School of Tropical Medicine and Public Health England. He is affiliated with the Liverpool School of Tropical Medicine. Views expressed in this article are those of the contributors and do not necessarily represent the official position of the National Health Service, the National Institute for Health Research, the Department of Health, or Public Health England.
- © Royal College of Physicians 2018. All rights reserved.








{kind=link}